


Abstract
Objectives: To investigate the epidemiology of pediatric hand fractures and to provide recommendations regarding prevention.
Methods: Medical records and x-rays were retrospectively reviewed for age at the time of injury, gender, fracture pattern, place where the injury occurred, and mechanism of injury. The study was conducted at King Khalid University Hospital, Riyadh, Saudi Arabia between January 2005 and December 2011.
Results: Of 361 cases reviewed, there were 291 (80.6%) male and 70 (19.4%) female patients. Most (46.2%) were in the age group of 13-18 years. For age group 1-4 years, the most common place of occurrence was at home (81.3%) and for the group 13-18 years, outdoors was the place of occurrence (64.7%). Females were mostly injured at home while males had similar distribution of indoor and outdoor injuries. The most common causes of fractures were: door slams in the 1-8 years age group; falls at home, in the 9-12 years age group; and both falls at home and sports in the oldest age group (13-18 years). The little finger ray are the most frequently injured part of the hand followed by the middle finger.
Conclusion: Our series showed that most hand fractures in children occurred at home, which requires reevaluation of home settings. Implementation of safety measures during sports activities are relevant in the oldest age group.
Childhood is the most important period in the development of healthy individuals. Among 1-18 year olds, 12% of 5.1 million global deaths from injuries in 2010 were due to unintentional injuries. For this pediatric age group, approximately 627,741 deaths were due to unintentional injuries in 2010.1 For unintentional injuries, falls rank second as a leading cause of mortality and account for 11% of worldwide, unintentional injury deaths.2 One study conducted at a hand center in England showed 663 hand fractures per 100,000 children aged 10-16 years.3 Injuries of the hand (including fractures) were among the most common injuries in the pediatric emergency departments in the United States of America.4 Severe hand fractures among children can lead to permanent loss of function and psychological trauma.5 Although there are several studies on pediatric upper limb fractures from different countries,6-26 little research has been conducted on primary prevention. Our literature search did not reveal any research on the prevention of hand fractures in Saudi children. A better understanding of the epidemiology of hand fractures in the pediatric age group is essential for effective preventive strategies development. In addition, there may be epidemiological variations in hand fractures among different populations, as some of these injuries depend on the environment, such as sports activities among local children. Various safety measures, such as compulsory use of protection during contact sports and implementation of playground safety, have been used in Western countries.3 We conducted a retrospective case series study to investigate the epidemiology of pediatric hand fractures among cases presenting to King Khalid University Hospital (KKUH) between 2005-2011. We aimed to describe the pattern of hand fractures in this age group and compare such fractures epidemiologically according to cause and place of injury. Finally, recommendations will be made regarding prevention.
Methods
We conducted a PubMed search to ensure that there were no previous studies on the epidemiology of pediatric fractures in children in Saudi Arabia aiming to give recommendations regarding prevention. The study was approved by the KKUH Institutional Review Board and the work was conducted according to the principles of the Helsinki Declaration.
The study was conducted at KKUH, Riyadh, Saudi Arabia (a tertiary facility with 800 beds). The hospital has a separate pediatric emergency department. As a standard practice, all patients with a suspected hand fracture undergo radiological examination of the injured hand. Although KKUH is a tertiary care institution, the emergency room accepts all Saudi nationalities and they are considered eligible for treatment and admission. This type of unrestricted eligibility for Saudi’s is also available in the Ministry of Health hospitals.
We conducted a retrospective chart review of all children (younger than 18 years old) who were diagnosed with hand fractures between January 2005 and December 2011. As it was difficult to verify the diagnoses from the medical records department, cases were included by identifying them through the x-ray system. The x-ray system database was screened for the diagnosis of hand fractures; and we identified the number of cases from the medical records.
All hand x-rays performed during the study period was reviewed by a hand surgery consultant and all children with hand fractures were included. Children with finger-tip amputations, joint dislocations without fractures, and wrist fractures were excluded. The medical records of included cases were then obtained and the data was abstracted using a data collection tool specifically designed for the purpose of this study. This information included: age at the time of injury, gender, fracture pattern, place where the injury occurred, causes, and mechanism of injury. The fracture pattern was recorded by bone, site, and type. The place where the injury occurred was recorded as either indoor (at home) or outdoor (such as school, desert, and recreation places). The cause of injury was documented in relation to indoor or outdoor occurrence. Causes of indoor and outdoor injuries were also identified.
