


Abstract
Fibrovascular polyps of the esophagus are rare, benign, and submucosal tumor-like lesions, their course is usually indolent until reaching enormous proportions. The most frequent symptoms are dysphagia, vomiting, and weight loss. Surgical excision is the treatment of choice, since endoscopic removal is not always feasible. We report a case of a 59-year-old man with a giant fibrovascular polyp who complained of progressive dysphagia. The lesion was resected by left cervical approach. The patient remains symptom-and recurrence-free within one-year of follow-up.
Fibrovascular polyps (FP) of the esophagus are rare, benign, intraluminal, submucosal tumor-like lesions that usually remain asymptomatic. The cause of the disease is unknown. Symptoms are present when the polyp reaches a large size, and include progressive dysphagia, odynophagia, and respiratory symptoms. We report a case of an old man with a giant esophageal fibrovascular polyp identified with computed tomographic (CT), endoscopy and specimen images. Our objective in presenting this particular case is to introduce the diagnosis and treatment of the giant esophageal fibrovascular polyp.
Case Report
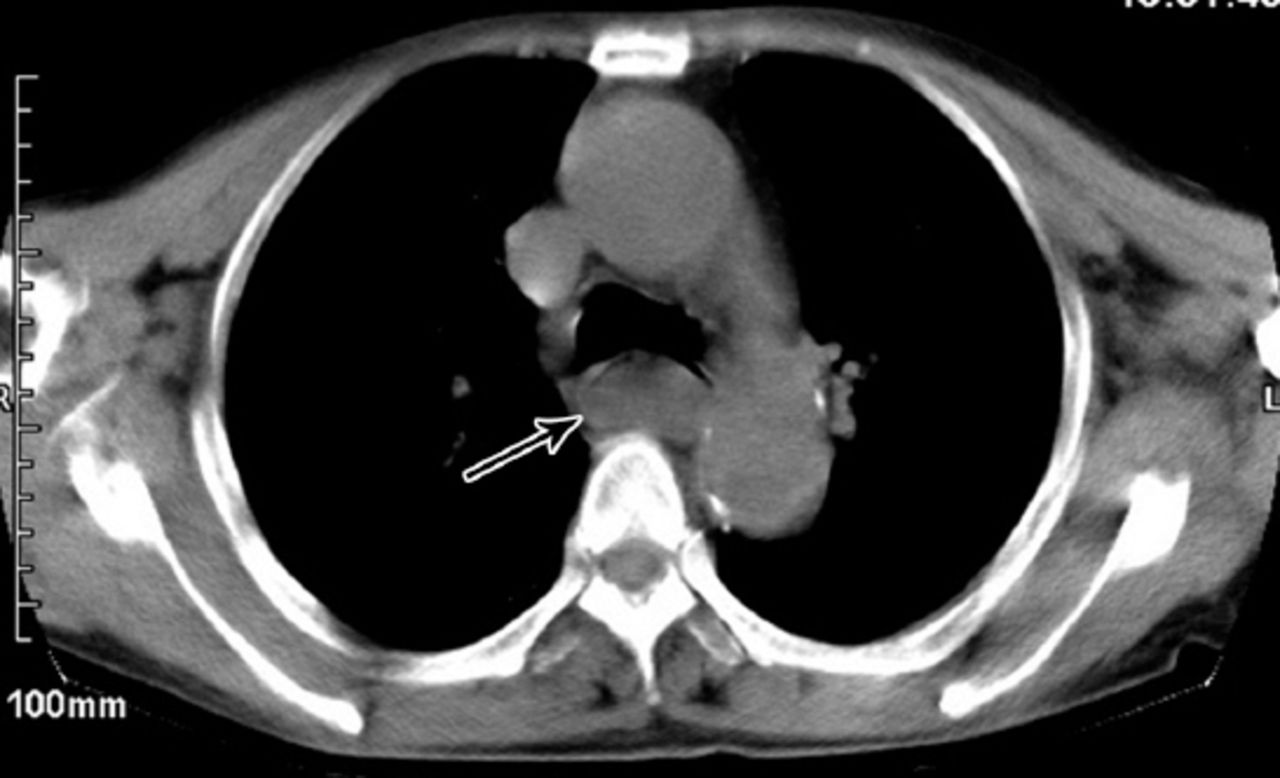
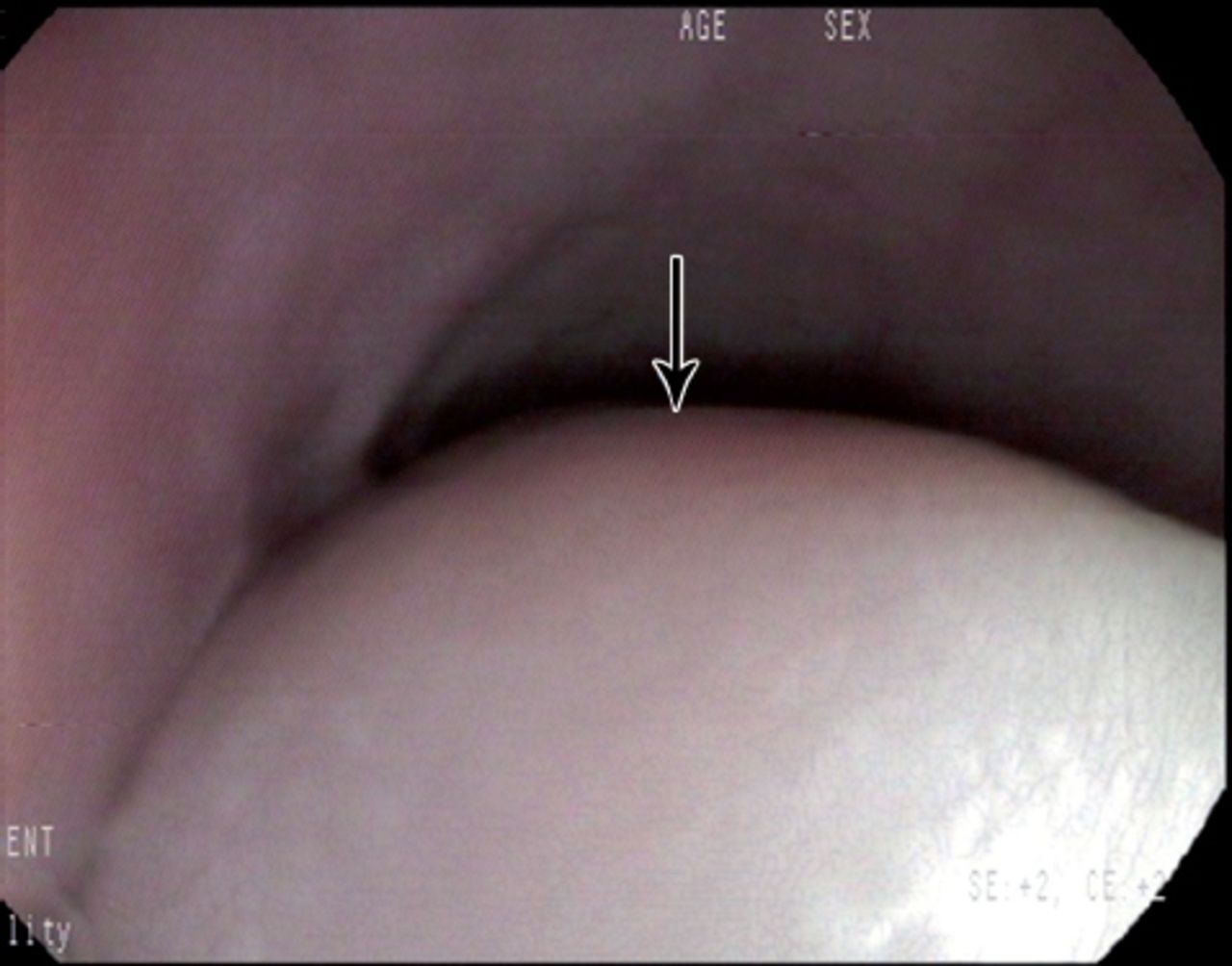
We report a case of a 59-year-old man who complained of progressive dysphagia for solids and liquids. He regurgitated a fleshy mass out into his mouth and swallowed occasionally, without attack of dyspnea. No history of loss weight, cough, or hematemesis was noted. The CT scan of the neck and thorax demonstrated a large (14×3×2 cm) intraluminal esophageal mass extending from the level of the cervical esophagus to the lower esophagus with no clear relation to the esophagus wall (Figure 1). The esophagogastroduodenoscopy showed a sausage-shaped mass obstructing the esophageal lumen, arising from the upper esophageal