


Abstract
Objectives: To test the effect of preoperative mannitol infusion on perioperative decreased cerebral oxygen saturation (rSO2) during laparoscopic cholecystectomy.
Methods: Forty patients scheduled for laparoscopic cholecystectomy were enrolled in this study conducted at Dammam Hospital of the University, Dammam, Kingdom of Saudi Arabia from December 2013 to June 2014. Patients received either 0.5 g/kg of 20% intravenous mannitol infusion over 10 minutes before induction of anesthesia (group M), or an equal volume of normal saline instead (group C). Primary outcome variable was rSO2. Other variables included extubation time, clinical assessment of consciousness recovery using the Modified Observer’s Assessment of Alertness/Sedation Scale (OAA/S), and the mini-mental state examination (MMSE) for cognitive evaluation.
Results: Anesthesia induction increased rSO2 in both groups. Pneumoperitoneum decreased rSO2 in group C, but not in group M. This drop in rSO2 in the group C reached its maximum 30 minutes after extubation, and was significantly less than the preinduction value. Time to extubation in group M was significantly shorter compared to group C (p=0.007). The OAAS in group M at 10 min after extubation was significantly higher compared to group C. No differences were found between the 2 groups in cognitive function as measured by MMSE score.
Conclusion: Preoperative mannitol infusion maintains perioperative rSO2 during laparoscopic cholecystectomy and shortens extubation time with earlier resurgence of OAAS.
Intracranial pressure (ICP) is elevated during pneumoperitoneum due to impedance of venous return from the lumbar venous plexus,1 and increased cerebral blood flow resulting from hypercarbia and catecholamine release.2,3 Elevated ICP may lead to adverse CNS outcomes in the form of late recovery, deterioration in cognitive function, deficit in memory, or seizures. The incidence of these complications varies according to duration of surgery, co-morbidities, and age.4,5 Previous reports showed decreased cerebral oxygen saturation (rSO2) as cerebral perfusion pressure declines because of increased ICP.6-8 Mannitol is a long-established osmotic diuretic. It decreases ICP by decreasing the overall water content, cerebrospinal fluid volume, and blood volume.9,10 Mannitol improves cerebral perfusion, microcirculation, and hence, cerebral oxygenation by decreasing blood viscosity. As a free radical scavenger, mannitol also exerts a protective effect on nerve cell membranes against biochemical injury through inhibition of their lipid peroxidation.11,12 The aim of this study was to test, whether mannitol infusion before anesthetic induction for laparoscopic surgery would improve rSO2 and enhance recovery. We hypothesized that infusion of 0.5 g/kg of 20% mannitol, immediately before induction of anesthesia for laparoscopic surgery, improves rSO2, shortens patients’ recovery time, and improves recovery quality, as well as postoperative cognitive function.
Methods
“Anesthesia, cerebral, oximetry, mannitol, laparoscope, cholecystectomy” as keywords was entered into Google® search engine (http://www.google.com/) to identify related information in the public domain. Top 50 hits of the search results were reviewed carefully to identify articles from peer-reviewed journals to be carefully read. The study was approved by the ethics committee of the University of Dammam, Dammam, Kingdom of Saudi Arabia, and was carried out according to principles of Helsinki Declaration. A written informed consent was obtained from 40 patients scheduled for laparoscopic cholecystectomy at Dammam Hospital of the University, Saudi Arabia from December 2013 to June 2014, and was enrolled in this double blind, randomized controlled study. Inclusion criteria included patients classified as American Society of Anesthesiologists (ASA) physical status I or II, aged between 25 and 50 years, and with a body mass