


Abstract
Otologic manifestations in chronic lymphocytic leukemia (CLL) are common presentations. However, temporal bone metastasis is rarely described as a sign of relapsing CLL. A 65-year-old male diabetic patient known to have CLL on remission presented to the outpatient otolaryngology clinic with a one month history of progressive bilateral otalgia and right otorrhea, despite multiple courses of antibiotics. He was admitted with suspicion of malignant otitis externa. Left ear showed large hemorrhagic bullae on the posterior segment of tympanic membrane. Left sided facial paralysis developed on the third day of admission. Full recovery of facial paralysis is achieved by 10 days course of corticotherapy. Histological examination of middle ear tissue biopsy showed infiltration by monotonous small lymphoid cells, showing round nuclei, condensed chromatin suggestive of CLL. Although rare, unusual otologic manifestations should raise the suspicion of a temporal bone metastasis as a sign of relapsing CLL.
The incidence of otologic complains in leukemia patients ranges from 16.8-48%.1 Hearing loss, conductive, or sensorineural, is the most common symptom. In addition, patients may complain of tinnitus, vertigo, otalgia, otorrhea, and otorrhagia.2 Although, otologic manifestations are very common in those patients, leukemic infiltration of the temporal bone is very rare, and only few cases are reported in the literature. We report a case of relapsing chronic lymphocytic leukemia (CLL) presenting with otitis media and lower motor neuron facial paralysis. Our objective in presenting this particular case is to highlight the rare temporal bone complications and management in CLL.
Case Report
A 65-year-old diabetic patient was admitted to the hospital with suspicion of skull base osteomyelitis. He presented with bilateral persistent otitis media for one month not responding to antibiotic therapy with severe otalgia. Past medical history revealed CLL 15 years ago. He was in complete remission for 8 years before having a recurrence presented as nasopharyngeal mass with secretory otitis media. A second relapse was detected last year where histology of a nasopharyngeal mass showed evidence of Richter’s transformation to high-grade lymphoma. He was started on cyclophosphamide, Hydroxydaunorubicin, oncovin, and prednisone (CHOP) chemotherapy regimen for 4 months and then continued on Rituximab to complete a 