Missing information from the medical records regarding the place and cause of injury resulted in a smaller sample of cases with full information than intended to be collected (cases with missing information for every specific analysis were excluded for that analysis). Statistical analysis was performed using the IBM SPSS Statistics for Windows version 19.0 (IBMCorp, Armonk, NY, USA). We used Chi-square and Fisher’s exact tests to compare the indoor and outdoor groups and the males and females groups for different nominal variables. We used non-parametric binomial test to compare the percentages for demographic characteristics. A p-value of less than 0.05 was considered significant.
Results
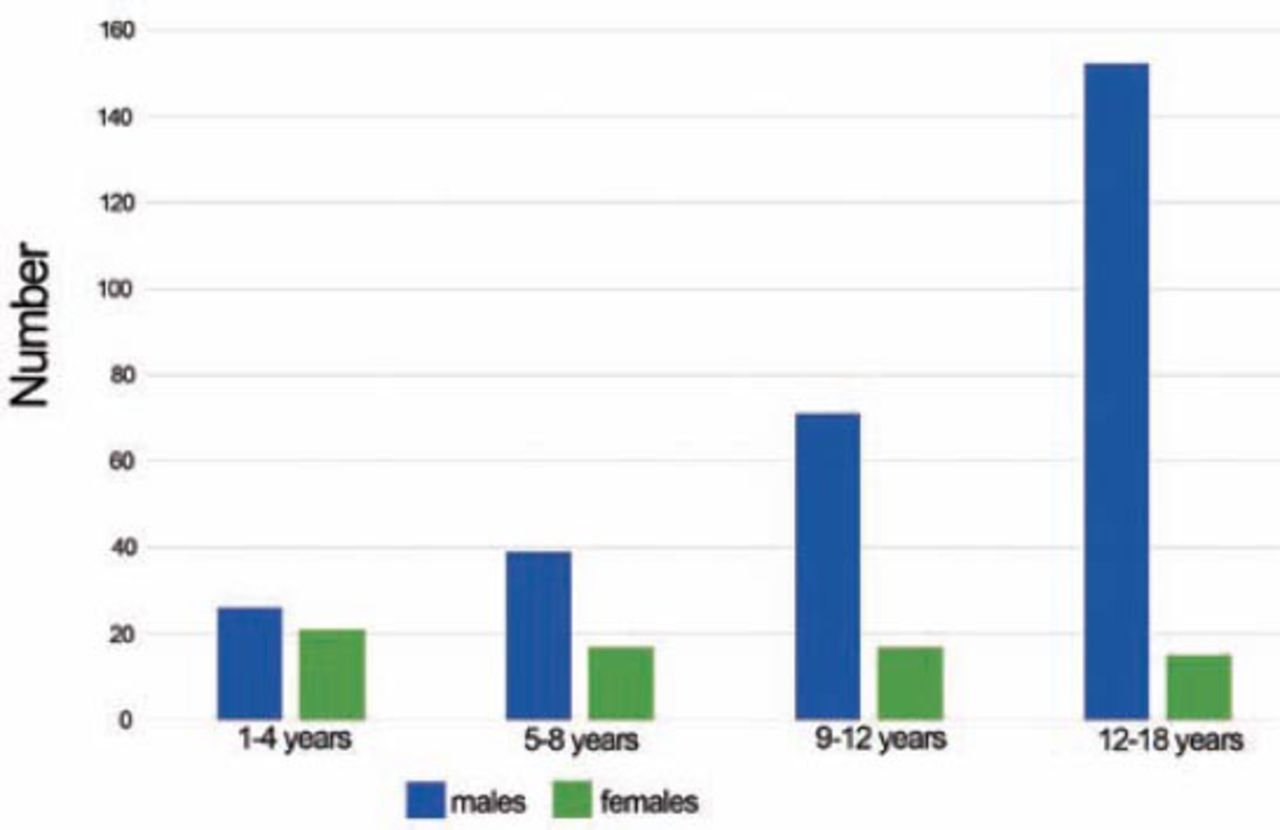
A total of 361 children met the inclusion criteria (Figure 1 & Table 1). There was a male preponderance with 291 (80.6%) male, and 70 (19.4%) female patients yielding a male to female ratio of 4.2 to 1 (p<0.0001). The mean age was 11 years, with an age range of 1-18 years. Most (46.2%) cases were in the age group 13-18 years and this was statistically significant (p<0.0001). The vast majority of patients with hand injuries were Saudi nationals (93.4%) (p<0.0001), which reflected the patient population seen in our medical center. The right and the left hands were almost equally affected in our series (p=0.307). Approximately 81.2% cases were attending and managed through the emergency room (p<0.0001), and most of the remaining cases were referred to the hand clinic for surgical management (Table 1). The place of hand fractures in our series was mostly at home for the age group 1-4 years old (81.3%) (p=0.007), but mostly outdoor in the age group 13-18 years old (64.7%) (p=0.007). Females were mostly injured at home while males had a similar distribution of indoor and outdoor injuries, but this did not reach statistical significance (p=0.069). The right and left hands were equally injured indoor and outdoor (p=0.648) (Table 2).

