


Abstract
Objectives: To identify the epidemiology, pattern, outcome, and impact of infant burns in Eastern Saudi Arabia.
Methods: We conducted a retrospective review of admitted infants charts over 4 years (2008-2013) at the Burn Unit of King Fahad Hospital, Hofuf, Al-Ahsa, Saudi Arabia. The charts were reviewed for age, gender, etiology, site of injury, total body surface area (TBSA), depth of burn, hospital stay, and discharge status.
Results: The total number of admissions to the Burn Unit was 510 cases. Out of these cases, 84 were infants, constituting 16.5% of total admissions. Scald burn was the most common etiology affecting 73 infants (86.9%). The highest percentage of total body surface area was between 5-10%, which occurred in 41 infants (48.8%). The average hospital stay was 10 days. No infant mortality was reported during this period.
Conclusion: The prevalence of burns among infants in our hospital is high, and preventive measures must be implemented to decrease the occurrence of burns in this age group.
Al-Ahsa is the largest governorate in Saudi Arabia’s Eastern Province, with a population of 1,079,156 people in 2010.1 Saudi Arabia is a young populated country, as 30.7% is below the age of 14.2 The number of pediatric burns is reportedly high in Saudi Arabia, mostly due to household hazards or due to habits that can be a possible burn source such as drinking tea and coffee from hot pots.3,4 Limited data is available on infant burns, worldwide.5 There is a scarcity of published data on infant burns from Saudi Arabia. The aim of this study is to identify the epidemiology, pattern, outcome, and impact of infant burns in eastern Saudi Arabia. Determine the burden of infant burns on the hospital by determining the number of infant admissions, and length of stay in the hospital. Finally start a preventive measures and public awareness to decrease the incidence of these burns.
Methods
We conducted a retrospective review of the clinical charts of 510 consecutive burn patients admitted to the Burn Unit of King Fahad Hospital, Hofuf, Al-Ahsa, Saudi Arabia over 4 years between 2008 and 2013. All infants aged 12 months or less admitted to the Burn Unit during this period were included in the study. No infants were excluded. The charts were reviewed for age, gender, etiology, site of injury, total body surface area (TBSA), depth of burn, hospital stay, and discharge status. A literature review for previous burn publications from Saudi Arabia was conducted using the Medline database (PubMed) using the key words: Burn [ti] OR Burns [ti] AND Saudi [ti]. The results were reviewed for any infant burn studies.
The data was collected and entered on a Microsoft Office Excel sheet. Data was analyzed using the Excel 2013 built in statistics tools. Confidence intervals and one tail t test were calculated were applicable. P values equal to or less than 0.05 was considered significant.
