


Abstract
Odontomas are odontogenic tumors formed of various dental tissues.They are classified into: central odontomas that are common, eruption odontomas that are rare with only 23 cases reported to date, and peripheral odontomas that are also rare. We present a case of a large complex eruption odontome in a 24-year-old Saudi male.
Historically, the term odontoma was first coined by Paul Broca in 1867 who defined it as tumors formed by the overgrowth of transitory of complete dental tissues.1 Odontomas are slow-growing, benign, odontogenic tumors that are usually asymptomatic and often discovered during routine radiography.
Histopathologically, odontomas can be divided into 3 groups:2 1) Complex odontoma: where the calcified dental tissues are arranged in an irregular mass bearing no morphologic similarity to rudimentary teeth. 2) Compound odontoma: epidemiologically, is the most common type of odontomas.3 It is composed of all odontogenic tissues in an orderly pattern that results in many teeth-like structures but without morphologic resemblance to normal teeth. Another rare variant of the compound odontomas is the so-called the peripheral compound odontomas, which arises extraosseously, and has a tendency to exfoliate.2 Histologically, they are composed of different dental tissues, including enamel, dentine, cement, and in some cases, pulp tissue.2,3 3) Ameloblastic fibro-odontoma: Is considered an immature precursor of a complex odontome. It consists of varying amounts of calcified dental tissue and dental papilla-like tissue.2
Clinically, 3 types of odontomas are recognized in the literature: central (intra osseous) odontoma, peripheral (extra osseous or soft tissue) odontoma, and erupted odontoma. Intraosseous (central) odontomas are located as it name implies inside the bone, and are discovered mainly incidentally, or due to aplasia, or impaction of a permanent or deciduous tooth. Intraosseous (central) odontomas are the odontogenic tumors of greatest incidence.2 Peripheral odontomas are the most rare clinical variant with only 6 cases reported to date2 with all of them microscopically diagnosed as compound odontomas. Lastly, and rarely intra osseous odontomas located coronally to an erupting or impacted tooth or superficially in the bone may facilitate