sphincter, and ending 15cm below (Figure 2). Due to the huge size of the polyp, the origin of the pedicle was not found. The decision was made to proceed with a left cervical esophagotomy. An esophagotomy was made, 4 cm in length, along the anterior border of the sternocleidomastoid muscle. After initial delivery of the distal tumor through the esophagotomy, the mucosal origin of the stalk was completely visualized, ligatured, and resected (Figure 3). The esophagotomy was sutured in a 2-layered fashion. Pathological examination showed fibrovascular polyp of the esophagus (Figure 4). He started oral feeding on the seventh postoperative day, and was discharged on the fourteenth day with good acceptance of diet. He has been followed up for one year without any sign of recurrence.
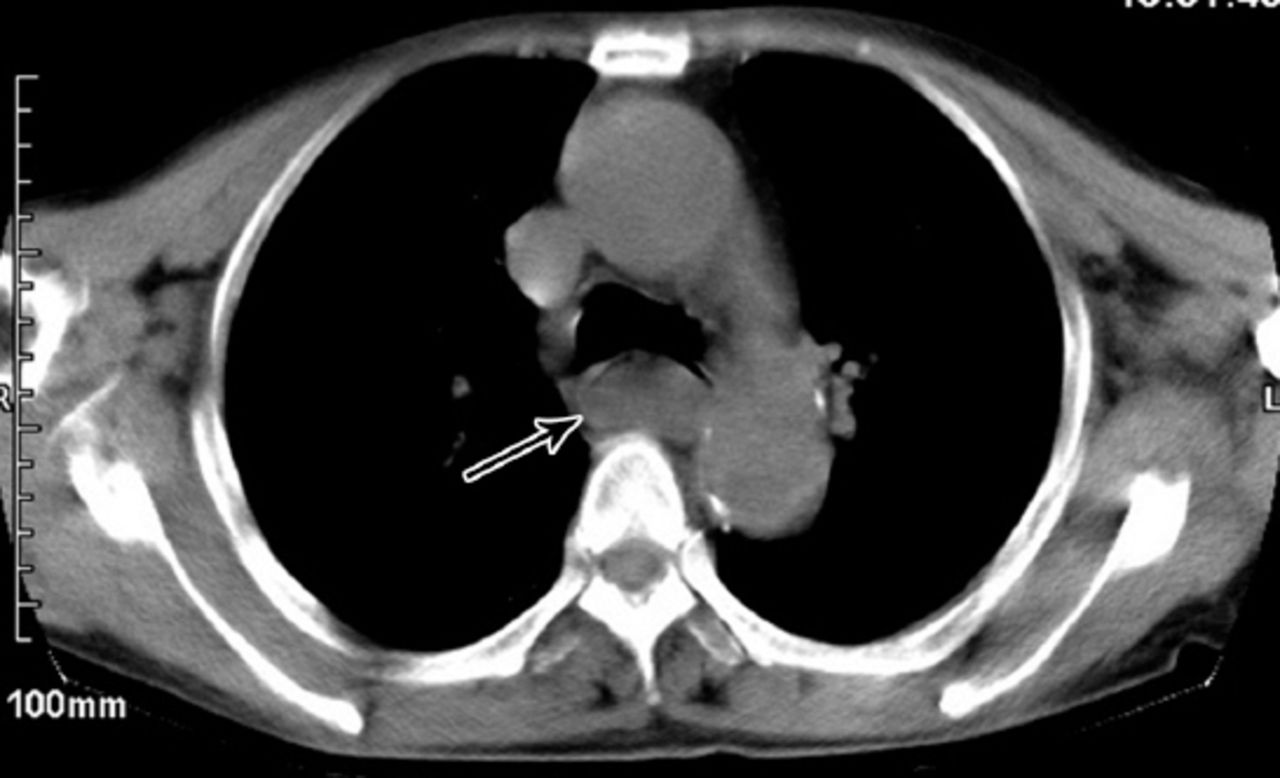
Computed tomographic scan of the chest demonstrates a large, fat density, intraluminal lesion in the esophagus (arrow).

