


Abstract
Cystic lymphangioma usually confined to head and neck is a well-recognized tumor that occurs during childhood. However, a cardiac lymphangioma is exceptionally uncommon and a particularly rare form of disease. We report a case of cystic lymphangioma arising from the right ventricular wall, and presenting as pericardial mass in a young female, who presented with a history of exercise intolerance in the form of breathlessness on exertion and palpitations. The management of such a case was a difficult task; however, she underwent near total resection of the mass, and is doing well for the last 2 years.
Cardiac tumors are rare but potentially curable form of heart disease with incidence ranging from 0.0017-0.33% at autopsy. A high index of clinical suspicion is necessary for diagnosis as these tumors have protean manifestations that mimic a variety of other cardiac and noncardiac diseases.1,2 Most (>80%) of these tumors are benign, and myxoma is by far the most common. Myxoma constitutes approximately 50% of all benign cardiac tumors in adults, but only a small percentage of such tumors in children. Rhabdomyoma is the most common benign tumor in children, and accounts for 40-60% of cases. Other benign cardiac tumors include fibromas, lipomas, hemangiomas, papillary fibroelastomas, cystic tumors of the atrioventricular node, and paragangliomas. The remaining 20% of primary cardiac tumors are malignant, and are usually described as sarcomas.3 Cystic lymphangioma, usually confined to head and neck, is a well-recognized benign tumor that occurs during childhood. However, a cardiac lymphangioma is exceptionally uncommon and a particularly rare form of cardiac disease, and is considered to be a malformation that arises from sequestration of lymphatic tissue that fails to communicate normally with the rest of the lymphatic system.1,4,5 Cardiac lyphangiomas most frequently occur in the pericardial space, sometimes compressing adjacent structures; a chylous pericardial effusion may be present.6,7 The presentation in most cases is usually but not necessarily dramatic or acute, and the type of symptoms depends on the site and degree of involvement, ranging from syncope or palpitations to arrhythmia, or congestive heart failure.4,5 All imaging studies can provide information regarding the anatomic details of the mass, however to obtain final diagnosis and treatment, patient’s need surgical exploration and resection of the mass as was seen in our case.1,4,5 The objective in presenting this particular case is to highlight its atypical clinical picture and diagnostic uncertainty until surgical exploration.
Case Report
A 42-year-old married female was admitted in a tertiary care hospital with history of breathlessness on exertion of 2 months duration, which was associated with productive cough without any prior history suggestive of respiratory tract infection or viral prodrome. The patient also gave history of occasional palpitations of same durations, and did not have any significant past history. Her physical and systemic examination was normal. The investigative profile of the patient revealed: hemoglobin of 12.7, platelets, and erythrocyte sedimentation rate (ESR) with normal counts. Biochemical parameters like kidney and liver functions were normal. Echocardiography was normal but the x-ray chest parasternal axis view revealed cardiomegaly. Transthoracic echocardiography revealed a large pericardial mass measuring 10.6 x 4.8 cms (Figure 1 & 2), honeycombed in appearance, compressing the right atrium and right ventricle, and was associated with moderate pericardial effusion. The possibility of hydatid pericardial cyst was made, but hydatid serology was negative. Ultrasonography of abdomen was also normal. She was then extensively worked up with all forms of imaging including contrast enhanced CT (CECT) chest and cardiac MRI (Figure 3). Her CECT thorax revealed isodense non-enhancing lesion in pericardial cavity with pericardial fluid. The CECT possibility of organized exudative collection was made, and pericardial tumor like mesothelioma/teratoma was less likely in view of non-enhancing lesion. Cardiac MRI shows multicystic lesion in the right atrioventricular groove of heterogeneous hyperintense signal on T1 weighted images and bright signal on T2 weighted and gradient echo images with indistinct myocardial wall along the pericardial lesion. Lesion shows hypointense septae, and is compressing the right atrium and right ventricle. The MRI possibilities of pericardial lymphangioma, complex pericardial effusion, hemangioma/teratoma were made. The uncertainty of diagnosis was explained to the patient and her immediate family (husband and brother), and due to this uncertainty, no prognostication was performed. They understood the risk and consented for the operation. Finally she was subjected to surgery with surgical notes revealing the operative findings as pinkish brown mass covering the entire right ventricle on opening the pericardium. At no place did it feel hard and nodular, and was arising entirely from the right ventricular myocardium, and approximately 10 ml of clear straw colored fluid was aspirated from 2 cystic areas of the mass, and was sent for cytology and biochemistry. A categorical report of absence of malignancy from frozen section made the surgeons to excise as much as possible of the mass using the cardiopulmonary bypass support, and unfortunately, while excising the mass in the atrioventricular (AV) groove her right coronary artery (RCA) got excised with the tumor, which was given left saphenous vein graft. The whole operative and postoperative periods were otherwise uneventful. Screening echo revealed residual mass seen 4/2.8 cm at the junction of right atrium (RA)/right ventricle (RV)without pericardial effusion. Histopathology report of excised RV mass came as cystic lymphangioma (Figure 4 & 5).