Age and gender distribution among 361 pediatric hand fracture cases in King Khalid University Hospital, Riyadh, Saudi Arabia, 2005-2011.
Socio-demographic characteristics of pediatric hand fractures in King Khalid University Hospital, Riyadh, Saudi Arabia (2005-2011).
Place of injury by age, gender and hand side in children presenting with hand fractures in King Khalid University Hospital, Riyadh, Saudi Arabia (2005-2011).
For the entire study population, the most common causes of indoor injuries were falls followed by door slams at home; while for outdoor injuries they were mostly due to sports (Table 3). We used the data in Table 3 for statistical analysis (using the non-parametric binomial test) to identify the most common causes of fractures in each age group aiming to identify the most significant risks for injury. Twenty-five out of 47 children (65%) in the youngest 2 age groups (1-8 years) sustained their hand fractures from door slams at home (p=0.029). In the intermediate age group (9-12 years), 17 out of 38 children (45%) sustained their hand fractures from falls at home (p=0.035). Finally, both falls at home and outdoor sports were the predominant causes (a total of 39 out of 55 children, or 71%) of hand fractures in the oldest (13-18 years) age group (p<0.0001).
Cause of injury by age group in children presenting with hand fractures in King Khalid University Hospital, Riyadh, Saudi Arabia (2005-2011).
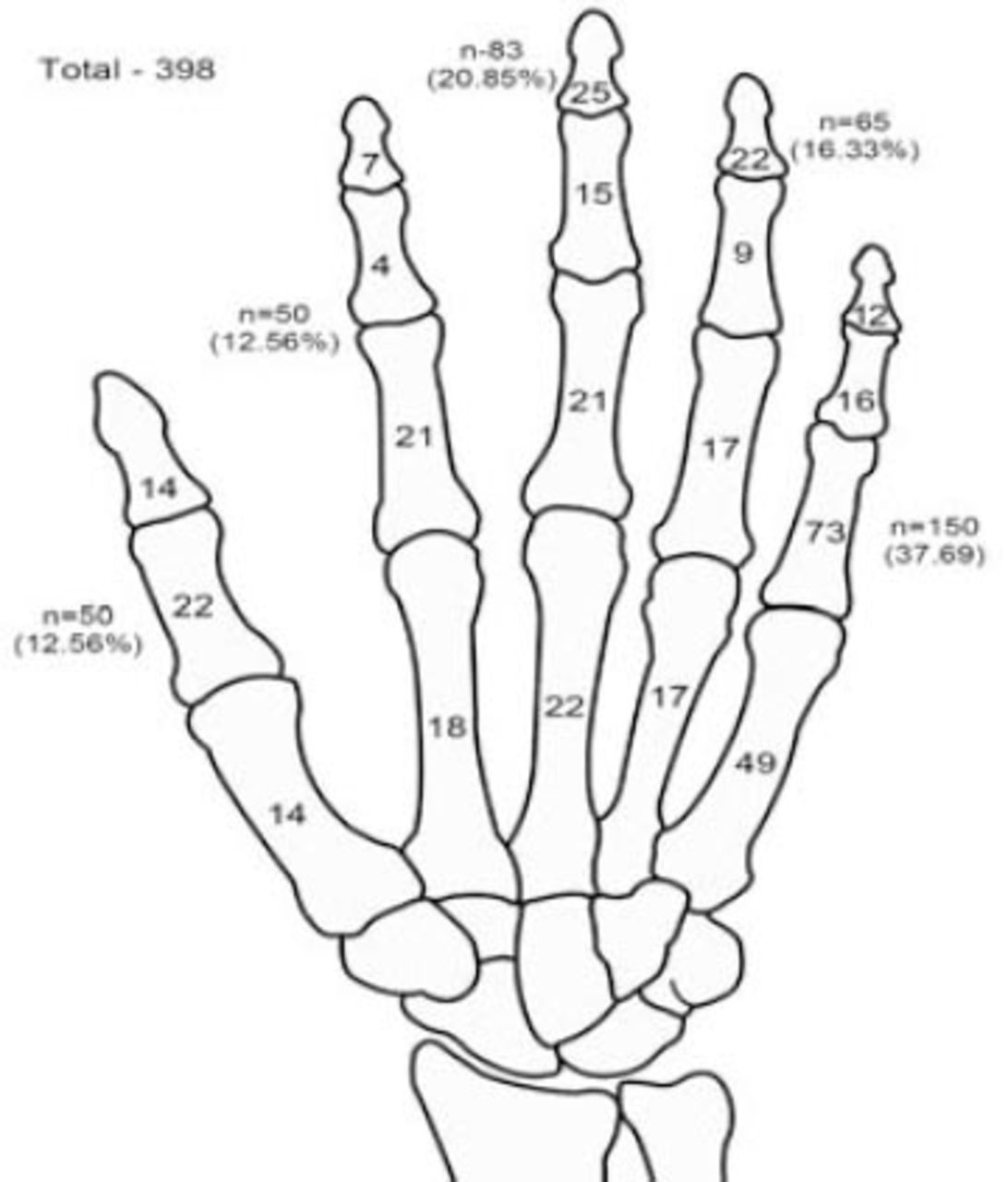