their eruption into the oral cavity. These lesions have been traditionally referred to as erupted odontomas, with only 23 cases being reported to date. In spite of the close similarity between the latest 2 clinical variants of odontomas; the eruptive odontomas still differ from the peripheral type by being more complex odontomas histologically, affecting an older age group at the time of diagnosis, and frequently associated with non-erupted second molars.2 Our objective in presenting this particular case is to report an additional rare case of a very large symptomatic eruption odontome in a Saudi male patient.
Case Report
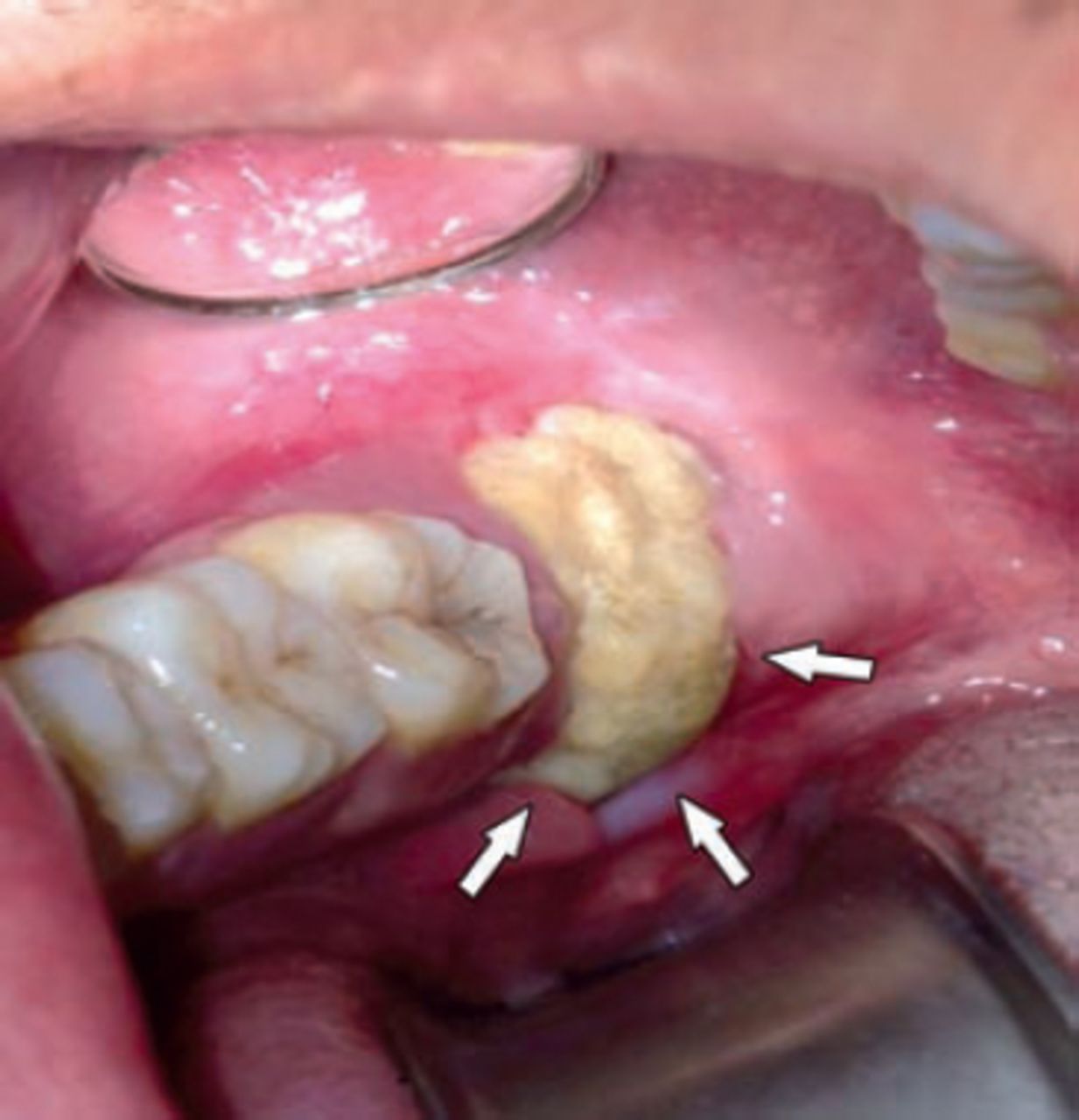
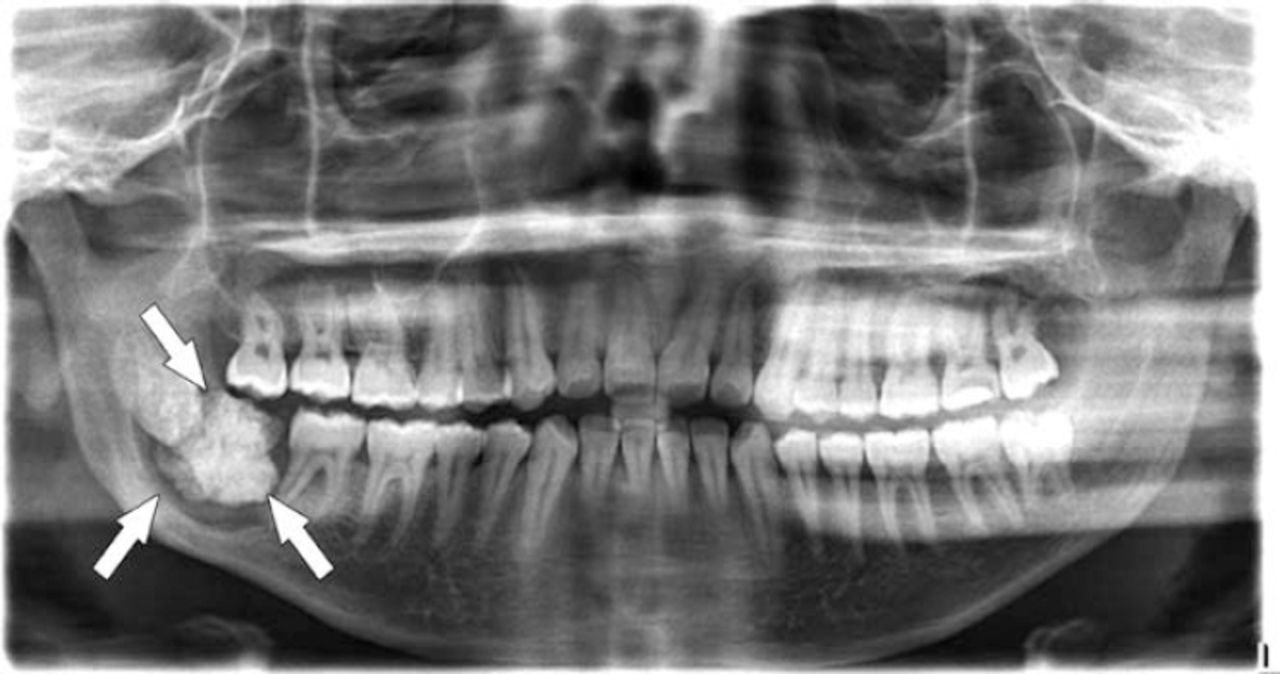
A 24-year-old Saudi male was referred to the oral and maxillofacial surgery clinic for consultation and treatment of repeated infection and pain in the right side of the lower jaw of over one-year duration. He also complained of bad odor and difficulty to open his mouth during the same period. On examination intra-orally, a hard bone-like structure with a rough surface exposed to the oral cavity distal to the right lower second molar was seen. Plaque accumulation over the mass with very foul odor and bad oral hygiene was noticed. The hard mass fenestrated the lingual tissues together with the gingival surrounding the lesion appearing very inflamed (Figures 1 & 2). Ortho-pantomo-graphic x-ray view showed a calcified mass distal to the lower right second molar, with the third molar on that side being displaced distally by the present mass. The calcified mass was encircled inferiorly on its central part by a radiolucent halo with the inferior dental canal being more inferiorly placed to the lesion. The lower right second molar showed advanced periodontal involvement with bone loss but without any resorption of its distal root (Figure 3).

Intra-oral view showing exposed calcified mass distal to the lower right second molar.

Intra-oral clinical view showing the lingual exposure of the mass and lingual tissues inflammation.
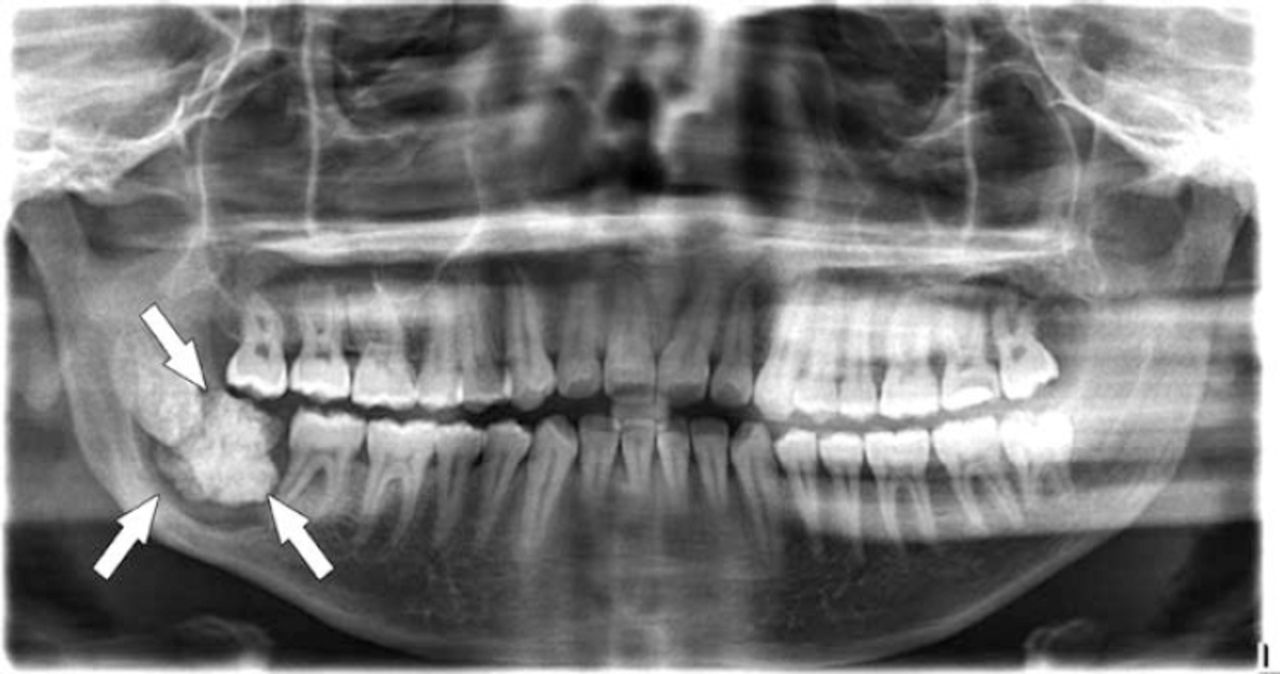
Ortho-pantomo-graphic x-ray view showing calcified mass on the lower right side related to horizontally impacted third molar tooth (#48) with a radiolucent halo encircling the central part of the calcified lesion.