6-month cycle. On admission, the right ear showed purulent otorrhea with edematous external auditory canal. Left ear showed large hemorrhagic bullae on the posterior segment of tympanic membrane that gives the impression of bullous myringitis.
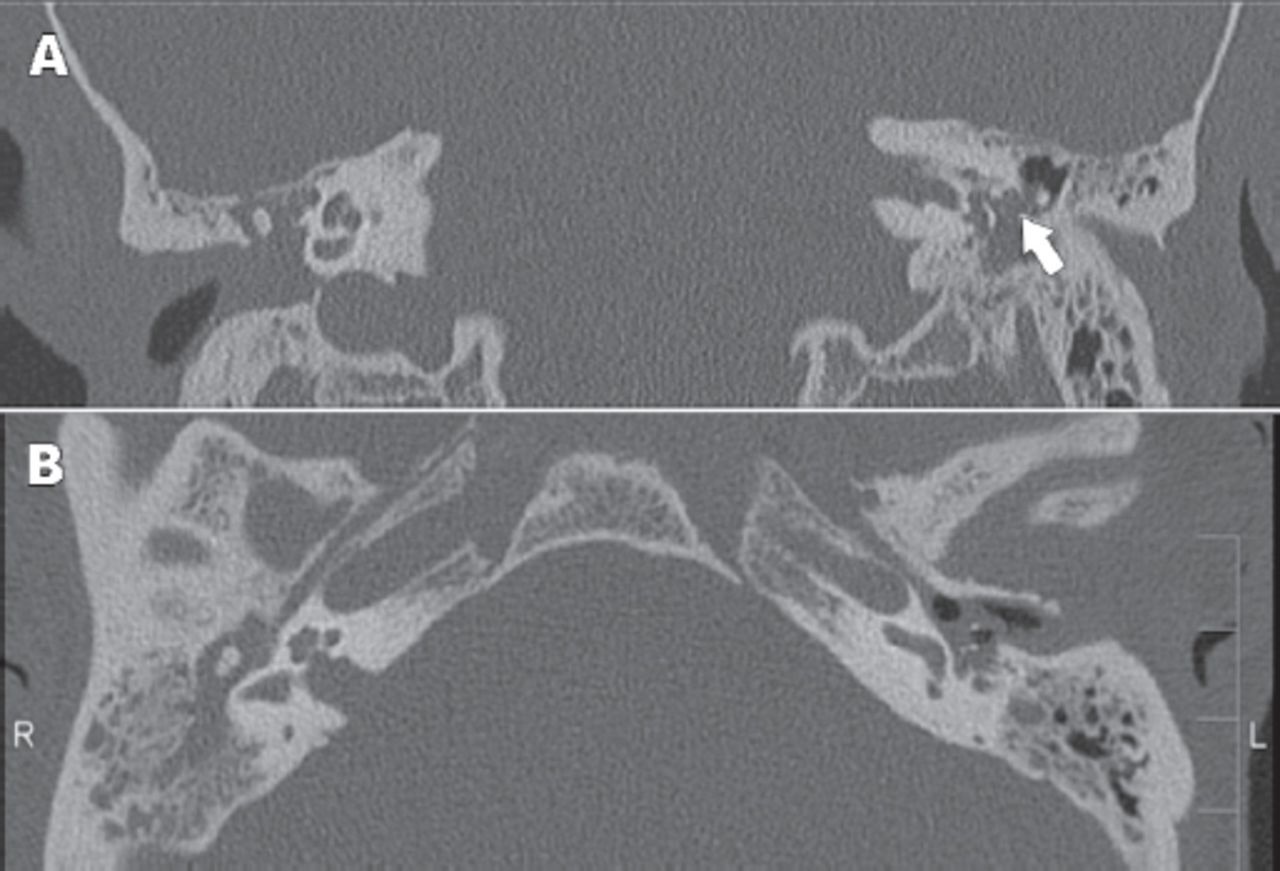
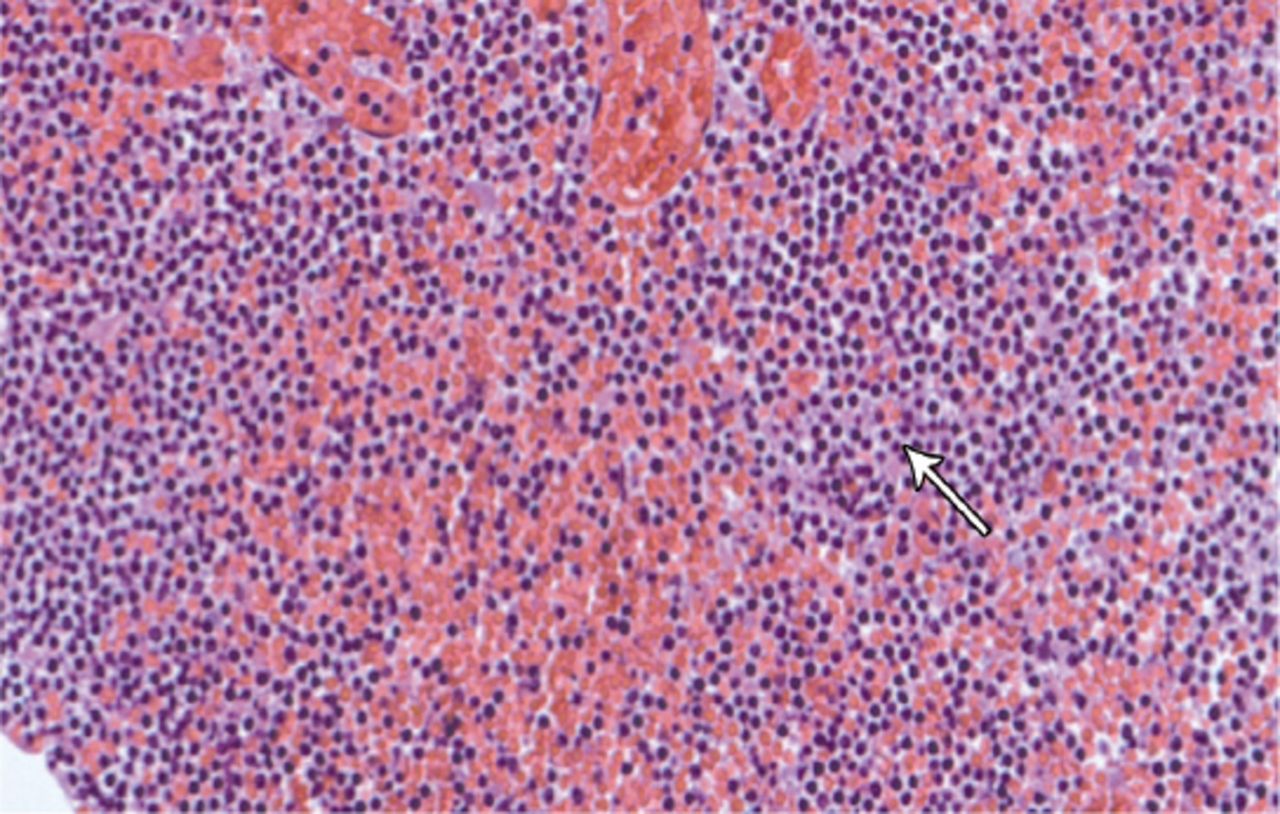
Nasopharyngoscopy revealed a non-obstructive central nasopharyngeal mass while the rest of the otorhinolaryngology examination was clear. Audiogram showed bilateral, moderate to severe mixed hearing loss. Temporal bone CT scan revealed bilateral opacification of the middle ears and mastoids cavities with dehiscence of the tympanic portion of the facial nerve bilaterally (Figure 1). No other bony erosions were noted. A complete blood count revealed hemoglobin - 10.8 g/dL (normal value [NV] - 13-17 g/dL), platelet - 494,000 mcL (NV - 150,000-450,000 mcL), and white blood cells - 108,000 mcL (NV - 4,500-10,000 mcL) with 85% lymphocytes. He was started on intravenous antibiotics, and on the third day of admission, he developed left sided lower motor neuron facial paralysis. He was sent to the surgical theater for myringotomy and ventilation tube insertions. His left tympanic membrane (TM) was perforated, and granulation tissue can be seen filling the mesotympanum and protruding through it. Biopsy of this granulation tissue was consistent with a lymphoproliferative malignancy (Figure 2). Bone marrow aspirate confirmed the diagnosis of a relapsing CLL. Cytogenetic chromosomal analysis revealed 71% trisomy 12 (which is the most common cytogenetic change in CLL, associated with an intermediate prognosis), and 13% monosomy p53. He was started on Ibrutinib, a long term daily oral chemotherapy that resulted in complete remission. Facial nerve paralysis was completely recovered with a residual TM perforation on the left ear. Granulation tissue of the middle ear disappeared completely at one month follow up after treatment.
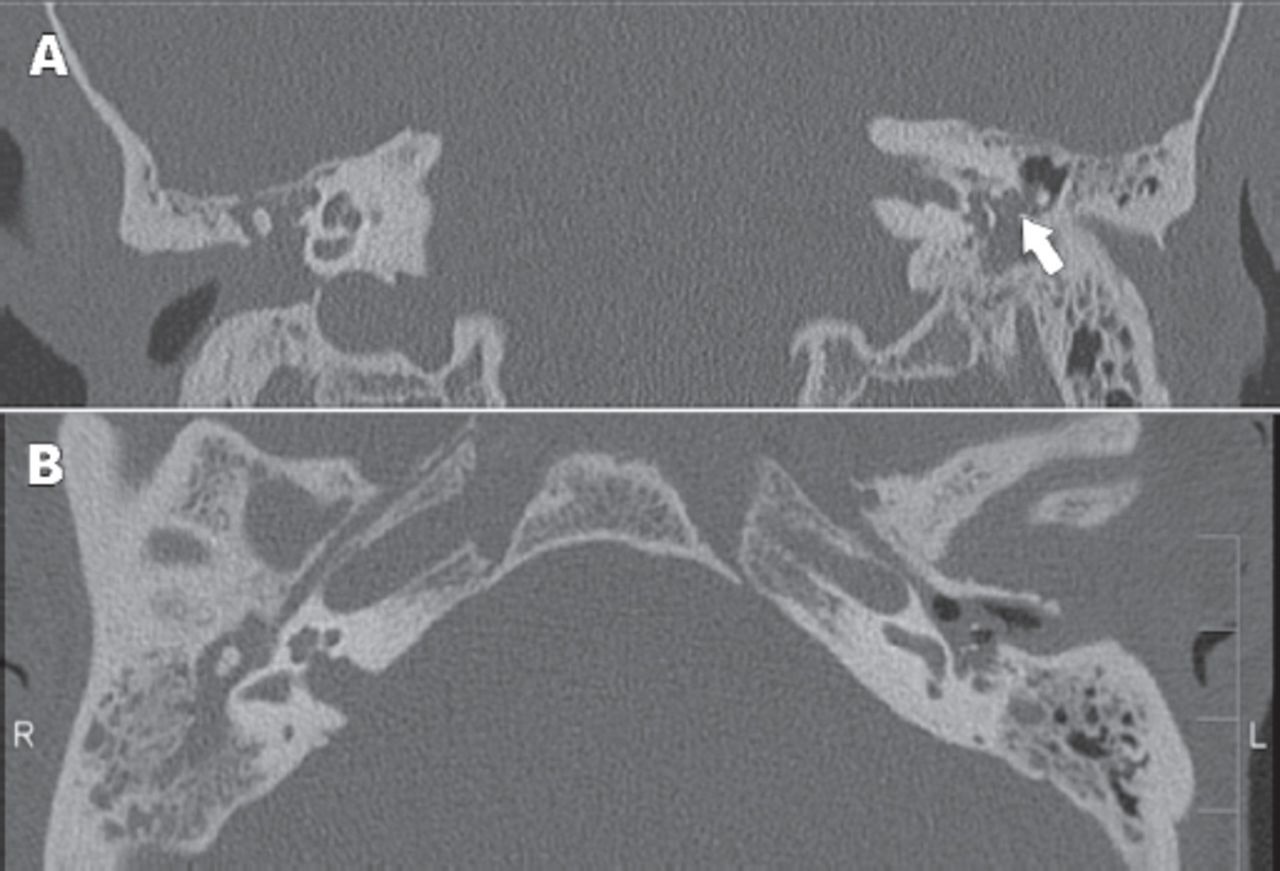
Coronal (A) and Axial (B) CT scan cuts of the temporal bones showing homogenous opacity of the mastoid and middle ear cavity. Dehiscent fallopian canal of the facial nerve is visible on the left side (arrow).
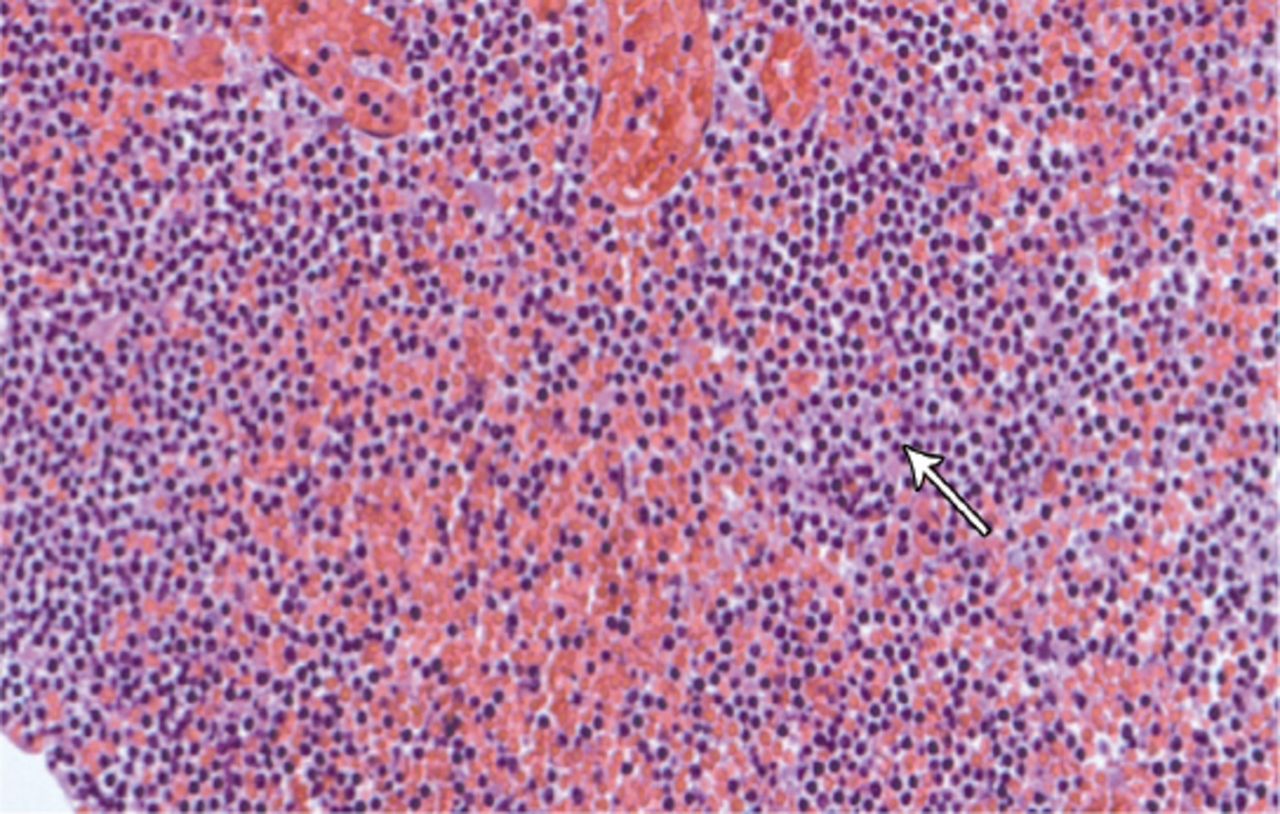
Fragment of middle ear granulation tissue infiltrated by monotonous small lymphoid cells showing round nuclei, condensed chromatin, inconspicuous nucleoli, and scanty cytoplasm (arrow).
