


Abstract
Objectives: To identify the problems and principles of treatment decisions in treatment-naïve limited-stage small cell esophagus carcinoma (LD-SCEC).
Methods: Clinical data from 39 patients with LD-SCEC treated in the Chinese People’s Liberation Army General Hospital, Beijing, China between 2000 and 2013 were retrospectively collected with regard to pathologic characteristics, overall survival (OS), and relevant prognostic factors.
Results: The median OS was 21.1 months (95% confidence interval [CI]: 12.4-29.7 months). The one-year OS was 76%, 3-year was 25%, and the 5-year OS was 8%. Depth of invasion, lymph metastasis status, and chemotherapy were independent prognostic factors. Of the 39 cases, only 38.4% (15 cases) were diagnosed as SCEC by the biopsy specimen. Eight of the 15 patients (group A) received chemotherapy and/or radiotherapy, while the remaining 7 patients (group B) and the other 24 patients (group C) received surgery as initial treatment. The one-year survival of group A was 87%, of group B was 69%, and of group C was 74% (p=0.037). The accuracy of the biopsy diagnosis influenced the treatment decisions and prognosis.
Conclusion: Small cell esophagus carcinoma is a systemic disease, with depth of invasion, lymph metastasis status, and chemotherapy as independent prognostic factors. Systemic therapy based on chemotherapy is recommended. The top priority is to improve the accuracy of diagnosis before deciding on the initial treatment option.
Small cell esophagus carcinoma (SCEC) is characterized as highly aggressive with poor prognosis, and represents 0.8-3.1% of all esophageal cancers and approximately 2.5-4.1% of all small cell carcinomas (SCECs).1,2 It has been increasingly recognized that SCEC is a clinicopathological entity with an absolutely different biological behavior and prognosis distinct from squamous and adenocarcinomas of the esophagus, but similar to small cell carcinoma that arises in the lung and other extrapulmonary organs.3-5 The clinical course of these tumors is highly aggressive in general, with early dissemination, frequent recurrences, and poor prognosis. Even with improved diagnostic capabilities, the diagnosis is still difficult in some cases, especially poorly differentiated squamous or adenomatous carcinoma, because of the small biopsy sample.6,7 Little research has focused on the influence of the diagnosis on the treatment choice, and whether the result of the biopsy pathology affects the therapy chosen or not is still unknown. Small cell esophagus carcinoma has commonly been treated with multimodality therapies, including surgery, chemotherapy, and radiotherapy.8 However, the role of surgery in the management of limited-stage SCEC is still under debate. Lv et al9 reported that SCEC was a systemic disease, and systemic therapy, based on chemotherapy, and radiotherapy, was recommended, but other researchers suggest that radical esophagectomy with extended lymphadenectomy should be considered as the initial treatment for patients with limited-stage SCEC.10 Because of the paucity of cases and a lack of large studies, the management of limited-stage SCEC (LD-SCEC) is still under exploration. The aims of the study were to analyze the characteristics and prognostics of treatment-naïve SCEC and, if possible, to identify the problems and principles of treatment decisions of treatment-naïve SCEC.
Methods
The Ethics Committee of The Chinese People’s Liberation Army (PLA) General Hospital approved this retrospective study, which was performed according to the principles of the Helsinki Declaration. Since it was a non-randomized retrospective prognosis analysis, and the data were de-identified and analyzed anonymously, the ethics committee waived the need for consent.
Patient selection
We retrospectively reviewed 6542 cases of carcinoma of the esophagus or gastric-esophagus (GE) junction at the Chinese PLA General Hospital, Beijing, China from January 2000 to January 2013. Among these 6542 cases, 70 patients were diagnosed as small cell carcinoma of the esophagus or GE junction. The World Health Organization histological criteria for small cell carcinoma were adopted. All cases were reconfirmed by a senior pathologist in the Chinese PLA General Hospital. Of these 70 patients, 26 patients were confirmed as extensive-stage disease, 5 patients were lost to follow up after the surgery. Finally, a total of 39 patients were selected for this study. The eligibility criteria for patients were as follows: 1) histopathologically proven SCEC or small cell gastric-esophagus carcinoma, 2) proven limited-stage disease, 3) without neoadjuvant therapy. The exclusion criteria as follows: 1) history of previously treated cancer other than basal or squamous cell carcinoma of the skin 2) incomplete medical records. Finally, a total of 39 patients were enrolled for analysis in this retrospective study.