Table 4 shows the cause of fracture by gender. Among females, falls at home and door slams at home were 2 equally important causes for fractures. Among males, falls at home were the most frequent causes of injury followed by sports-related fractures (Table 4). All 24 children who sustained hand fractures during sports were males (p<0.0001). The most frequently fractured digit in the hand was the little finger (37.7%) followed by the middle (20.9%), and ring fingers (16.3%) (Figure 2). The most frequently injured bone was the proximal phalanx (n=154, 38.7%) followed by the metacarpal (n=120, 30.2%) (Figure 2). Across all age groups, the little finger ray was fractured the most, followed by the middle finger (Figure 3). The distribution of fractures within the little finger ray showed that the proximal phalanx was the most frequently fractured bone in the 5-8 years group (14 out of 19 little finger fractures, 73.7%) and in the 9-12 years group (21 out of 31 little finger fractures, 67.7%). However, the metacarpal was the most frequently fractured bone in the 13-18 years group (40 out of 82 little finger fractures, 48.8%) (Figure 3).
Cause of injury by gender in children presenting with hand fractures to King Khalid University Hospital, Riyadh, Saudi Arabia (2005-2011).

The distribution of hand fractures by bone among 361 cases. The total number of fractures is 398 as some cases had multiple fractures. Also note that the little finger is the most commonly injured ray (n=150 fractures), and the proximal phalanx of the little finger is the most commonly injured bone (n=73 fractures).