index (BMI) between 22-34 kg/m2. Exclusion criteria were significant obstructive or restrictive pulmonary disease, and significant cardiac dysfunction. Patients were randomly assigned into 2 equal groups using an online research randomizer (www.randomizer.org). The first group received 0.5 g/kg of 20% intravenous (i. v) mannitol infusion over 10 minutes immediately before the induction of anesthesia (group M), while the second group received an equal volume of 0.9% normal saline (group C) by an anesthetist not involved in data collection. Ringer’s lactate solution was infused during operation at a rate of 6 ml/kg/h. A standardized anesthetic regimen was used. General anesthesia was induced with propofol (2 mg/kg) and fentanyl (2 µg/kg). Orotracheal intubation was facilitated with rocuronium 0.6 mg/kg. A train of 4 responses to ulnar nerve stimulation was monitored by a peripheral nerve stimulator (GE Healthcare Finland Oy, Type E-NMT-00, Helsinki, Finland). If a visible T2 response appeared, a bolus of rocuronium 10 mg was administered. Anesthesia was maintained with sevoflurane to maintain an adequate anesthetic depth as indicated by a bispectral index (BIS) value of 45-60. Further fentanyl boluses of 1 µg/kg were given in response to a heart rate >20% of baseline value. Electrocardiogram and pulse oximetry (Datex-Ohmeda, WI, USA) were continuously monitored during surgery. Nasopharyngeal temperature was continuously monitored and maintained above 36.5°C using a forced air warmer (Bair Hugger, Arizant Healthcare, Eden Prairie, MN, USA) and warming of infused fluids. Cerebral regional oxygen saturation was continuously monitored using near infrared spectroscopy (NIRS) (INVOS 3100A, Somanetics Corporation, Troy, MI, USA). After the induction of anesthesia, a single NIRS sensor was placed on the right side of the patient’s forehead, with the caudad border approximately 1 cm above the eyebrow, with the medial edge at the midline according to the manufacturer’s guidelines. Mechanical ventilation was achieved with Datex-Ohmeda ventilator, Bromma, Sweden. Set inspiratory pressure was manipulated to achieve a tidal volume (VT) of 8 ml/kg/h during surgery with accepted variation of <5%. Respiratory rate (RR) was also manipulated to keep an end tidal carbon dioxide tension (EtCO2) of 35-40 mm Hg. At the end of skin closure, anesthesia was discontinued, residual neuromuscular block was reversed with neostigmine 0.05 mg/kg and glycopyrrolate 0.008 mg/kg, and patients were left until spontaneous breathing resumed. Tracheal extubation was carried out when patients were able to maintain VT of 6-8 mL/kg, RR >12/min, and can open their eyes. Time elapsed from cessation of anesthetics to extubation was registered. The primary outcome variable (rSO2) and mean arterial pressure (MAP) were recorded at the following points: T1 - before induction room air; T2 - before insufflation with FiO2 50%; T3 - 20 min after insufflations with fraction of inspired oxygen (FiO2) 50%; T4 - after desufflation with FiO2 50%; T5 - 30 min after extubation; and T6 - 60 min after extubation on room air. All measurements were obtained in 30° anti-Trendelenburg’s position. Similarly, ETCO2 was recorded before insufflation, 20 min after insufflation, and after desufflation. Other secondary outcomes included extubation time, clinical assessment of recovery of consciousness using the modified Observer’s Assessment of Alertness/Sedation Scale (OAA/S)13 and the Mini-mental State Examination (MMSE) for cognitive assessment.14 To minimize potential observer bias, a single investigator blinded to group allocation performed all OAA/S and MMSE score assessments. When the MMSE score is 2 points lower than the preoperative, patients were considered to have a decline in cognitive function.15 The MMSE score was evaluated 30 min preoperatively and one hour after extubation, while the OAA/S was evaluated at 10, 20, and 30 min after extubation.