All patients received an endoscopic biopsy before treatment. Staging workup included a physical examination, chest radiography, barium meal, CT scan of the abdomen and brain, B ultrasound of the cervical lymph node, and radioactive isotope bone scans. Unless clinically indicated, brain MRI was not routinely performed. Complete blood count, blood biochemistry analyses, and liver and renal function evaluations were also performed. For the 8 patients who did not receive surgery, the depth of tumor invasion was evaluated by endoscopic ultrasonography (4 patients), contrast-enhanced CT (3 patients), and MRI (one patients).
At this point in time, there is no specific staging system for SCEC. The disease stage is presented as either a Limited-stage disease (LD) or an extensive-stage disease (ED) according to the Veteran’s Administration Lung Group’s 2-stage classification scheme (VALSG) for primary pulmonary SCEC.11 Limited-stage disease is defined as a tumor confined within a localized anatomical region, which can be safely encompassed within a radiation field. Extensive-stage disease is defined as a tumor outside local regional boundaries. To find prior related research, a literature search was performed in MEDLINE from January 1, 1960 to August 30, 2014, by 2 independent investigators. We searched the related studies with the following text words: “esophagus carcinoma,” or “esophagus cancer,” or “esophagus tumor” or MeSH “esophageal neoplasms” and “small cell cancer” or “small cell carcinoma” or “small cell tumor” or MeSH “carcinoma, small cell”. Only articles written in English were included in the current study.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows version 21 (IBM Corp, Armonk, NY, USA). The survival rate was calculated by the Kaplan-Meier method, and the log-rank test was used to assess differences in survival between groups. Patients who were lost to follow-up were defined as censored values at the last time of contact. Patients who were still alive at the end of the study were also classified as censored values. A Cox proportional hazards regression was used to examine the independent prognostic factors. Relative prognosis was summarized using estimates and 95% confidence intervals (95% CI) for the hazard ratio. A 2-sided probability value of less than 0.05 was considered to be statistically significant.
Results
Patient characteristics
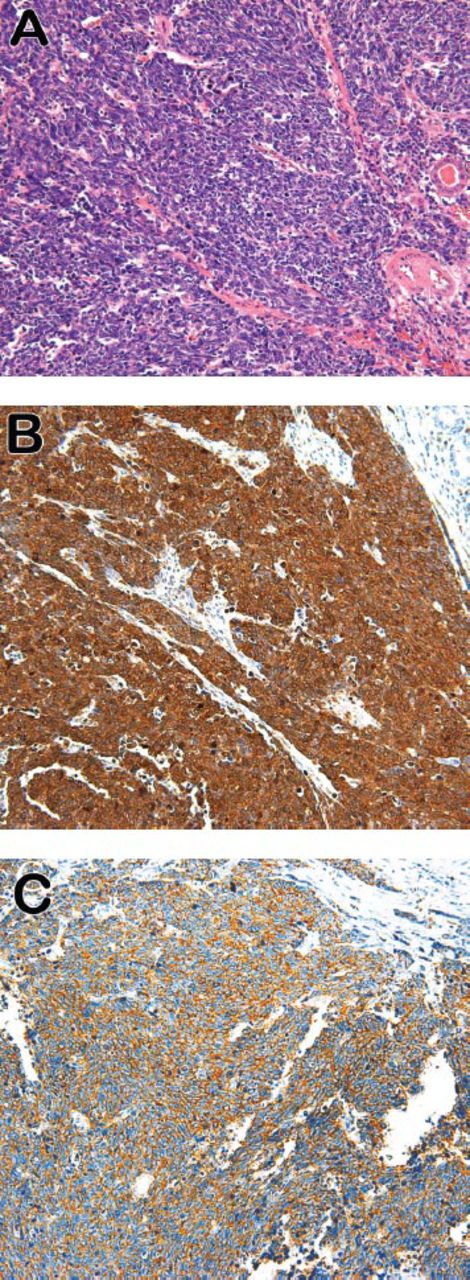
In total, 39 patients were identified in our institute. Their general characteristics are listed in Table 1. All the patients received biopsy before the treatment. Of those patients, 6 cases failed to gain the pathology diagnosis, 18 cases were diagnosed as non-small cell carcinoma, and only 15 of the 39 cases were diagnosed as SCEC by the biopsy specimen. Only 38.4% (15/39 cases) of patients showed a definitive diagnosis by the biopsy specimen. A typical case is presented in Figure 1. Histopathologic assessment revealed that the tumor consisted of small cancer cells with dense chromatin nuclei. Immunohistochemically, the tumor cells were positive for neuron specific enolase (NSE) (Figure 1B) and synaptophysin (Figure 1C). The pathological stage could be exactly defined in 31 patients who underwent surgical resection. The median tumor length was 4 cm (range 0.9-11 cm). According to the American Joint Committee on Cancer (AJCC) TNM Classification of Carcinoma of the Esophagus and Esophagus-gastric Junction,12 8 cases were stage T1; 9 cases were stage T2; 4 cases were stage T3; and 10 cases were stage T4. Sixteen cases (51.6%) of lymph node metastasis were detected among the 31 patients. Of the 8 patients who did not receive surgery, the evaluation of stage was assessed by endoscopic ultrasonography and/or imaging tests examination. Among those patients, 3 cases were stage T1-T2; 5 cases were stage T3-T4; 3 cases were lymph node metastasis positive; and 5 cases were lymph negative.
