


Abstract
Solitary fibrous tumors (SFT) of the upper limb are extremely rare, and we report this tumor in the arm of a 30-year-old male. He is presented with a 22 cm painless mass. Complete surgical excision was performed. The histological diagnosis of SFT was based on the presence of ectatic blood vessels and positive staining for CD34 and vimentin. He remains disease-free at the 3-year follow-up interval. The report aims to increase the awareness of the criteria for the histological diagnosis of SFT, as well as the principles of their surgical excision and follow-up.
Solitary fibrous tumors (SFT) are rare spindle-cell mesenchymal tumors, which are also known as fibrous mesotheliomas. As the name implies, the tumor is mainly seen in the pleura, the mesothelial lining of the lungs. In 5% of cases, it is accompanied by hypoglycemia secondary to tumor production of insulin-like growth factor II; and this is most often seen in tumors located in the pelvis and retroperitoneum.1 The majority of the tumors are histologically benign; however, atypical features have been described in some, and malignant cases have been reported.2 Extra thoracic SFT are very rare, and those involving the upper limb are extremely rare. In 2003, Akisue et al3 reviewed the literature on SFT of the limbs and could only find 9 cases involving the upper limbs. Since 2003, few other upper limb tumors have been reported.2,4-7 Our objective in presenting this particular case is to increase awareness, and focus on the criteria for histological diagnosis of SFT, as well as the principles of their surgical excision and follow-up.
Case Report
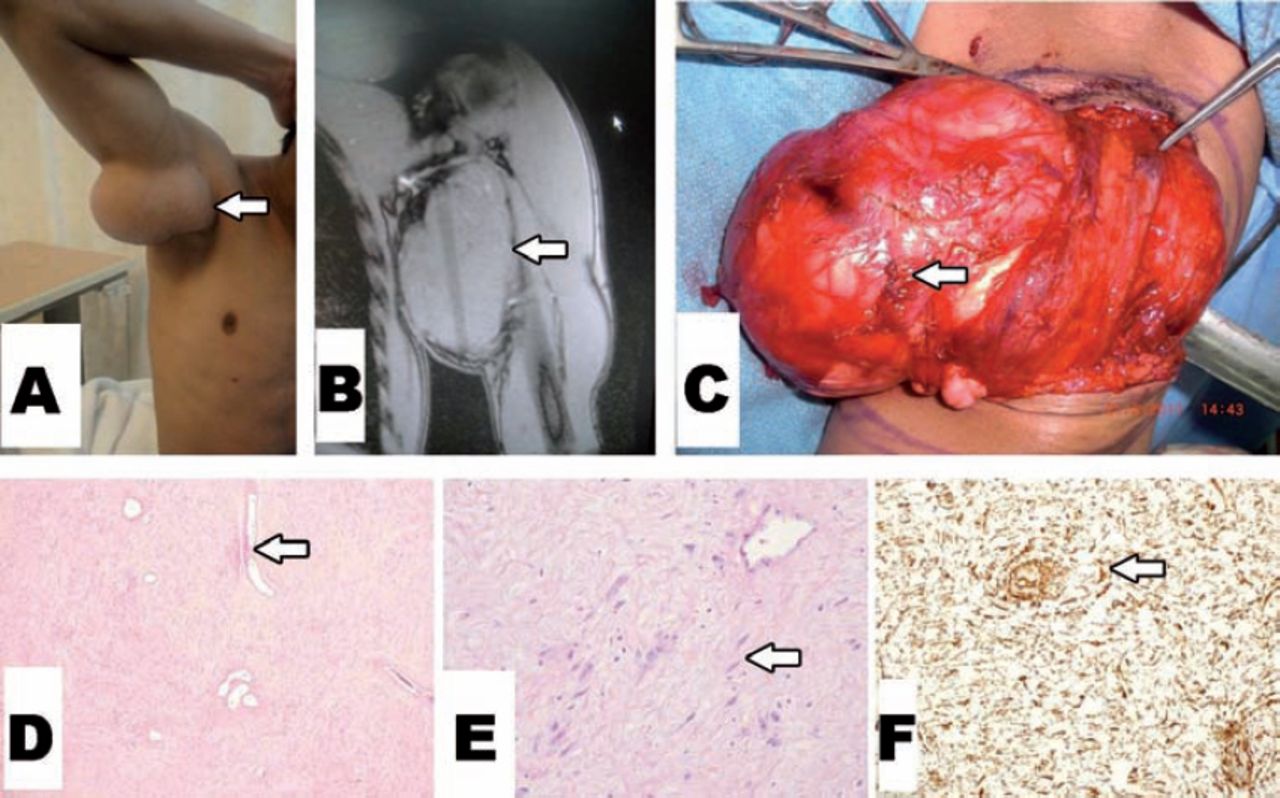
A 30-year-old man presented with a one-year history of a slowly growing mass of the left upper-medial arm (Figure 1A). There was no pain or neurovascular-related symptoms. On MRI (Figure 1B), a well circumscribed mass with intermediate signal intensity on T1 and T2 weighted images was seen. A metastatic work-up including CT scan of the chest and ultrasound of the abdomen was negative. Surgical excision was performed under general anesthesia. A well-circumscribed tumor was found with a firm whitish capsule (Figure 1C). The tumor mass along with the capsule was excised. The mass measured 22 × 10 cm and cut-sections showed a multi-nodular mass with a smooth surface feature. Histological examination showed a benign hypocellular fibrous tumor with ectatic blood vessels (Figure 1D); composed of fibroblasts separated by thin bands of collagen (Figure 1E). There were no areas of tumor cell necrosis, and mitotic figures were rare. There was no pleomorphism or atypia. All resection margins were free of tumor. Tumor cells stained positive for CD34 (Figure 1F), and vimentin; and negative for desmin, actin, cytokeratin, and S-100 protein. The final diagnosis was a benign solitary fibrous tumor. He did well after surgery and after 3-years is disease free.