The esophagogastroduodenoscopy showed a sausage-shaped mass obstructing the esophageal lumen (arrow).

A complete sausage-shaped mass with a stalk after surgery.
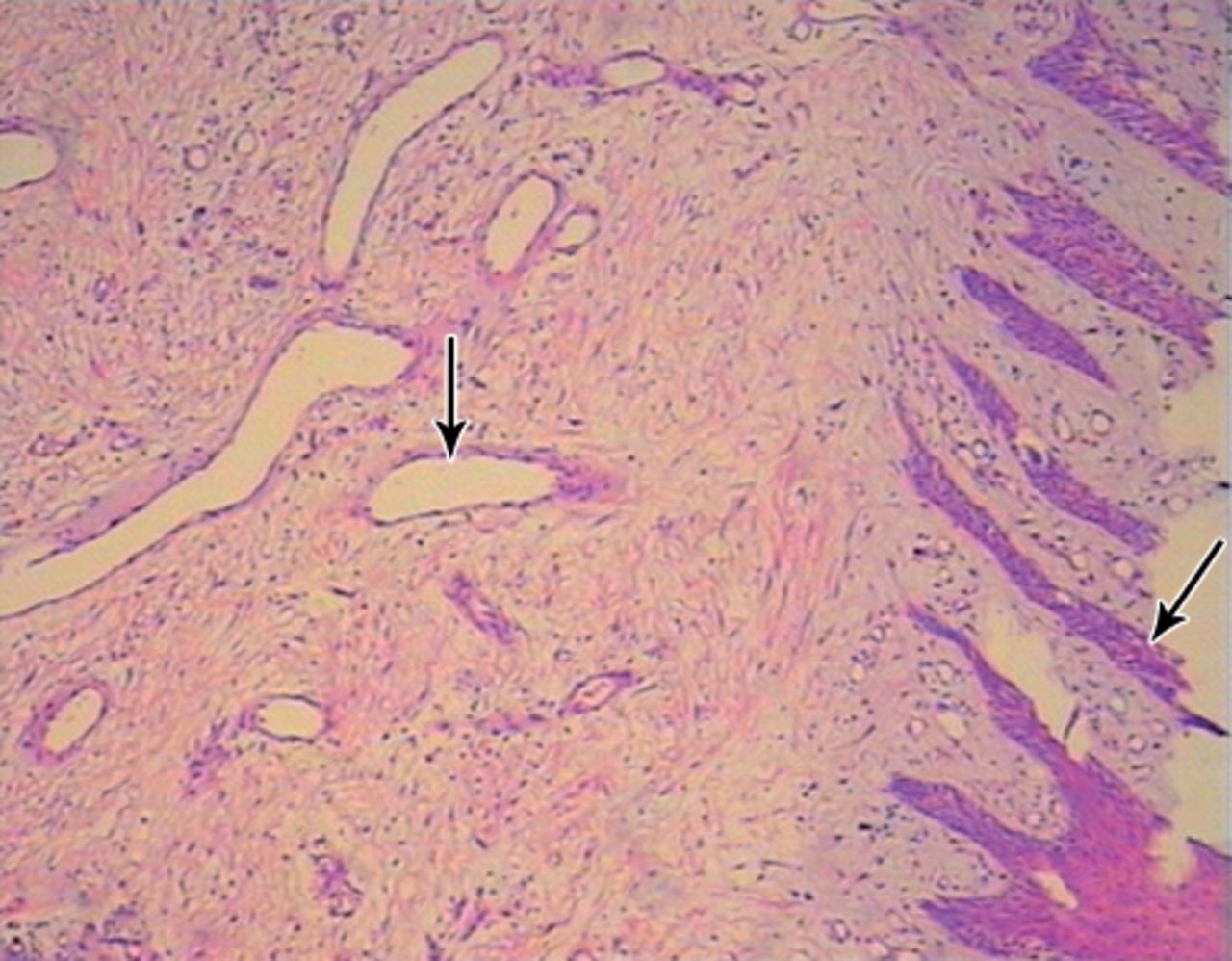