Characteristics of 39 patients enrolled in the study period.

Histological and immunohistochemical assessment of small cell carcinoma A) Hematoxylin and Eosin (H&E) staining demonstrated small cells with hyperchromatic nuclei and scant cytoplasm (original magnification × 200); B) & C) the tumor cells showed positive immuno-staining intensity for neuron specific enolase and synaptophysin (original magnification × 200).
Treatment
The choice of initial therapy depended on the pathology and performance status. Of the 15 cases diagnosed as SCEC by the biopsy, 6 patients received chemotherapy and sequential radiotherapy, 2 patients received concurrent chemoradiotherapy (those 8 patients were defined as group A), the remaining 7 patients (defined as group B), and the other 24 patients who were undefinably diagnosed (defined as group C) received surgical treatment as initial therapy.
Of the 31 patients who received surgical resection, 26 cases were treated by esophagectomy with 2-field lymph node dissection (the mediastinal and perigastric lymph nodes), 3 cases were treated by the cervico-thoraco-abdominal procedure, and 2 cases received explorative resection. Cervical lymphadenectomy was not systematically performed in this series. There were 3 cases that underwent incomplete resection, one case of R1 resection, and 2 cases of R2 resection.
Thirty-three patients received platinum-based regimens. Five cases received a 3-drug combination therapy, and the others received double drug therapy. Regimens evolved from cisplatin plus vincristine (2 cases) to cisplatin or carboplatin plus etoposide plus 5-fluorouracil or not (25 cases), and further to irinotecan plus cisplatin (3 cases), and docetaxel plus cisplatin (2 cases), one patient received alternating regimens (etoposide plus cisplatin and etoposide plus ifosfamide). A median course of 5 (range, 2-8) rounds of chemotherapy was given.
Of the 39 patients, 17 received radiotherapy, 10 were as adjuvant radiotherapy. The target volume covered the primary lesion or the tumor bed with regional lymph nodes. The median dose of radiotherapy was 50Gy (rang 40-60Gy). No patients received prophylactic brain irradiation.
Outcome and survival analysis
By May 2014, with a median follow-up of 25.5 months (3-66 months), 26 patients (61.8%) had died, 9 (29.4%) were still alive, and the other 4 patients had been lost to follow-up. The median overall survival time (OS) was 21.1 months (95 CI: 12.3-30.0 months). The one-year OS was 76%, the 3-year OS was 25%, and the 5-year OS was 8%. The available recurrence data is shown in treatment failure part of Table 1. Local recurrence was detected in 11 patients, including the primary site (3 cases) and regional lymph nodes (9 cases). Distant metastases were seen in 15 patients; 4 cases occurred in the bone, 5 cases in the lung and 10 cases occurred in the liver, 3 cases showed more than one site metastasis. Only one case got metastasis in the brain.