The study was conducted according to the Principles of the Helsinki Declaration and approved by the King Fahad Hospital Research and Ethical Committee, and the Ministry of Health Research and Studies Committee.
Results
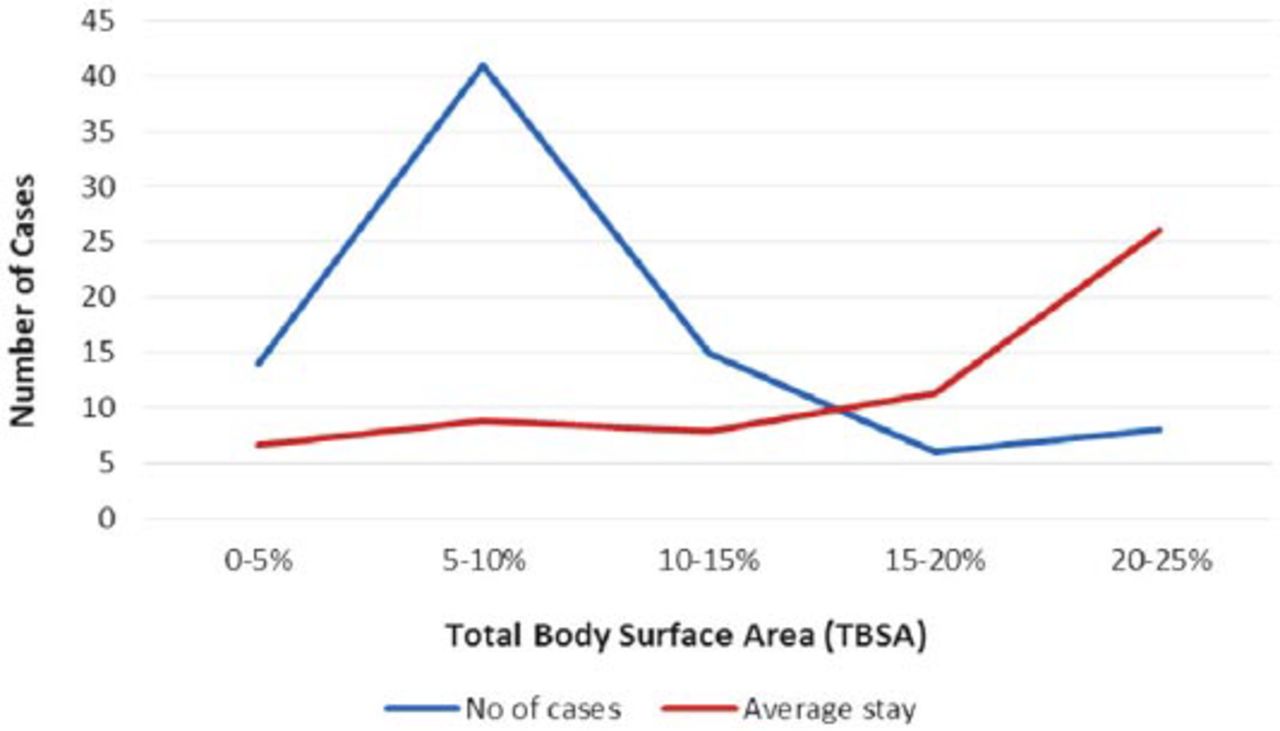
A total of 510 burn cases were admitted during the study period. Out of these admissions 203 (39.8%) were children (less than 12 years), and 307 (60.2%) were adults, there were 84 infants (less than one year), constituting 16.5% of total admissions, and 41.4% of the pediatric age group. Analysis showed that scalds represented the major etiological factor affecting 73 cases (86.9%), followed by flame with 5 cases (6%) (Figure 1). Figure 2 shows infant burn etiologies as a percentage of total admissions, and a percentage of total pediatric admissions. The most frequently encountered total body surface area (TBSA) affected was between 5-10%, which occurred in 41 infants (48.8%). The minimum TBSA affected was 1%, which occurred in one infant. The maximum admitted TSBA affected among admitted infants was 25%, which occurred in 3 infants (Table 1). Table 2 summarizes the number and percentage of body parts recorded among the admitted infants. The upper limb was the most affected body part, recorded in 45 infants (54.2%). The trunk was second with 43 infants (51.8%). Infants with upper limb burns had a higher age (mean±SD) of 10.9±2.17 months compared with infants with no upper limb burn (9.6±2.85 months) p<0.02 using one tail t test. More males (52 infants, 61.9%) were admitted than females (32 infants, 38%) with a ratio of 3:2. The burn age has 2 peaks the first peak was in the 8-month-old infants, with a total of 8 infants (9.5%), and the second peak was in the 12-month-old infants with a total of 51 infants (60.7%). The average hospital stay was 10 days for the 75 cases who were discharged routinely. Nine cases where excluded from the calculation of hospital stay because they were discharged against medical advice. The highest category was between 1-5 days accounting for 36% (27 cases), followed by 6-10 days accounting for 28% (21 cases). When TBSA was compared with length of stay, the lowest average (±SD) stay days was 6.6±5.95 days for the 0-5% TBSA category, and the highest was for the 20-25% category with an average of 26.1±10.37 days (Figure 3). The average stay days were higher when the trunk was involved (11.4 days) compared to 8 days when trunk was not involved (p<0.03) using one tail t test. From the 84 infants, 75 (89.3%) were discharged by their physician after proper treatment was completed. While the remaining 9 (10.7%) were discharged against medical advice by their parents, or shifted to another hospital. No infant mortality was recorded during the study period (Table 3).

Types of burn among 84 infants admitted in the Burn Unit of King Fahad Hospital, Hofuf, Al-Ahsa, Saudi Arabia.

Percentage of infant burn types from the total and pediatric admissions.
Infants burn total body surface area 84 infants admitted to the Burn Unit of King Fahad Hospital, Hofuf, Al-Ahsa, Saudi Arabia.