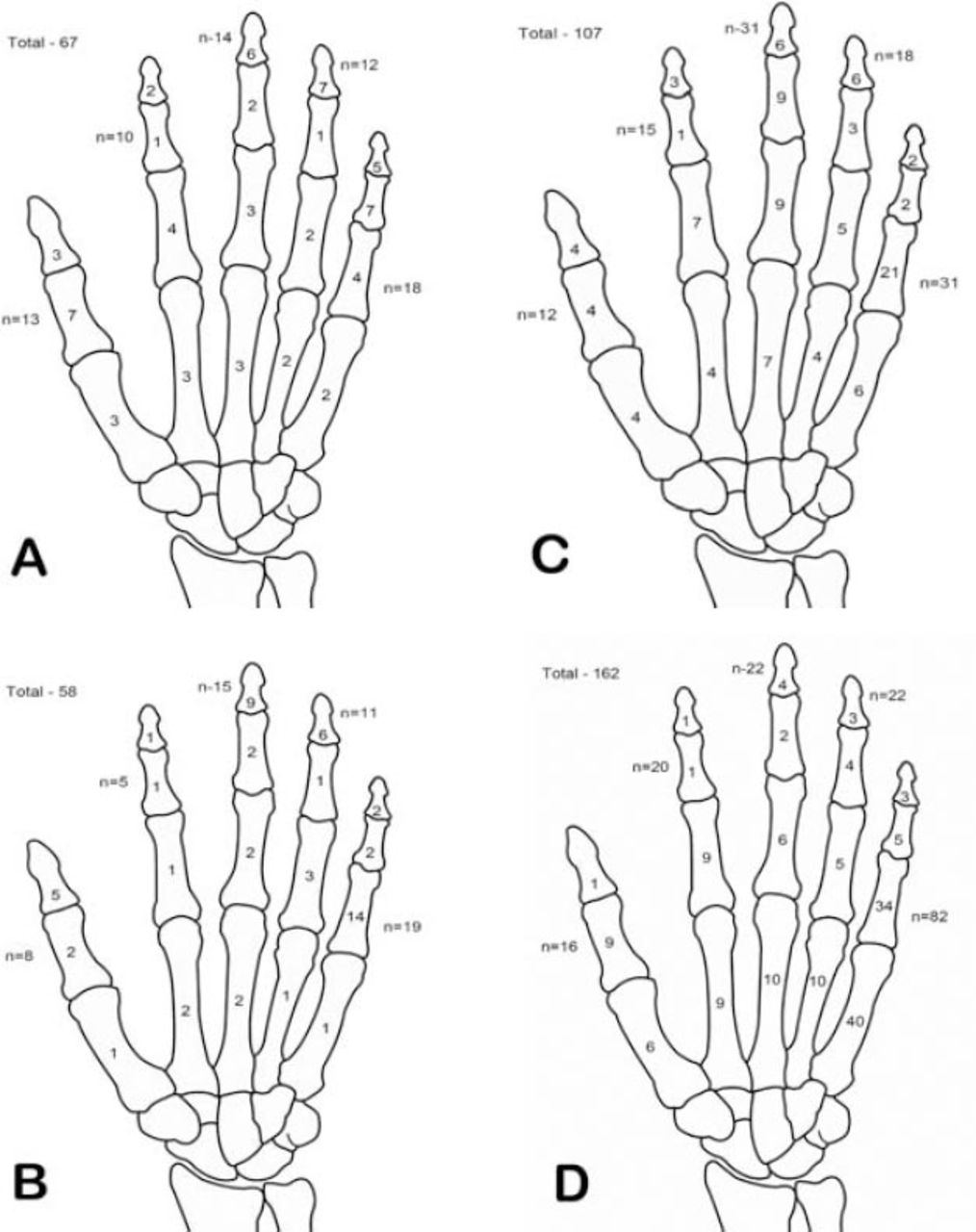
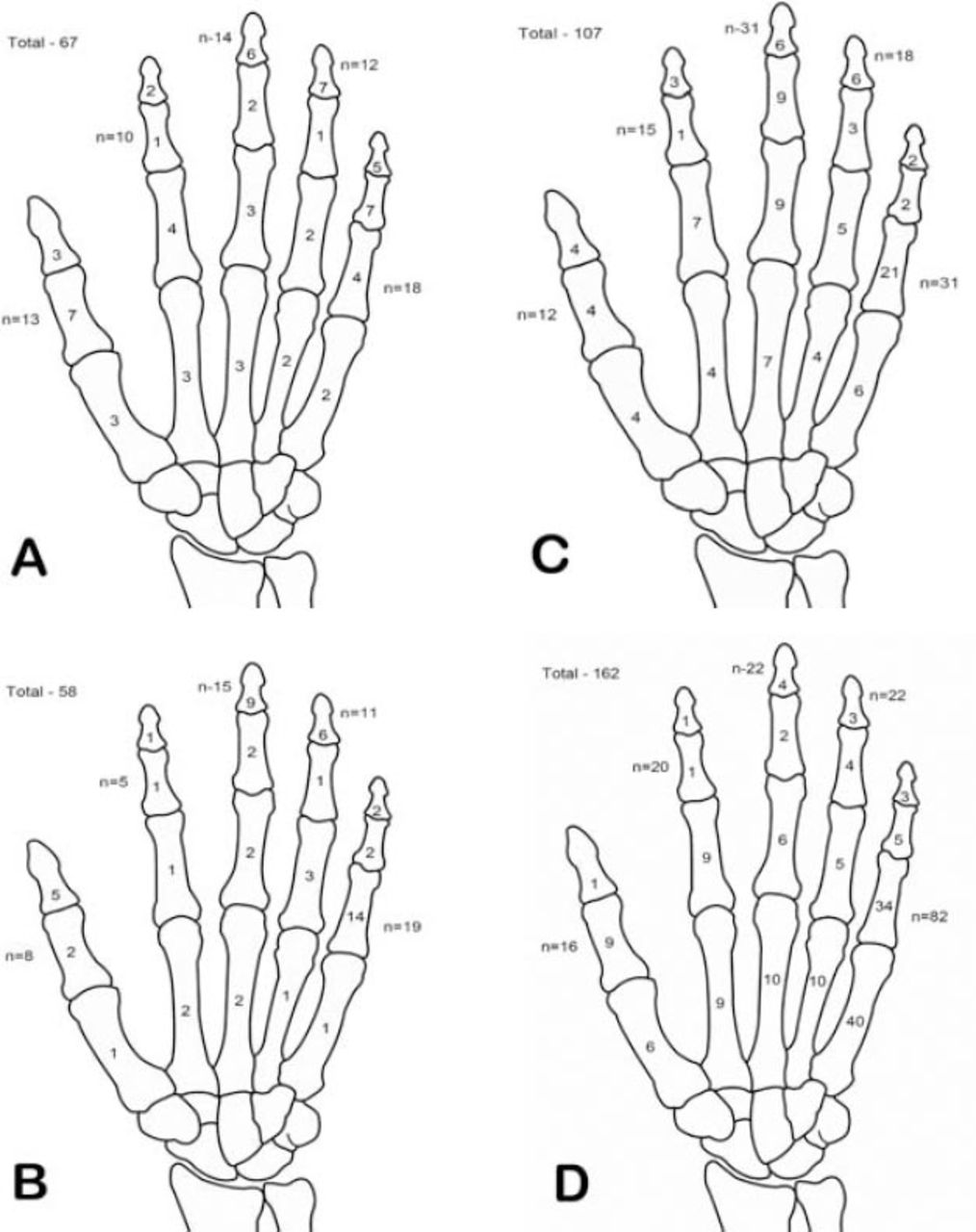
The distribution of hand fractures by bone and age group. The total number of cases is 361, and the total number of fractures was 398. In this figure the total number of fractures shown by age distribution is only 394 as the age was missing in 4 fractures. A) 1-4 years. The distal phalanx in this age group is the most commonly injured bone (n=24) and that the little finger is the most commonly fractured ray (n=18). B) 5-8 years. The distal phalanx (n=23) and proximal phalanx (n=22) are the 2 most commonly injured bones. The little finger (n=19) remains the most commonly injured ray. Within the little finger ray, the proximal phalanx makes 14 out of 19 fractures. C) 9-12 years. The proximal phalanx (n=46) is the most commonly injured bone. The little finger (n=31) and the middle finger (n=31) have equal distribution of fractures. The proximal phalanx of the little finger (n=21) remains the most commonly injured site. D) 13-18 years. The metacarpal (n=75) is the most commonly injured bone and the little finger (n=82) is the most commonly injured ray. Within the little finger ray, the metacarpal (n=40) is the most common site of fracture in this age group.