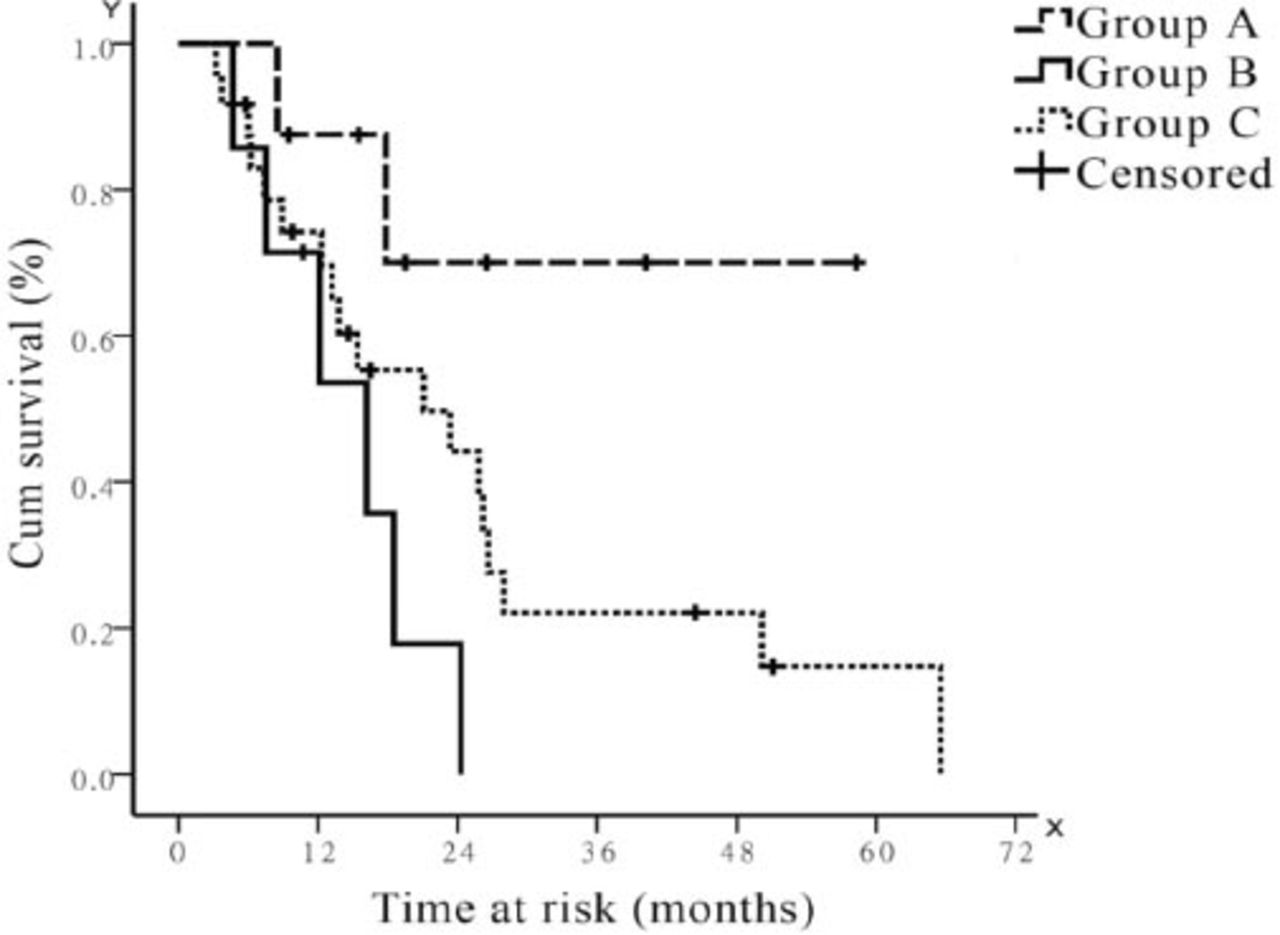
Of the patients in group A, 3 patients achieved complete remission and 4 achieved partial remission, and in one patient the disease was assessed as stable. Only 2 patients showed recurrence, one of them acquired a new metastasis in the lung, and the other showed recurrence in the cervical lymph nodes. For group B, the median survival was 16.2 months, which was similar to group C (OS = 21.1 months, p=0.119), but worse than group A (p=0.019, Figure 2). The one-year survival of group A is 87%, of group B is 69%, and of group C 74% (p=0.037).