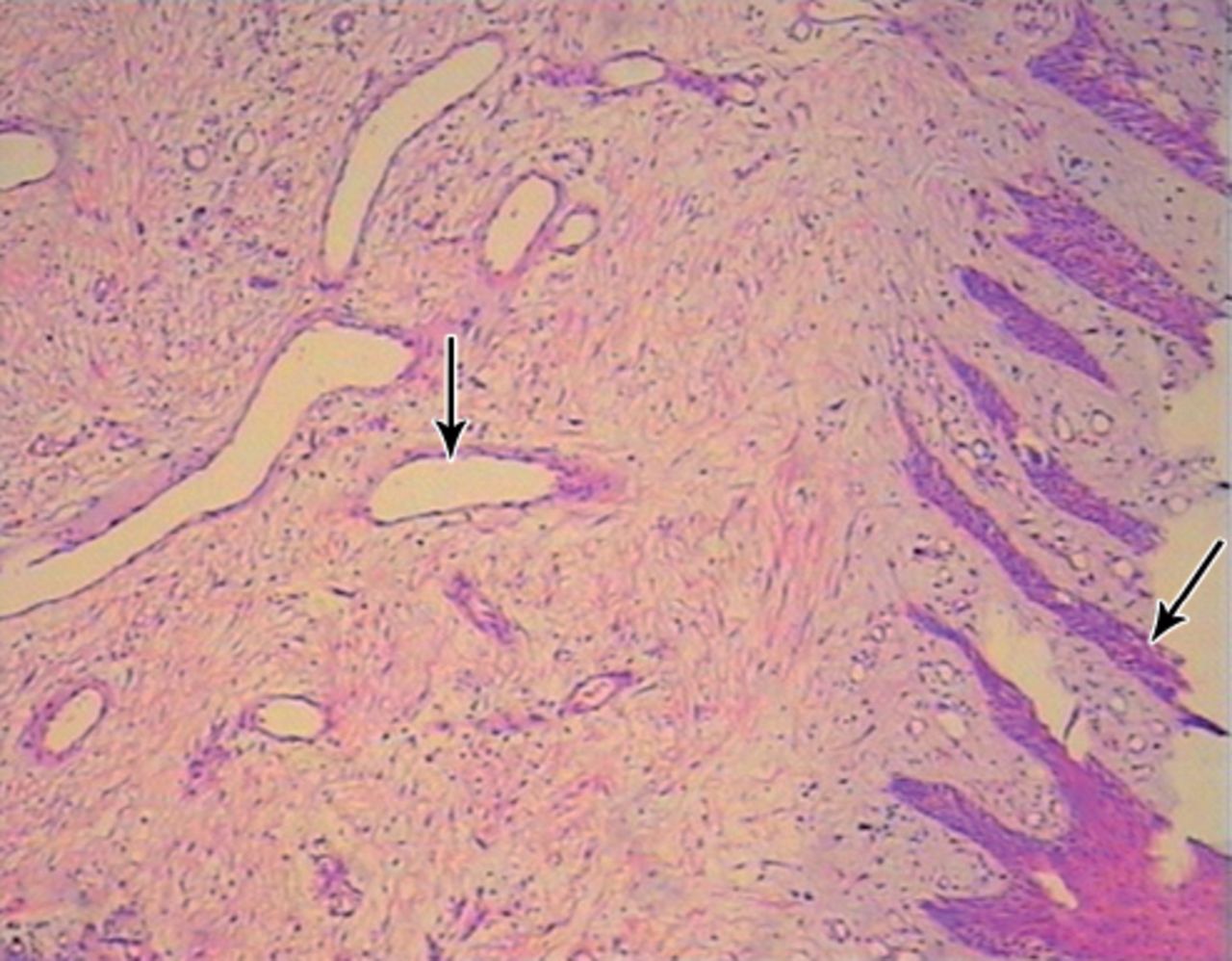
Polypoid lesion covered by squamous epithelium (arrow), blood vessels (arrow), and lymphoplasmacytic infiltrate (Hematoxylin & Eosin ×40).