He consented for the potential complications of surgically removing the mass in terms of inferior alveolar and lingual nerves injury, and possible pathologic fracture of the right side of the lower jaw while removing the lesion. The proposed treatment plan also included disimpaction of lower right third molar and extraction of periodontally involved second molar. He accepted the proposed treatment under local anesthesia but refused the extraction of the lower right second molar. Under local anesthesia, the surgical removal of the lower right third molar in addition to the calcified mass together with curettage of the infected soft tissues in the area was carried over. The specimens sent for histopathological examination included the soft tissues around the lesion and the hard, calcified lesion. The healing course postoperatively was uneventful without any neural defect of the related nerves.
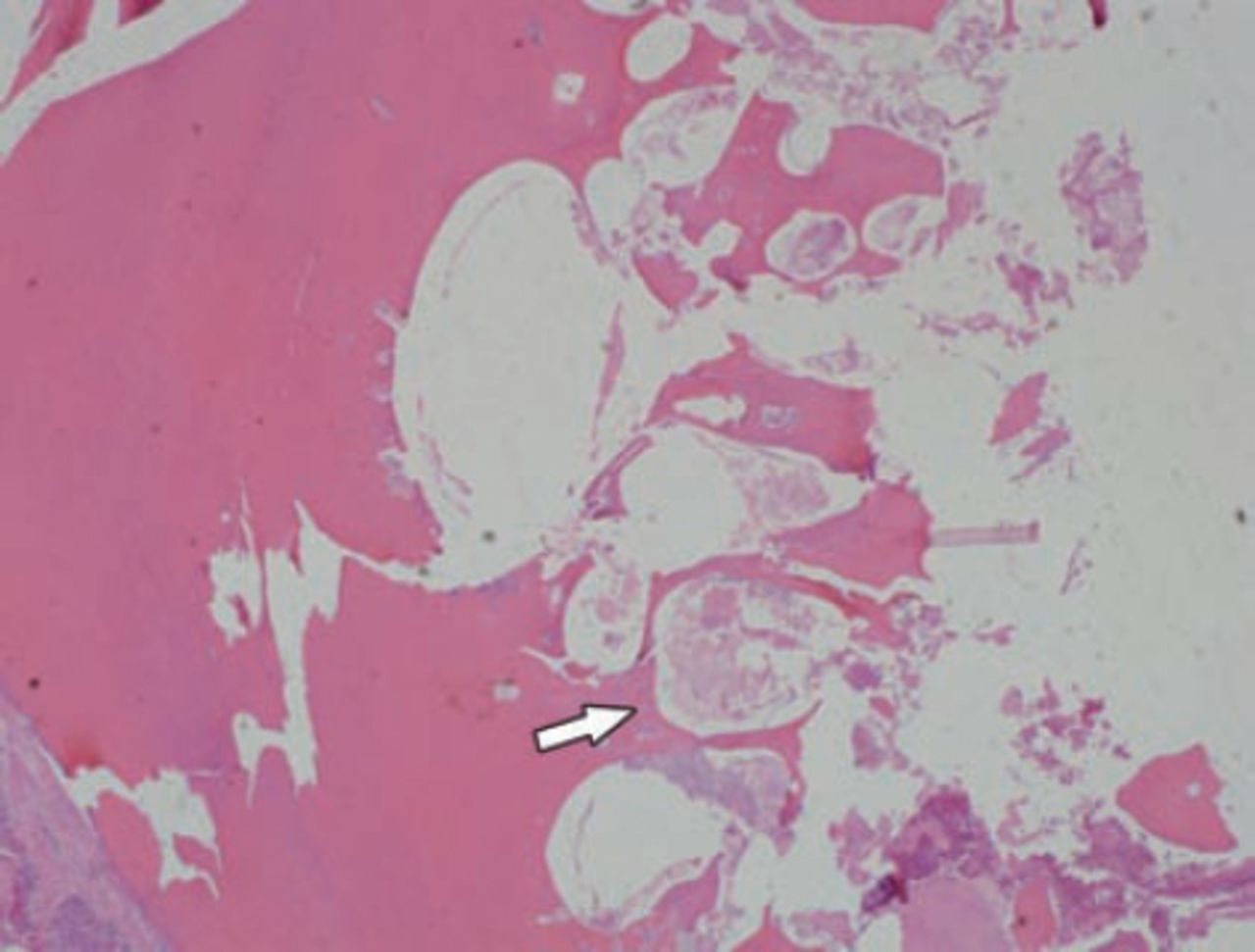
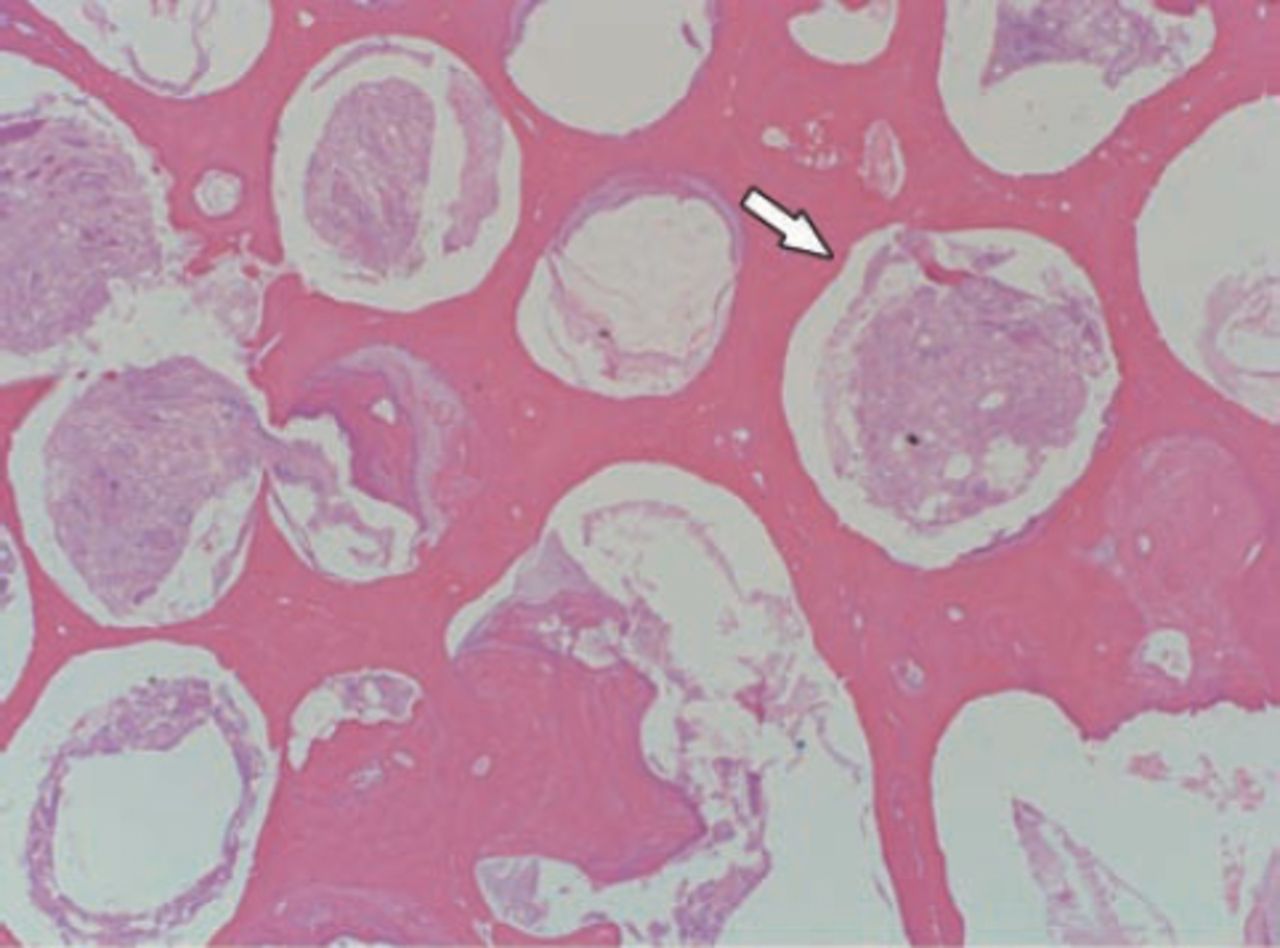
Histopathological report showed that the soft tissue specimen stained with hematoxylin and eosin stain (H&E stain) composed of inflammatory cells, necrotic debris, epithelial proliferation, and mucosal epithelial fragments. While the calcified specimen also stained with H&E stain showed irregular areas of decalcified dentine and enamel with a final diagnosis of complex odontome associated with infected tissues (Figures 4 - 7).
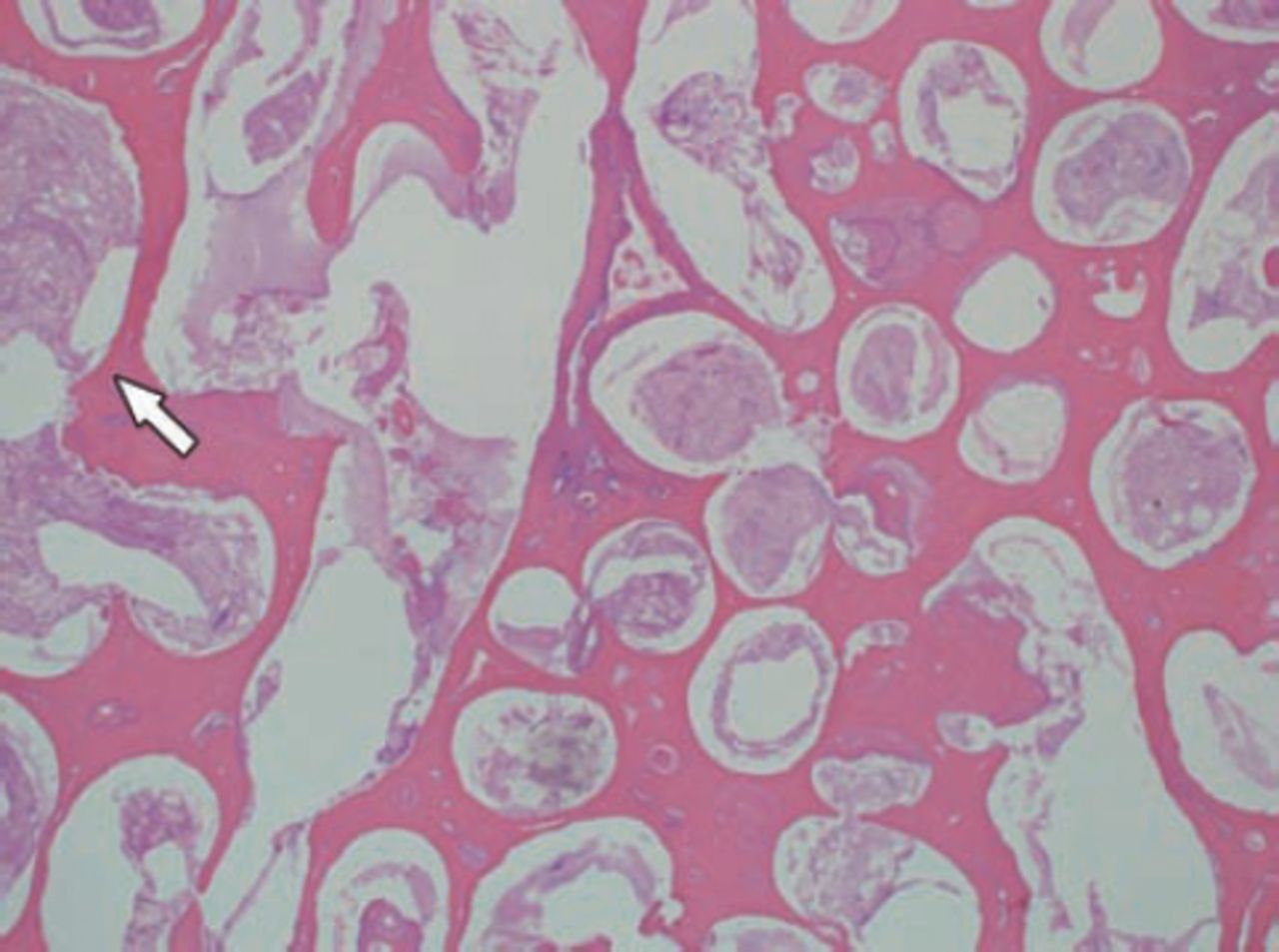
Histopathological decalcified section stained with hematoxylin and eosin stain of the complex odontome with area of irregularly arranged decalcified enamel and dentin (arrow).