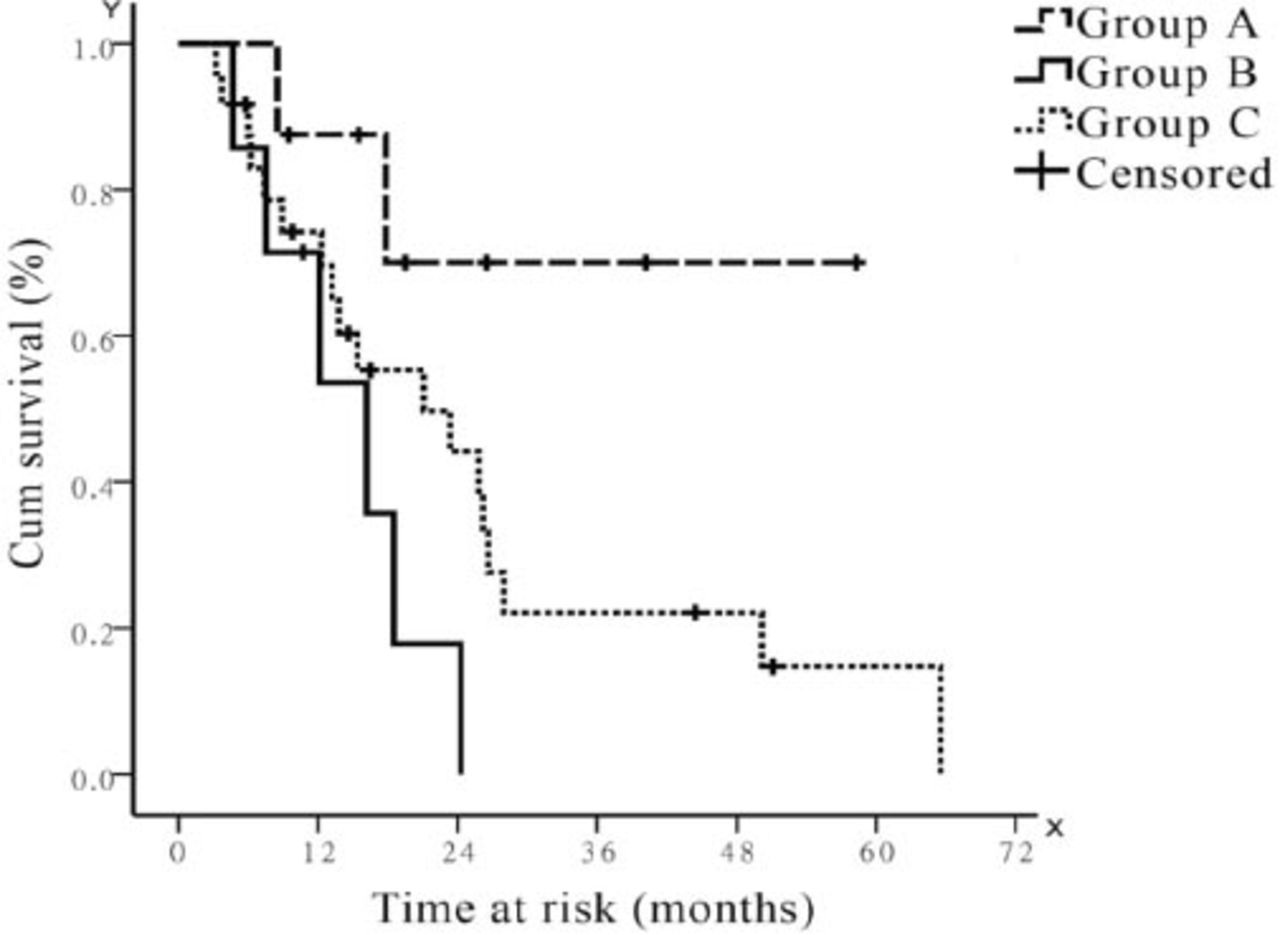
Survival according to the different biopsy pathology and treatment. Group A - patients were diagnosed with small cell esophagus carcinoma (SCEC) by the biopsy, and received chemoradiotherapy without surgery as initial treatment; Group B - patients were diagnosed with SCEC by the biopsy, and received surgery as initial treatment; Group C - patients with poorly differentiated carcinoma-not otherwise specific or negative pathological findings of the biopsy and received surgery as initial treatment. The media overall survival of Group A was unreached, and was 16.2 months for Group B and 21.1 for Group C. Among the 3 groups, p=0.037; Group B versus Group A, p=0.019; Group B versus Group C, p=0.119; Group C versus Group A, p=0.089.