Power analysis was based on the t-test of a pilot study of 10 patients that showed an average rSO2 after peritoneal insufflation of 60 ± 10 (mean ± standard deviation [SD]). Sixteen patients were required in each group to have a 90% chance to detect a 20% difference of rSO2 between the 2 groups at the 5% level of significance. To compensate for dropout cases and lack of normality in data distribution, we studied 20 cases in each group. Parametric data were expressed as the mean ± SD in text, and mean ± 95% confidence intervals in graphs. Nonparametric data were expressed as median and interquartile range. Data were tested for normality using the Kolmogorov-Smirnov test. Extubation time and demographic data except gender were compared using Student’s t-test. Gender distribution was compared between the 2 groups using Fisher’s exact test. Two-way repeated measure analysis of variance was used for continuous parametric variables as rSO2, MAP, and ETCO2, and the differences were then calculated by post hoc testing (Newman-Keuls test). Friedman repeated measures analysis of variance followed by Newman-Keuls test were used for within-group comparison of nonparametric variables, such as OAA/S and MMSE score, and Mann-Whitney rank-sum test for comparison of values between groups. Analysis was performed using Statistica software version 7.0 for Windows (Statsoft, Chicago, IL, USA). A p≤0.05 was considered significant.
Results
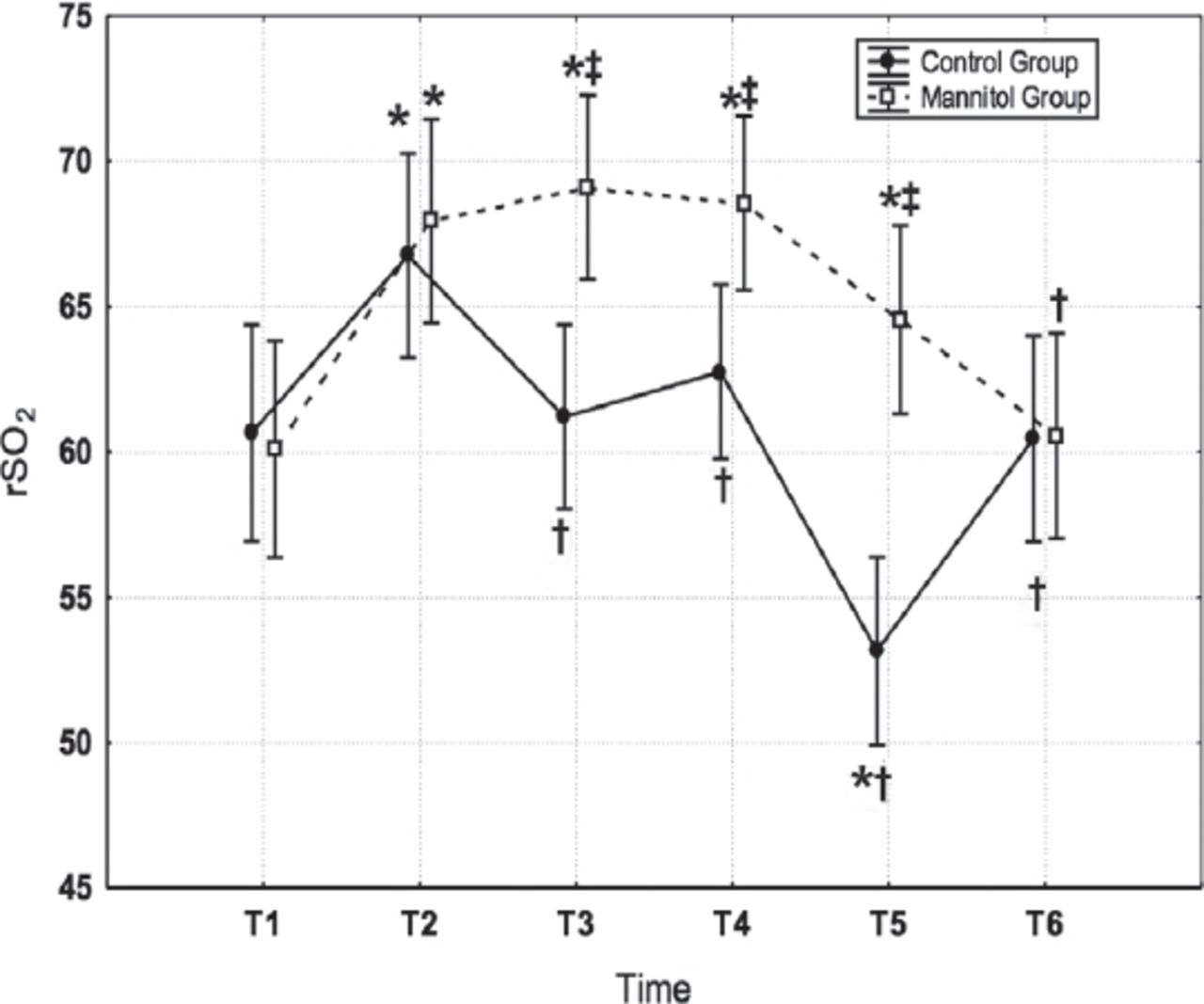
All patients completed the study. There were no differences between the 2 groups in demographic data. There were also no differences in the duration of abdominal insufflation, or the duration of surgery (Table 1). As shown in Figure 1, the induction of anesthesia in both groups with FiO2 50% increased rSO2 significantly above the pre-induction values. Abdominal gas insufflation reduced rSO2 in the control group but not in the mannitol group. This reduction reached its lowest value 30 minutes after extubation and was, even significantly less than the preinduction value. One hour after extubation, rSO2 returned to the control preoperative value and was similar in both groups. There were no significant differences between both groups in MAP or ETCO2 at any of the observation times. Time to extubation in group M (6.5 ± 1 min) was significantly shorter than the control group (9 ± 2 min), p<0.001. Similarly, The OAA/S of group M, 10 min after extubation was 4 (3-4) (median [IQ range]), and was significantly higher than that of group C (2 [2-4]) (p=0.007) indicating faster recovery. Later, patients in both groups had the same level of recovery with no difference between the 2 groups in the OAA/S at 20, and 30 minutes after extubation. No differences were detected between the 2 groups in the MMSE score for the cognitive function.