Discussion
Our study describes the epidemiology of hand fractures among children managed at KKUH during a 6-year period (2005-2011). Children are known for being active, which can lead to certain patterns of hand fractures. Most of these fractures could be managed in outpatient clinics, and few required surgical intervention. There was a preponderance of male patients (80.6%), which was consistent with other studies.3,14-17 This reflects that males are more active than females (especially outdoors) in addition to having more health risky behavior. This may be also due to the fact that most females tend to be at home, especially in Arab and Muslim cultures. A previous study,18 reported a male to female ratio of 3.2:1, and suggested that this higher ratio was due to males being involved in sports and other activities such as fighting. Our findings support this theory, although fighting was the cause in only one case in our series (Table 3).
In the present study, there was a peak age group for injuries (13-18 years) (Figure 1), which was also reported by other studies.15,17,18 This may be related to higher participation in sports in this age group, which was also evident by the higher proportion of fractures caused by sports related activities within this age group in our study. In our study, 19 out of 23 (82.6%) children aged 1-4 years old sustained their hand fractures at home, while the most sports-related fractures were in the 13-18 years age (Table 3). Furthermore, door slams at home were the main causes of fractures in the youngest 2 age groups (1-4 and 5-8 years). Falls at home were the main causes in the intermediate age group (9-12 years). Both falls at home and sports were important causes in the oldest age group (13-18 years). These findings have obvious implications in prevention. The right and left hand were similarly involved in our study, and this was also reported by other authors.16,18 In our study, the little finger was the most frequently fractured digit and the mostly frequently fractured bones were the proximal phalanx followed by the metacarpal. Several authors reported that distal phalanx fractures were most common in the 1-4 years and the 5-8 years age groups; little finger proximal phalanx fractures in the 9-12 years age group; and fifth metacarpal neck fractures, in the 13-18 years age group.15,16,18 In our study, the distribution of fractures within the little finger ray showed that the proximal phalanx was the most frequently fractured bone in the 5-8 years and the 9-12 years groups; and the metacarpal was the most frequently fractured bone in the 13-18 years group. The latter includes fifth metacarpal neck fractures reported by other authors to be the most frequent fracture of the hand in teenagers.15,16,18 Findings of the present study show that pediatric hand fractures in Saudi Arabia should be classified into 3 age groups (1-8 years, 9-12 years, and 13-18 years) to target fracture prevention. Safety of doors at home, prevention of falls at home, and safety measures in sports should be the targets to prevent hand fractures in these 3 age groups.
Study limitations
The retrospective nature of the study resulted in missing data. Another limitation is that we had no data regarding patient exposure to various risk factors to identify health risk behavior. Finally, we did not study methods of implementation of various safety measures in the prevention of fractures. This would require home visits and visits to sites of sport activities. We believe that these visits and studying the effect of prevention campaigns should guide future research on this topic in Saudi Arabia.
In conclusion, most hand fractures in children occurred at home, which requires reevaluation of the settings at home. This could be achieved by closely assessing most common reasons for falls at home, and making sure of the safety of doors to protect the children from injuring their hands. The conditions of sporting activities associated with hand fractures in the older age group need further study. Further, research is also needed to properly identify the best preventive measures and their effectiveness. Finally, it is important that clinicians in the emergency room have proper knowledge of hand fractures in children and their common sites according to the age group as this would greatly aid in proper diagnosis and management.
Acknowledgment
The research team would like to acknowledge the Deanship of Scientific Research, College of Medicine Research Center, King Saud University, Riyadh, Saudi Arabia for the support in conducting this study. We also would like to acknowledge the Medical Records Department, King Khalid University Hospital, Riyadh, Saudi Arabia for their cooperation during the study. We would like to thank all the interns for their help in data collection. We also would like to thank Mr. Virgilio Salvador for providing Figures 2 & 3.
Footnotes
Disclosure. This work was funded by the College of Medicine Research Center, Deanship of Scientific Research, King Saud University, Riyadh, Kingdom of Saudi Arabia. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 23, 2014.
- Accepted March 16, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}