Discussion
Fibrovascular polyps of the esophagus are rare benign tumor-like lesions, accounting for approximately 1% of all esophageal benign tumors.1 There are more than 100 cases reported in the literature so far. Fibrovascular polyps greater than 5cm in maximal diameter are defined as a giant FP. Usually these polyps arise from the cervical esophagus, inferiorly to the cricopharyngeal muscle, and this area has also been termed as the Laimer-Haeckermann triangle (also known as the Laimer’s triangle),2 which reveals their trend to prolapse into the mouth causing the characteristic “regurgitation of a fleshy mass”. Because the disease has no symptoms at the early stage, the lesions often can grow very large when it was found. Dysphagia, vomiting, chronic gastrointestinal bleeding, hoarseness, throat discomfort, weight loss, and respiratory symptoms are the most frequent complaints of patients with FP.3 They may also present as regurgitated masses into the mouth, and can cause laryngeal occlusion and subsequent asphyxiation if the polyp is large enough in size.4,5
For purposes of diagnostic investigation, barium double-contrast examination of the esophagus is commonly used, which shows a sausage-shaped mass with multiple filling defects. Endoscopy visualizes an intraluminal mobile mass covered with normal mucosa, emerging from the upper esophagus. Endoscopic ultrasonography may be useful, since it provides information on a diameter of a polyp, as well as its vascularity at insertion point. At CT, fibrovascular polyps can manifest different degrees of attenuation values according to the proportions of fibrous and adipose tissues. The mainstay of treatment once diagnosis is achieved is resection, which is necessary in view of the potential risk of respiratory compromise, bleeding, and the debilitating symptoms. It is worth noting that atypical lipomatous tumor (ALT) and FP symptoms are very similar, but ALT is a rare, low-grade malignant neoplasm.6 Malignancy cannot be excluded preoperatively and excision is the approach to get definitive diagnosis.
There are 2 options: surgery or endoscopic resection, based on the size, the location of the stalk’s base, its mobility, and the vessels that nourish it. The FP less than 2 cm can be removed by endoscopic resection. But those larger than 5 cm usually require open surgical resection, because of the thick vascularized pedicle.7 In most cases, the left-sided cervical is the preferred approach. If the lesion is huge, a thoracotomy or a laparotomy may be necessary. A recurrent giant FP patient underwent several surgeries via a combination of endoscopic, trans-oral, trans-cervical, trans-thoracic and trans-abdominal approaches.8 If the diagnosis is not clear or the lesion cannot be completely removed through the simple esophagostomy, esophageal resection may be necessary. The recurrence of FP after resection within years is very rare, so patients should undergo CT and endoscopic surveillance for several years.8
In conclusion, giant fibrovascular polyps are uncommon benign neoplasms of the esophagus and its recurrences are more uncommon. Resection is recommended in view of potential deadly complications. Endoscopic resections, open surgery via trans-cervical, trans-thoracic, or trans-abdominal approaches have been used. Investigations should aim to identify the pedicle’s origin and the bulk of the polyp before operation, to aid in the planning of the surgical approach.
Case Reports
Case reports will only be considered for unusual topics that add something new to the literature. All Case Reports should include at least one figure. Written informed consent for publication must accompany any photograph in which the subject can be identified. Figures should be submitted with a 300 dpi resolution when submitting electronically or printed on high-contrast glossy paper when submitting print copies. The abstract should be unstructured, and the introductory section should always include the objective and reason why the author is presenting this particular case. References should be up to date, preferably not exceeding 15.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received June 1, 2015.
- Accepted September 25, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.