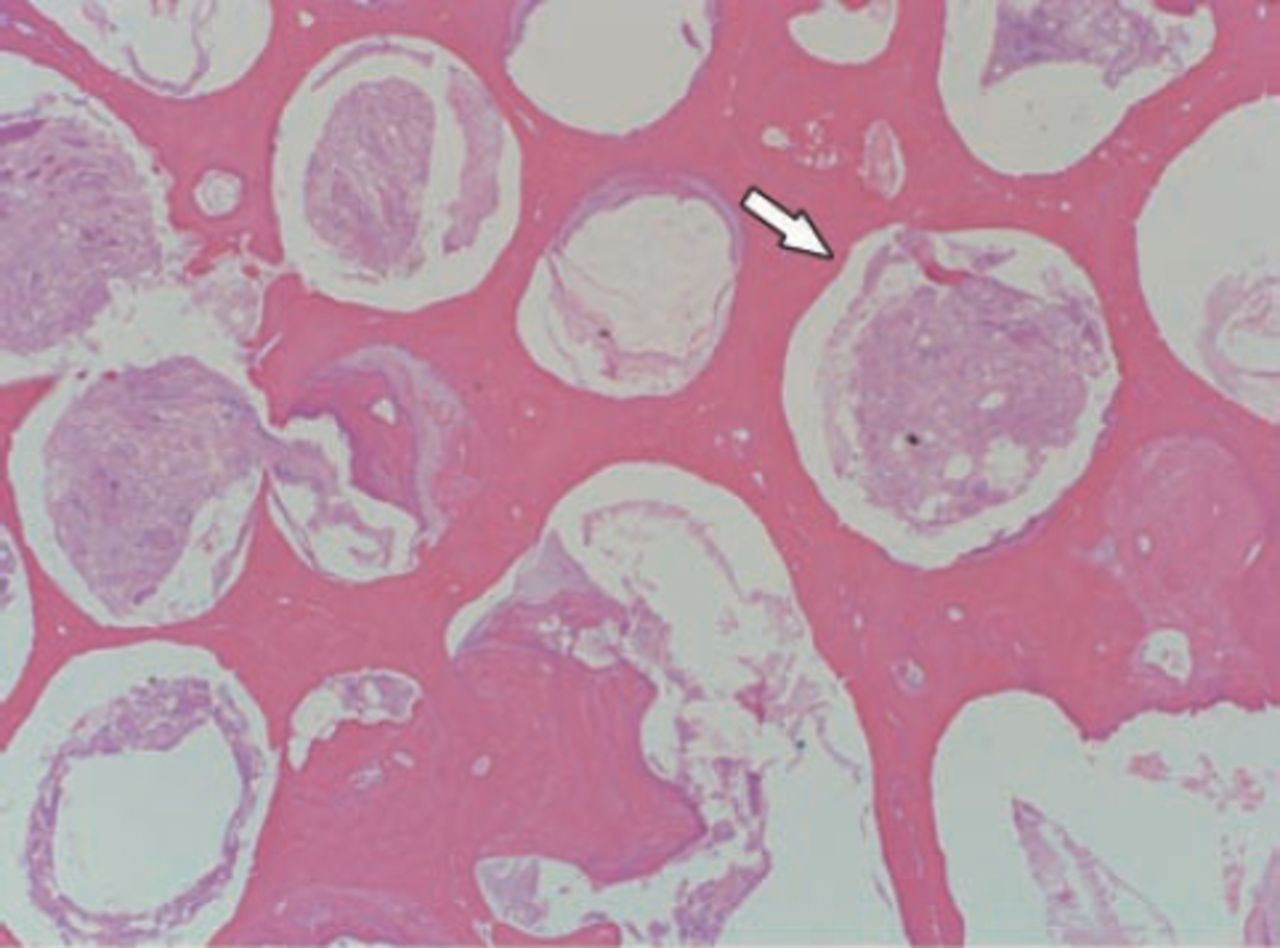
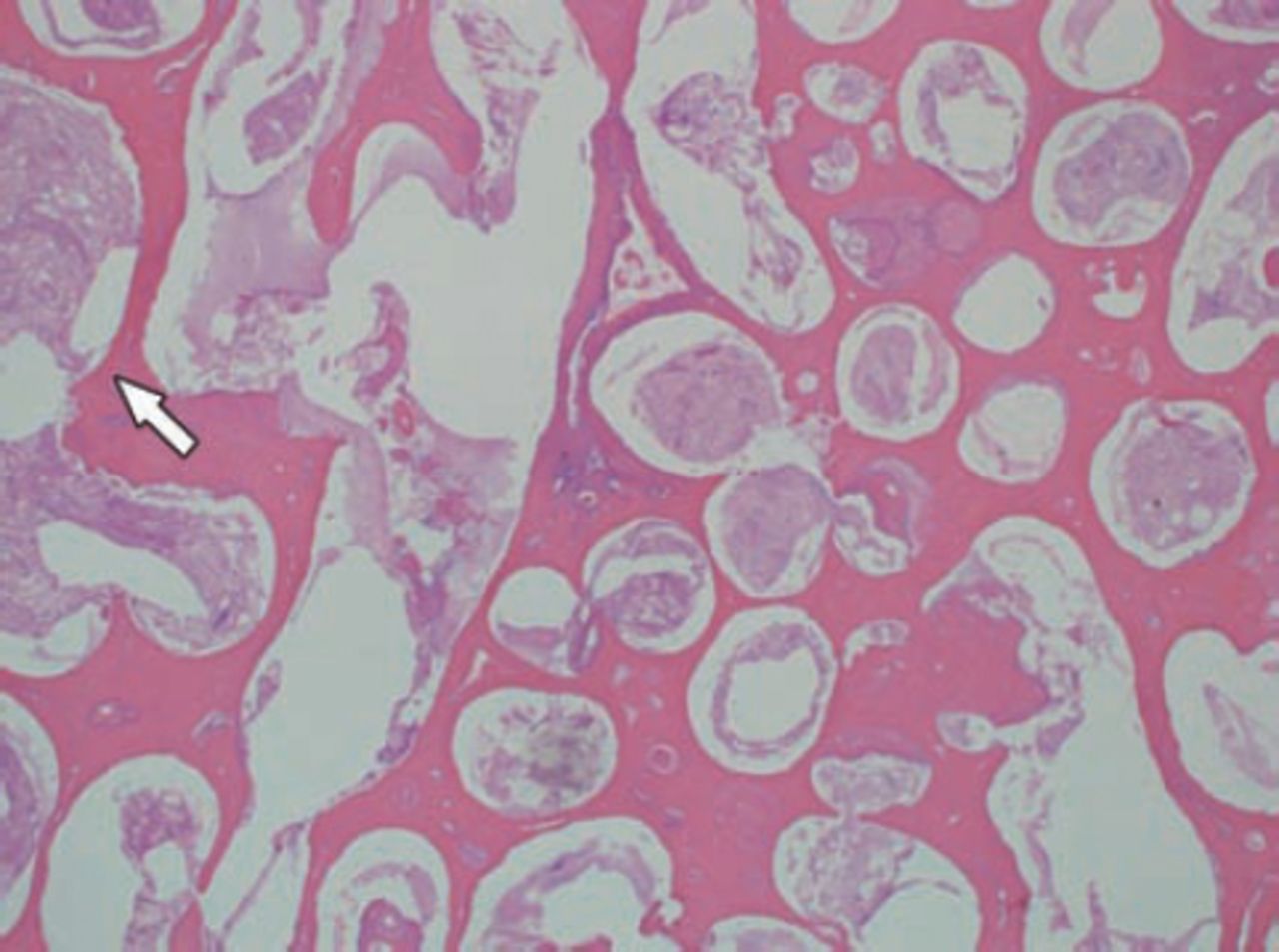
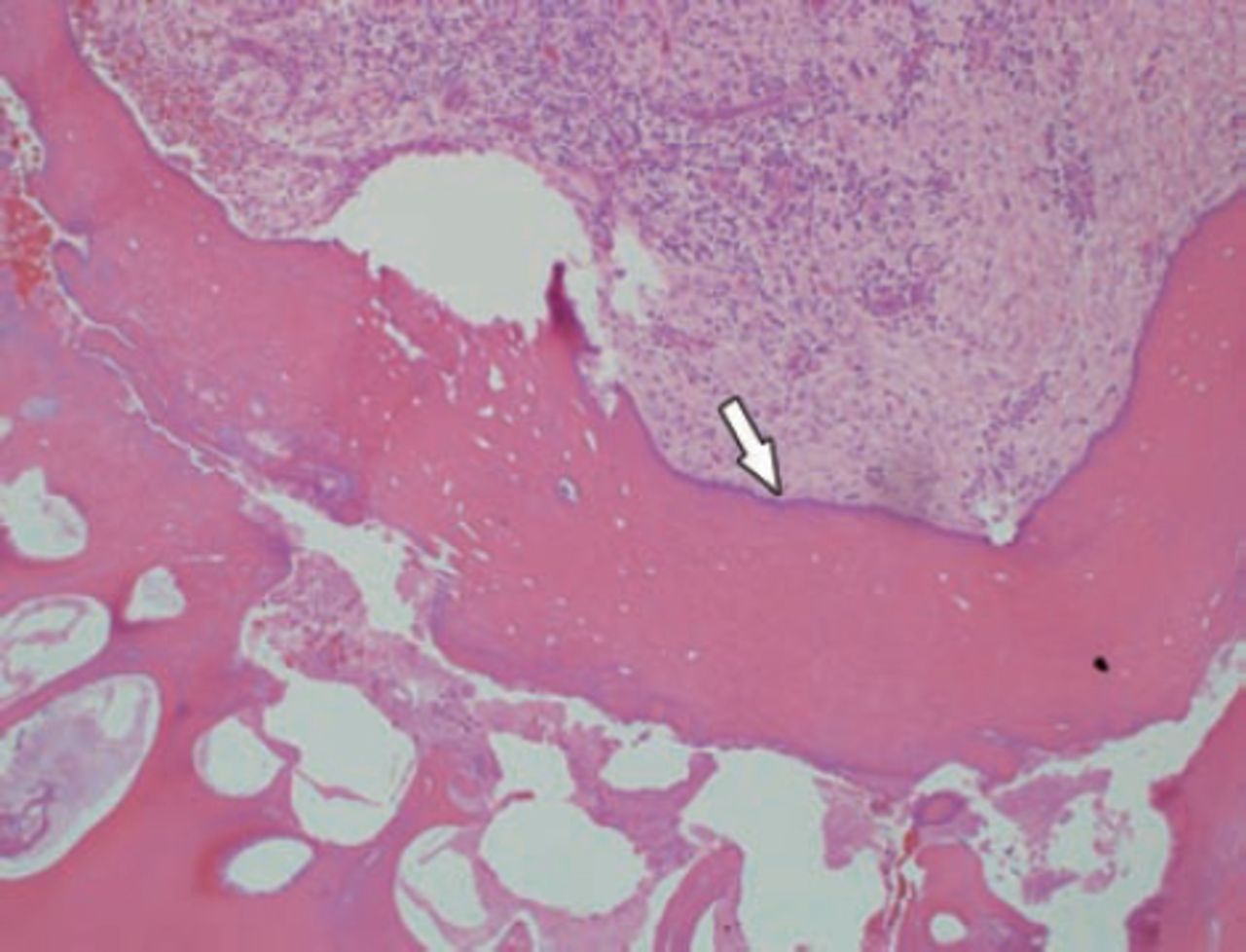
Histopathological section stained with hematoxylin and eosin stain of the complex odontome (arrow, higher magnification) showing the typical irregular arrangement of dentine, enamel matrix, cementum, and pulp-like connective tissue.