Affected body part in 84 infants admitted to the Burn Unit of King Fahad Hospital, Hofuf, Al-Ahsa, Saudi Arabia.
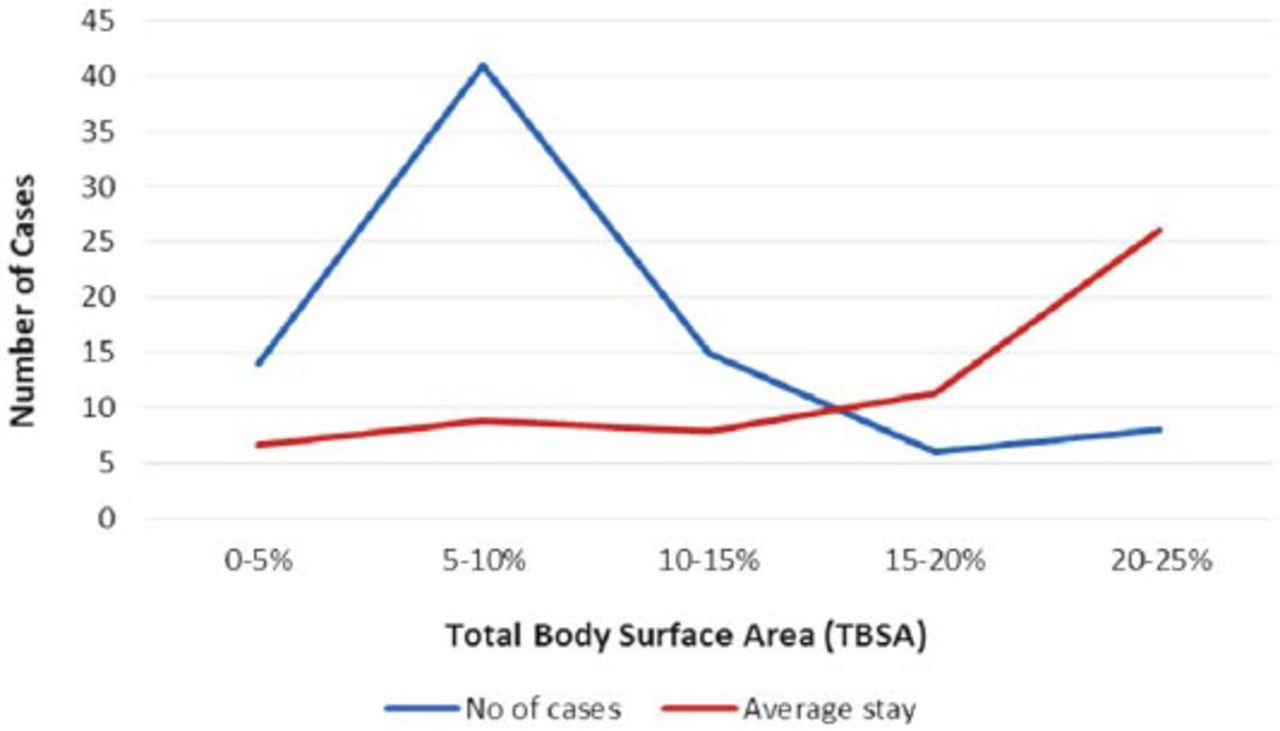
Correlation of number of admissions and total body surface area (TBSA) and stay days of 84 infants admitted to the Burn Unit of King Fahad Hospital, Hofuf, Al-Ahsa, Saudi Arabia.
Type of burn with type of discharge among 84 infants admitted to the Burn Unit of King Fahad Hospital, Hofuf, Al-Ahsa, Saudi Arabia.
Discussion
The paucity of data on burn injuries in infants initiated our 4-year study. A recent publication on infant burns, and literature review by Laitakari et al5 reviewed only 6 previous publications that addressed infant burns. Our review of the literature revealed no previous publications in Saudi Arabia on infant burns except for a publication by Al-Qattan,6 who reported on the treatment of 53 infants with palm burns due to camp fire injures. Our study included 84 infants admitted over a period of 4 years, which constituted 16.5% of all admissions, and 41.4% of pediatric admissions to the Burn Unit. This percentage is higher than Laitakari et al’s review,5 which reported the highest percentage was 30% of pediatric admissions. Laitakari’s own study showed that only 3% of pediatric admissions were infants.5 Scalding was the most common cause of burns at 86.9%. This is consistent with previous studies in which all reported scalding as the most common etiology.5,7,8 Most of these scalds are attributed to the use of hot water during bathing or cleaning. However, a study carried out on infants referred to the emergency department by Lorch et al,8 showed a different pattern of scalding, with the common cause of scalding being hot beverages and soup.8 Unfortunately, in the current study we were unable to determine the common cause of scalding due to inadequate details in the files of reviewed cases.