According to the sample size and clinical evaluation, age, gender, surgery, radiotherapy, chemotherapy, depth of invasion, and lymph status were analyzed in the multivariate cox regression model. The multivariate cox regression analysis for the 39 patients demonstrated that deep depth of invasion, positive lymph metastasis, and treatment without chemotherapy were independent factors decreasing OS (Table 2).
Multivariate overall survival analysis by Cox’s proportional hazards mode.
Discussion
Small cell esophagus carcinoma is a rare and highly aggressive malignancy. Approximately 1,000 new cases of SCEC are diagnosed yearly in the USA, which represents 2.5-5% of small cell cancer cases.13 Since the first 2 cases of SCEC were reported by McKeown in 1952,14 several prospective studies have focused on this rare disease. The reported median survival for the LD-SCEC various from 14 months to 21 months, which was similar to this study (median OS: 21.1 months). In this study, the one-year OS was 76%, the 3-year OS was 25%, and the 5-year OS 8%, which is also similar to the reported data (the one-year OS 51-58%, 3-year OS 13.2%-30%, 5-year OS rate 7.8-18%).1,2,8,15-18 The multivariate analysis of our data shows depth of invasion, and positive lymph metastasis were independent prognostic factors, which was also confirmed by other studies.1,2,9,18 Although the general characteristics and prognostic factors of SCEC patients were similar to those in previous studies, some interesting issues are exposed in this study.
Chemotherapy, but not surgery was also proven to be an independent prognostic factor in this study. This indicates that SCEC is a systemic disease and systemic therapy based on chemotherapy should be recommended. In this series, the first-line regimen was various treatments. Four cases received CE/PE, 2 cases received DP, one case received EPF, and one case received NP. The overall objective response rate of 8 patients without surgical treatment was 87.5% (7/8 case), which is comparable to the reported result of 90% in some studies.8,19 The combination of etoposide and platinum compound was the most widely used and sensitive regimen for SCEC. A case-control study found that regimens containing platinum improved overall OS compared with regimens without platinum.18 However, no optimal first-line regimen was available for treatment-naïve patients until now, and all the results were analyzed. Prospective randomized clinical trials and further meta-analysis is needed to prove this hypothesis. For patients with resectable limited-disease, the role of surgery is still controversial.10,20 In this study, patients who did not receive surgery as initial treatment (group A) had the best OS, and better than group B and group C who received surgery. Indicating that surgery was not necessary for all of the treatment-naïve LD-SCECs. The SCECs have a similar biological behavior and prognosis as small cell lung cancer (SCLC). Parallel data from patients with SCLC indicate that a combination of chemotherapy and radiation alone can cure a small subgroup of patients, and the optimal treatment for patients with limited-staged SCLC is concurrent chemoradiotherapy.21 Although some literature espouses surgery for patients with SCEC, there is no question that patients can be cured without it.2,8,18 However, the short- and long-term health related quality of life is deeply affected after esophagectomy for cancer. The recovery period after esophagectomy can exhaust more than half, if not all-of this life expectancy. Among esophagus carcinoma patients, quality of life was worse at 6 weeks after an esophagectomy than it had been preoperatively, and most quality of life indicators improved to their preoperative level only after 9 months.22,23 Due to the efficacy of chemoradiotherapy and limitations of surgery, surgery is not indispensable and needs to be reevaluated by the multidisciplinary team before the initial treatment of LD-SCEC.