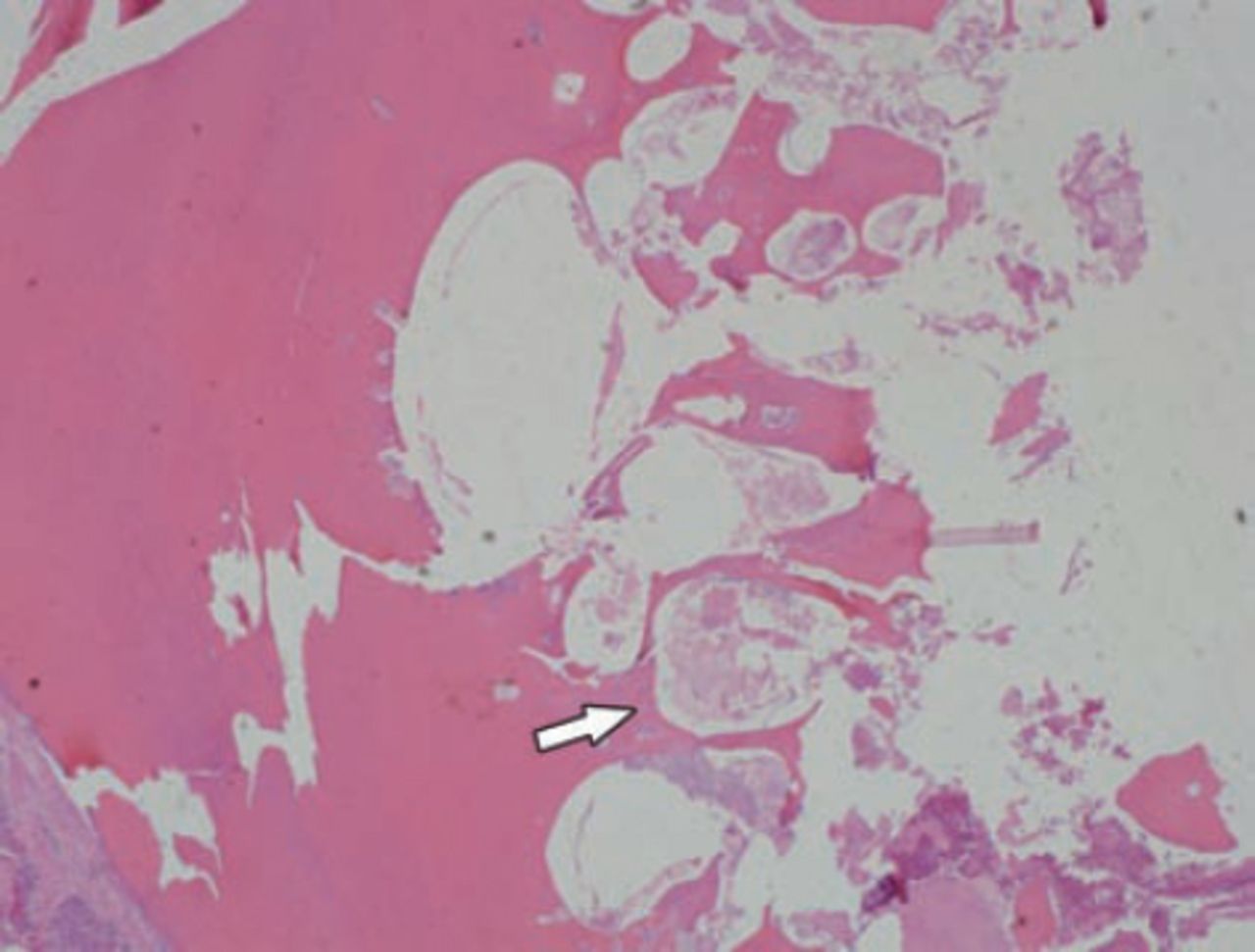
Photomicrograph of the decalcified section of odontoma stained with hematoxylin and eosin stain showing irregularly deposit mature tubular dentin, enclosing clefts and hollow circular spaces of decalcified enamel, and enamel matrix (arrow).
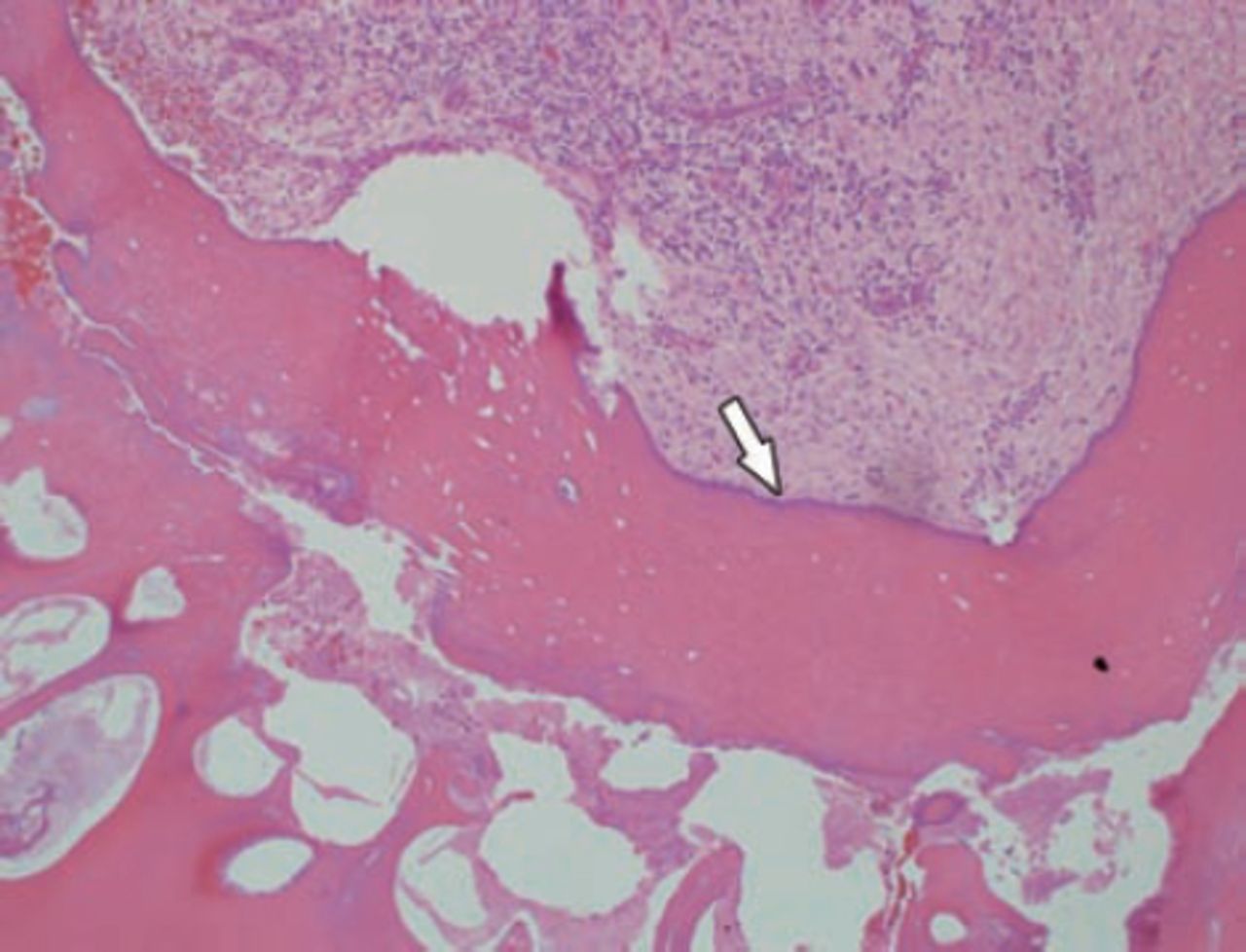
Histopathological decalcified section stained with hematoxylin and eosin stain showing irregularly deposited mature tubular dentine, enclosing enamel, and enamel matrix clefts with connective tissue simulating the normal pulp and cementum were also evident in a few areas in a haphazard desposition of dental tissue was consistent with the diagnosis of a complex odontoma (arrow).