Intraoperative characteristics of patients included in a study on mannitol infusion during laparoscopic cholecystectomy.

Changes in cerebral oxygen saturation (rSO2) in the control and mannitol groups. Measurements were carried out before anesthesia induction (T1), after anesthetic induction (T2), 20 minutes after pneumoperitoneum (T3), after evacuation of pneumoperitoneum (T4), 30 minutes after extubation on room air (T5), and 60 minutes after extubation (T6). Vertical bars denote 95% confidence intervals. *Significant difference in comparison to T1. †Significant difference in comparison to T2. ‡Significant difference from the control group.
Discussion
This present study further proves the previous finding that abdominal gas insufflation during laparoscopic surgery decreases rSO2, and shows that this effect can be mitigated with preoperative infusion of small dose of mannitol. Gipson et al16 studied the alterations in rSO2 during laparoscopic surgery using in-vivo optical spectroscopy (INVOS [Somanetics Corporation, Troy, MI, USA) cerebral oximeter. The cohort for their study included 70 adults for laparoscopic herniorrhaphy, gastric bypass, or cholecystectomy. They concluded that significant changes in rSO2 do occur in some patients during insufflation for laparoscopic surgery. Other investigators described similar effect, and suggested intermittent pneumatic sequential compression of the lower extremities to restore rSO2.17,18 Increased intra-abdominal pressure during laparoscopy results in increased systemic vascular resistance and decreased cardiac output.19-21 These alterations in systemic hemodynamics may result in alterations in end-organ blood flow and oxygen delivery. In addition, abdominal insufflation raises ICP due to increased venous pressure, which hinders cerebral venous drainage from the lumbar venous plexus with a consequential increase in the cerebral blood volume.1
Mannitol infusion lowers ICP via creating an osmotic gradient between plasma and brain tissue, drawing water from the cerebral extracellular space into the vasculature.22 Zhou et al23 suggested the use of mannitol to increase the cerebral oxygen content after prolonged retroperitoneal laparoscopy. However, in their study, cerebral oxygen balance was evaluated through blood gas analysis of samples obtained from the jugular bulb and the radial artery, and mannitol was administered 150 minutes after abdominal insufflation. The small dose of mannitol (0.5 g/kg) used in the present study was selected to minimize the potential side effects that include initial volume expansion with increased risk of heart failure, subsequent hypovolaemia and hypotension, metabolic acidosis and electrolyte imbalance, including hypernatraemia and hypokalaemia. However, further studies are required to find out the optimum dose of mannitol.