Clinical photo showing: A) preoperative appearance, B) MRI showing an iso-intense mass, C) surgical excision of the mass along with its capsule, D) the tumor is hypocellular with ectatic blood vessels (hematoxylin and eosin stain x40), E) high power showing the fibroblasts surrounded by thin collagen (hematoxylin and eosin stain x200), and F) positive CD34 immunostain (x100).
Discussion
Solitary fibrous tumors of the upper limb are extremely rare, and less than 20 cases were reported in the literature.2-9 Historically, SFT were known as hemangiopericytomas because the presence of stag-horn vascular pattern was thought to be an indication of a pericytic origin. Later, this stag-horn vascular feature was found to be present in several other benign, and malignant tumors such as infantile myofibromatosis, and synovial sarcoma.10
The differential diagnosis of SFT is a long list of benign fibrous tumors that are known to affect the upper limb of children and adults. All benign fibrous tumors are mainly composed of fibroblasts (spindle cells) separated by collagen bands. The diagnosis of the type of tumor will be based on other histological features and on immunohistological analysis.11,12 An accurate histological diagnosis is essential because it will determine the behavior, risk of recurrence, and the adequacy of surgical resection. For example, nodular fasciitis has a very low risk of recurrence and may even regress spontaneously; while desmoid tumors are locally aggressive with a high risk of recurrence and hence require wide local excision. The diagnosis of nodular fasciitis is based on the presence of myxoid areas and positivity for actin staining, while desmoid tumors are positive for desmin staining. Therefore, an experienced histopathologist is an essential member of the team for managing fibrous tumors of the limb. The most characteristic histological feature of SFT is the presence of ectatic or stag-horn blood vessels; although other distinct histologic patterns have been described.6 Furthermore, SFT cells will stain positive for CD34 and vimentin; and will stain negative for actin, desmin, and other epithelial (such as cytokeratin), and neural (such as S-100 protein) markers. Finally, all benign-looking fibrous tumors should be carefully examined for any areas of atypia or polymorphism. These features suggests the presence of a malignant component, and Baldi et al13 have reported a distant metastases from tumors with such features. The tumor in our patient had no such features. However, it should be emphasized that histological features will not always predict biological behavior.
Surgically, the tumor mass should be removed along with its capsule since failure to do so is associated with increased risk of local recurrence.14 Other factors that are known to be associated with local recurrence include positive surgical margins, accidentally going through the capsule during surgery, high cellularity, and the presence of frequent mitotic figures.13 None of these features were present in our patient and there was no local recurrence through the 3-year follow-up visit. Long-term follow-up is recommended for benign SFT since they may have a very slow growth, and late recurrences have been reported.13 The histological features of the tumor of our patient are associated with a low risk of recurrence, and surgical excision was curative. Long-term follow-up is planned for our patient.
In conclusion, we report a rare case of SFT of the upper limb and emphasize the principles of excision, the diagnostic criteria, and follow-up of similar cases. Excision should include the capsule surrounding the tumor mass. The diagnosis should be confirmed by the presence of stag-horn vessels and positivity for CD 34 and vimentin. Long term follow up is required even for tumors with rare mitotic figures.
Case Reports
Case reports will only be considered for unusual topics that add something new to the literature. All Case Reports should include at least one figure. Written informed consent for publication must accompany any photograph in which the subject can be identified. Figures should be submitted with a 300 dpi resolution when submitting electronically or printed on high-contrast glossy paper when submitting print copies. The abstract should be unstructured, and the introductory section should always include the objective and reason why the author is presenting this particular case. References should be up to date, preferably not exceeding 15.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This work is supported and funded by the College of Medicine Research Center, Deanship of Scientific Research, King Saud University, Riyadh, Kingdom of Saudi Arabia.
- Received October 19, 2014.
- Accepted December 15, 2014.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.