Discussion
An elderly diabetic patient presenting with otalgia and facial nerve paralysis has most probably skull base osteomyelitis. However, this present study shows that those findings can be signs of relapsing CLL. Chronic lymphocytic leukemia is characterized by proliferation of (mono) clonal mature B-lymphocytes in peripheral blood, bone marrow, and lymphoid tissues with a characteristic immunophenotype.3 In a study of the frequency of genetic abnormalities in leukemic B-cells, 111 out of 180 CLL cases (62%) displayed one or more cytogenetic abnormalities. In the whole series, del(13q-) was the most frequently observed abnormality (35%) followed by trisomy 12 (23%), 11q- (9.4%), and 17p- (8%).4 Peripheral facial palsy (PFP) is most commonly caused by a benign self-limiting inflammatory neuropathy condition, known as Bell’s palsy.5 However, systemic diseases can present with PFP including Guillain-Barré syndrome, sarcoidosis, syphilis, leukemia, Lyme disease, meningitis, and acute HIV infection.6
Temporal bone metastasis from distant primary carcinoma can mimic any local inflammatory or infectious process. Metastasis can reach the temporal bone through any of these patterns: a) hematogenous spread; b) tumor cells gaining access to the cerebrospinal fluid and disseminating through the subarachnoid space into the internal auditory canal; c) direct extension; d) leptomeningeal extension from an intracranial primary tumor; and e) lymphomatous infiltration.7 Druss8 in 1945, was the first otologist to call attention to the fact that patients with leukemia can present with secondary otological complications.
Buyukavci et al9 reported that bilateral PFP is a warning sign of leukocyte infiltration. The CLL can present with otologic symptoms in up to half of the affected persons, such as acute otitis media and acute mastoiditis.10 However, it is important to keep in mind the possibility of temporal bone metastasis of CLL with unusual presentations, including facial paralysis and sensorineural hearing loss.
In conclusion, unusual otologic manifestations in patients with past history of CLL should alert us to the possibility of temporal bone metastasis. Full history and physical examination is mandatory in addition to proper imaging and histological exams.
Related Articles
Basakran NS. CD44 as a potential diagnostic tumor marker. Saudi Med J 2015; 36: 273-279.
Raja-Sabudin RZ, Othman A, Ahmed-Mohamed KA, Ithnin A, Alauddin H, Alias H, et al. Immature reticulocyte fraction is an early predictor of bone marrow recovery post chemotherapy in patients with acute leukemia. Saudi Med J 2014; 35: 346-349.
Hou S, Yang W. A meta-analysis on Rituximab combined CHOP chemotherapy for non-Hodgkin lymphoma in China. Saudi Med J 2011; 32: 675-678.
Acknowledgment
We thank our colleagues Dr. Heba N. Raslan, MD, Consultant Hematopathology, and Dr Ahmed Alsaghier, MD, Consultant Hemato-Oncology, King Fahd Specialist Hospital, Dammam, Kingdom of Saudi Arabia for their insight and expertise that greatly assisted this case report.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 10, 2015.
- Accepted August 19, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.