Discussion
Erupting odontomas are initially intra osseous or central odontomas that later on become extra osseous or erupted. However, the mechanism behind the eruption in the case of erupting odontomas remains uncertain as some odontomas erupt at a young age and others at an older age. To date, most of the reported erupted odontomas are related to non-erupted teeth; it may, therefore, be postulated that the eruptive force of these teeth plays an important role in odontoma eruption.4 Eruption at a younger age is therefore possible through bone remodeling that might have resulted from the presence of dental follicles.3 The mechanism of odontome eruption appears to be different from tooth eruption because of the lack of the periodontal ligament in the odontome. Therefore, the power required for the eruption of odontomas is not linked to the contractility of fibroblasts, as is the case for teeth. Although there is no root formation in the odontome, its increasing size may lead to the sequestration of the overlying bone and hence, leads to eruption.5 The increase in size of the odontoma over time produces a force sufficient to cause bone resorption.3 Another reason for odontoma eruption could be the bony remodeling of the jaws. However, for this to occur a dental follicle is required, although indirectly, as it provides both the conductance and chemo attraction for the osteoclasts necessary for tooth eruption. Immunocytochemical investigations have indicated that the pattern of cellular activity involving both reduced dental epithelium and the follicles is associated with tooth eruption. The reduced dental epithelium initiates a cascade of intercellular signals by expressing epidermal growth factor β and transforming growth factor. These factors, in turn, stimulate the follicular cells to produce colony-stimulating factor, which recruits osteoclasts to the follicle. The reduced dental epithelium also secretes proteases, which assist in the breakdown of the follicle to produce a path of least resistance. The epithelial signaling could, therefore, explain the remarkable consistency of eruption times as it is likely that the dental epithelium is programmed as part of its functional life cycle.3 While in elderly cases where eruption odontomas were not related to impacted teeth or are located in edentulous ridges it was postulated that it is likely that resorption of the edentulous part of the alveolar process plays a role, but it is also possible that reactive growth of the capsule contributes to this phenomenon.2,5
To date, only 23 cases of erupted odontomas have been documented in the literature with the first case being described in 1980 by Rumel et al.1 Histopathologically, of the 23 reported cases of erupted odontoma, an almost equal frequency was noted of complex odontomas with 12 cases being diagnosed as compound odontomas2,4-9 as compared with 11 complex odontomas.2,3,6 Fifteen females (65%) were more affected as compared with 7 males (30%), with one case where the patient’s age and gender were not determined.2-10 The patients’ age ranged from 9 to 65 years, with a mean age of about 26 years confirming an age prediction of these lesions between the second and third decades of life.2,7 The clinical signs and symptoms of erupting odontoma includes association with delayed eruption, impaction and/or altered eruption of adjacent teeth in over 66% of the cases due to the obstruction of the eruptive trajectory of these adjacently related teeth.2,3,6,10 Pain, swelling, infection, and adjacent tissues suppuration were the most common symptoms, due to the spontaneous emergence of odontomas into the oral cavity and the exposure of the tumor through the oral mucosa inflammation of the adjacent soft tissues, or infection associated with suppuration.2,3,5,6 Other symptoms include anesthesia in the lower lip, swelling in the affected area, and even facial asymmetry.3 Pain as the first symptom was rarely reported, and it is probably due to secondary infection that can occur because of replacement of bone by a large amount of avascular hard tissue.3 The secondary infection may also be due to the explosion of an odontoma through the mucosa that allows the invasion of oral micro-organisms into the bone due to lack of adequate adhesion between bone and odontoma, due to absence of periodontal ligament. Other reported signs and symptoms including; pain, swelling, tongue irritation,3 facial asymmetry,3 malocclusions,2,6 halitosis,2 and recurrent infections were recorded.2,3 The age of the reported case is 24 years, which agrees with the average age of the reported cases that showed that the eruption of odontomas are more common between the second and third decade of life.2,6 Furthermore, the patient’s male gender adds more to the frequency of males (33), as compared with 62.5 females in the reported series.5-9
Histopathologically, our reported case added another complex odontoma case to equalize the frequency of complex odontoma as compared with the compound ones in the published series.5-9 Reviewing the reported cases of eruption odontome, most of them are of small size with the exception of only 2 cases that closely resemble our case in size and being large enough to be examined both visually and manually; these are the cases reported by Junquera et al2 and Vengal et al.3 The case of Vengal et al3 shares a great similarity with our case in both size, presentation, location, as well as diagnosis, while the case reported by Junquera et al2 was a maxillary lesion in the area of upper second molar tooth. Similarly; our reported case agrees with other cases where erupted odontomas, especially if they are of a large size and present with associated repeated infection, halitosis, displacement, and impaction of related teeth.2-10
In conclusion, a rare case of large erupted complex odontoma in a 24-year-old Saudi patient is presented. Pain, repeated infection, and halitosis were the most commonly reported symptoms. The eruption odontoma was located distal to the lower right second molar tooth associated with an impacted distally placed third molar. The related gingival tissues are inflamed in relation to the rough surface of the odontome. The treatment carried out was excision of the lesion and disimpaction of the wisdom tooth under local anesthesia. The case presented represents the third large eruptive odontome that can be examined both manually and visually. The presenting signs and symptoms and the value of radiographic and histopathological examination in achieving proper diagnosis is emphasized.
Copyright
Whenever a manuscript contains material (tables, figures, etc.) which is protected by copyright (previously published), it is the obligation of the author to obtain written permission from the holder of the copyright (usually the publisher) to reproduce the material in Saudi Medical Journal. This also applies if the material is the authors own work. Please submit copies of the material from the source in which it was first published.
Acknowledgment
The author would like to thank the Department of Histopathology of Prince Sultan Military Medical City for their help in preparing and photographing the histopathology slides. The author is also grateful to Professor H. A. Mosadomi, Riyadh Dental and Pharmacy Colleges, for review and diagnosing the histopathology slides.
- Received October 9, 2014.
- Accepted November 3, 2014.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.