However, based on the knowledge of Al-Ahsa community habits, hot water from bathing and personal cleaning in toilets in our community is the most likely cause. Water hoses are used for self-cleaning after toilet and they are usually installed low and infants can reach them. Mothers also use water for cleaning their babies after a wet or soiled diaper. Previous studies did not report any perineum burns, however, in our study the perineum (either the only area burned, or part of the burned areas) was involved in 11 infants (13.3%, Table 2).5,8 The differences in cleaning practices within societies is an important factor for burns among infants. The use of an appropriate hot water supply and equipment is important as reveled by Kubilius et al3 who noticed increased scalding burns among pediatrics where hot tap water is not available due to the use of hot water for household duties.
While contact burns were the second most common cause among infants in previous studies, flame burn was second in our study.5,7 Chemical burns were not common, and only reported by Nguyen et al,4 in which flame, chemical, and radiation were the cause in only 5 infants (5%). This difference in pattern may be due to the local practice of using campfires, as reported by Al-Qattan,6 wood and coal for local methods of cooking, and using chemicals for opening blocked sewage lines at homes. The hand was the most common body part affected in previous studies, followed by the trunk.5,8 Our study is consistent with these studies. We classified the body as upper and lower limb, trunk, and perineum. The upper limb was the most affected followed by the trunk. We grouped infants into groups, with and without upper limb burns, and the second with and without trunk burns. When the upper limb was involved the average ± SD age was higher (10.9±2.17 month), compared with infants with no upper limb burns (9.6±2.85 months). This was also reported by Nguyen et al, and can be attributed to mobility and motor development of the older infants, as this may be a risk factor as published by previous studies.4,9 Trunk involvement resulted in a higher stay-days average (11.4 days) compared with 8 days when the trunk was not involved. The trunk association with higher stay days was not reported in previous study. Trunkal involvement is associated with higher TBSA involvement, and thus more stay-days. The peaks of increased burn around the eighth and twelfth month (Figure 4) is only noticed in our study, although Nguyen et al4 reported increased burns with older infants.4 The TBSA involvement varies among all previous studies as reviewed by Laitakari et al.5 Some studies ranged from 0.5-38% as in Nguyen et al’s study,4 and 0.5-40% in Laitakari own study.5 Our range was from 1-25% with the most common involvement being between 5-10%. Nguyen et al4 reported that 94% of contact burns were small and were very small and ranged from 0-1% TBSA. Most of the previous studies reported that they admit infant to the burn unit even with small TBSA, this low threshold to admit low TBSA is that even a 0.5% burn in an infant may require special care and considered a significant injury to an infant, especially if it is on the hand or perineum. There are many limitations to our study. This study addressed infant admissions to the burn unit, but the true number of infants treated for burns in the emergency department and discharged, or those whose parents refused to admit them to the burn unit is unknown. Also, the exact mechanism of the burn, and the place where the burn occurred was not properly recorded in the admission papers. No other data on the socioeconomics of the family, the number of siblings, literacy of parents, and so forth was collected.

The peaks of increased burn around the eighth and twelfth month in 84 infants admitted to the Burn Unit of King Fahad Hospital, Hofuf, Al-Ahsa, Saudi Arabia.
In conclusion, infant burns should be properly reported and studied, as the etiology of these burns are different from other age groups. Preventive measures should focus on the etiology of these burns based on community habits and behavior, such as the use of campfire and wood or hot water during infant cleaning. Future study should include other important variables that contribute to burns in infants, like socioeconomics and literacy of parents.
Acknowledgment
We express our acknowledgment to the King Fahad Hospital Research and Ethical Committee and the Ministry of Health Research and Studies Committee for their help and guidance through the study process and publication.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 5, 2014.
- Accepted January 12, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.