Partial pressure of carbon dioxide (PaCO2) was identified as a major predictor of cerebral saturation24 since it was found to be the most potent physiologic cerebral vasodilator with the rate of cerebral blood flow increases linearly by 2-4% per mm Hg PaCO2 within the range of 25-75 mm Hg.25,26 There were no significant differences in our study between both groups in ETCO2 since we maintained ETCO2 within the normal range by mechanical ventilation. Similarly, body position can influence rSO2. A previous study8 on laparoscopic gynecological surgery demonstrated that rSO2 was decreased in association with the Trendelenburg position. Some studies demonstrated that rSO2 increased during Trendelenburg-pneumoperitoneum condition, and PaCO2 increased in a similar manner.27,28 It has been suggested that rSO2 measurements can best be assessed if the patient’s body position is held constant.29 All our rSO2 measurements were obtained while patients were in 30° anti-Trendelenburg position.
Our results showed that control patients with lower rSO2 had a significant longer extubation time, and a significant higher OAAS at 10 min indicating earlier recovery. Postoperative MMSE scores for the cognitive function was similar in both groups at one hour after extubation, and was not different from the preoperative levels. Casati et al29 demonstrated a faster recovery and hospital emergence when perioperative rSO2 were maintained at 75% of baseline in elderly patients undergoing major abdominal nonvascular surgery. Casati et al29 suggested that decreased rSO2 is unlikely to have a clinical significance in the form of neurocognitive changes unless it is less than 75% of baseline. None of our patients had rSO2 less than 75% of the baseline. The absence of cognitive changes in our patients may also be related to the younger age of our patients and the short duration of pneumoperitoneum. Papadopoulos et al30 in a prospective observational study that included 69 elderly patients with hip fractures recorded rSO2 values from baseline until the second postoperative hour and MMSE scores preoperatively, and on the seventh postoperative day. They used a protocol to promptly treat intra-operative cerebral desaturation; nevertheless, among their patients with normal baseline rSO2, 3 patients developed intraoperative desaturation and had postoperative cognitive dysfunction.
Our study has some limitations. First, we selected to test the effect of a small dose of mannitol to avoid mannitol side effects. However, a dose response study is required to find the optimum dose of mannitol and the timing of its administration, especially with prolonged procedures and those with Trendelenburg position. Second, our patients were healthy patients aged less than 50 years. Further studies are required to test the benefit of mannitol in older patients and those with mild cognitive changes. Recommendations to treat rSO2 include ensuring adequate ventilation, checking head positioning, increasing FiO2, allowing PaCO2 to increase if less than 35 mm Hg, and increasing BP with fluids or vasoconstrictors, and decreasing the cerebral metabolic rate of oxygen by propofol administration. Our study proves that preoperative mannitol infusion maintains rSO2 during laparoscopic surgery. Further studies are needed to reveal whether mannitol could improve rSO2 in other clinical settings and surgical procedures, such as cardiac surgery.
In conclusion, in this study we concur the following: abdominal gas insufflation for laparoscopic surgery decreases rSO2; reduction of rSO2 was associated with longer recovery; and rapid infusion of small dose of mannitol prevents the effect of insufflation on rSO2 and enhances recovery.
Related Articles
Al-Qahtani HH, Alam MK, Asalamah S, Akeely M, Ibrar M. Day-case laparoscopic cholecystectomy. Saudi Med J 2015; 36: 46-51.
Beqiri AI, Domi RQ, Sula HH, Zaimi EQ, Petrela EY. The combination of infiltrative bupivacaine with low-pressure laparoscopy reduces postcholecystectomy pain. A prospective randomized controlled study. Saudi Med J 2012; 33: 134-138.
Muter SA, Rifat UN, Abd ZH. Renoprotective effect of mannitol infusion during extracorporeal shock lithotripsy. Saudi Med J 2009; 30: 767-770.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 26, 2015.
- Accepted June 19, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.