One of the most important factors to determine the treatment option is the pathological diagnosis. However, the diagnosis is very difficult, particularly in those that are considered poorly differentiated.16,24 In this series, the most difficult problem was the accuracy of diagnosis. The clinical manifestations of SCEC are similar to those of non-small cell carcinoma (non-SCEC) of the esophagus.6,9,17 The differential diagnosis is dependent on histopathological examination. Because of the small amount of preoperative tissue in the present series, some patients were pathologically diagnosed preoperatively as having non-SCEC, but postoperatively as SCEC. Only 15 of the 39 patients received the exact diagnosis of SCEC,8 of these 15 patients received chemoradiotherapy without surgical treatment and obtained greater benefit than the remaining 31 patients who received surgical intervention as the initial treatment. Surgical treatment was overused in those patients, but the fundamental problem was the poor preoperative diagnostic accuracy. The accuracy of biopsy diagnosis influenced the treatment decisions and prognosis. Since tumor cells may not be detectable in biopsy specimens, tumor cells proliferate in the submucosal layer in many cases, endoscopic ultrasound-guided fine needle aspiration should be employed and other efforts and methods should be developed to increase the diagnostic yields of submucosal lesions.25,26
Another interesting situation was brain metastasis. For patients with SCLC, brain metastasis was found in 10-18% at the time of diagnosis, but the incidence of brain metastasis increased from 50-80% at 2 years post treatment, and was the main reason for treatment failure.27 Brain metastases in SCEC is not as common as SCLC, reportedly in only 4.5% (1/22 cases) to 5.5% of patients (7/127 cases) in other studies.18,28 In this present study, none of those patients received prophylactic brain irradiation, and only one patient developed brain metastasis. The most frequent sites of distant failure were the liver and bone metastases. Given this low incidence, prophylactic brain irradiation for SCEC seems unnecessary.
Study limitations
Due to the rarity of the tumor, the number in each subgroup was very small, especially for the subgroup diagnosed as SCEC by the biopsy. The small numbers suggest that the results need to be further confirmed. However, because of the rarity of SCEC, it is difficult to conduct prospective, randomized controlled trials to assess optimal treatment. Meta-analysis maybe another way to assess the right treatment choices, and more studies are needed to undertake this. In addition, the retrospective nature must be considered in interpreting our data.
In conclusion, SCEC is a systemic disease, with depth of invasion, lymph metastasis status, and chemotherapy as independent prognostic factors. Systemic therapy based on chemotherapy is recommended. Surgery is not indispensable. The accurate of biopsy diagnosis will influence the treatment decisions and prognosis, so therefore, the top priority is to improve the accuracy of diagnosis before a decision is made on the initial treatment options.
Illustrations, Figures, Photographs
Four copies of all figures or photographs should be included with the submitted manuscript. Figures submitted electronically should be in JPEG or TIFF format with a 300 dpi minimum resolution and in grayscale or CMYK (not RGB). Printed submissions should be on high-contrast glossy paper, and must be unmounted and untrimmed, with a preferred size between 4 × 5 inches and 5 × 7 inches (10 × 13 cm and 13 × 18 cm). The figure number, name of first author and an arrow indicating “top” should be typed on a gummed label and affixed to the back of each illustration. If arrows are used these should appear in a different color to the background color. Titles and detailed explanations belong in the legends, which should be submitted on a separate sheet, and not on the illustrations themselves. Written informed consent for publication must accompany any photograph in which the subject can be identified. Written copyright permission, from the publishers, must accompany any illustration that has been previously published. Photographs will be accepted at the discretion of the Editorial Board.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This project was supported partially by the twelfth five years’ medical science project of PLA (CWS12J120).
- Received December 22, 2014.
- Accepted January 5, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.