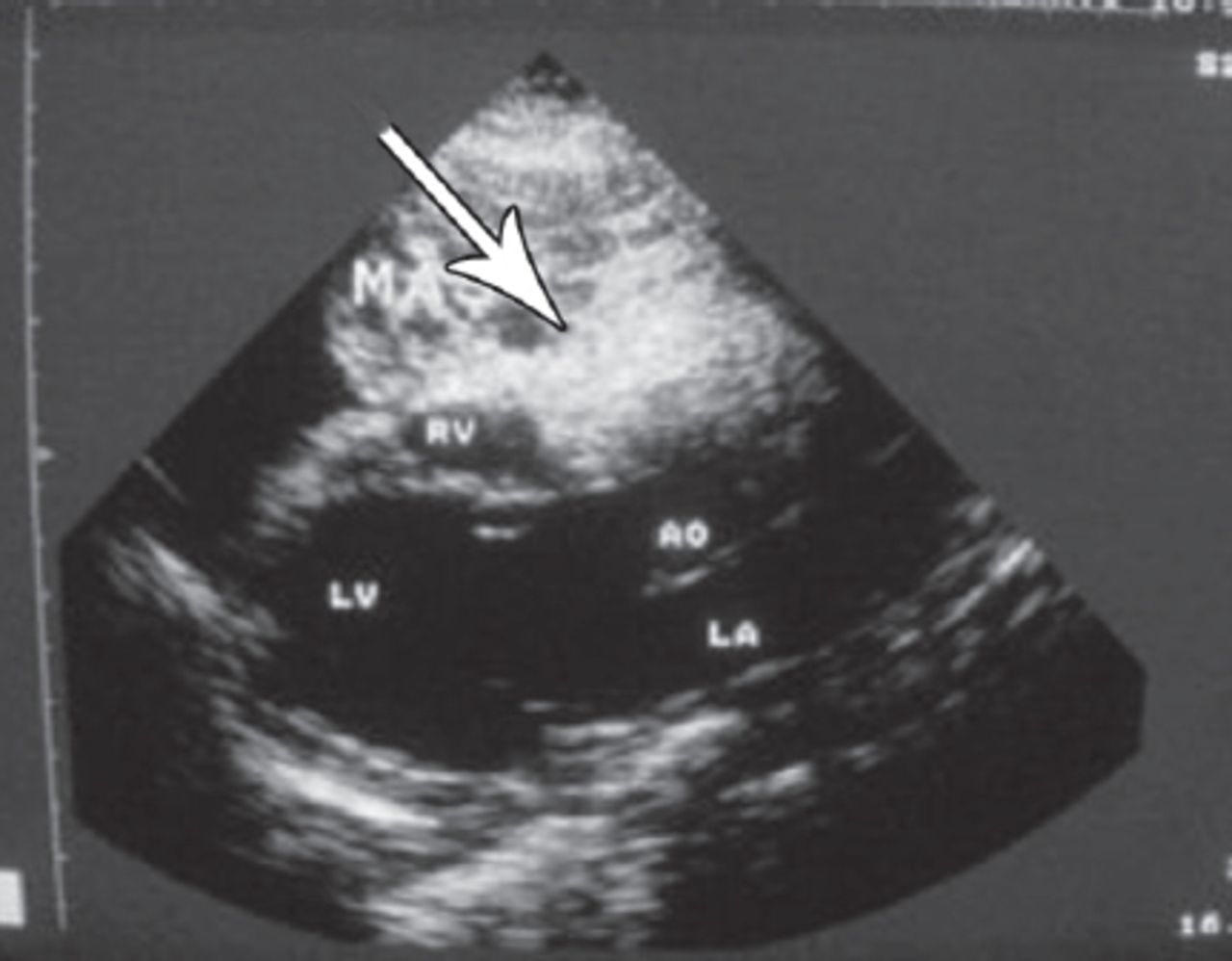
A 2D echo in parasternal long axis showing cystic mass in the pericardial cavity with compression of the right atrium and right ventricle.

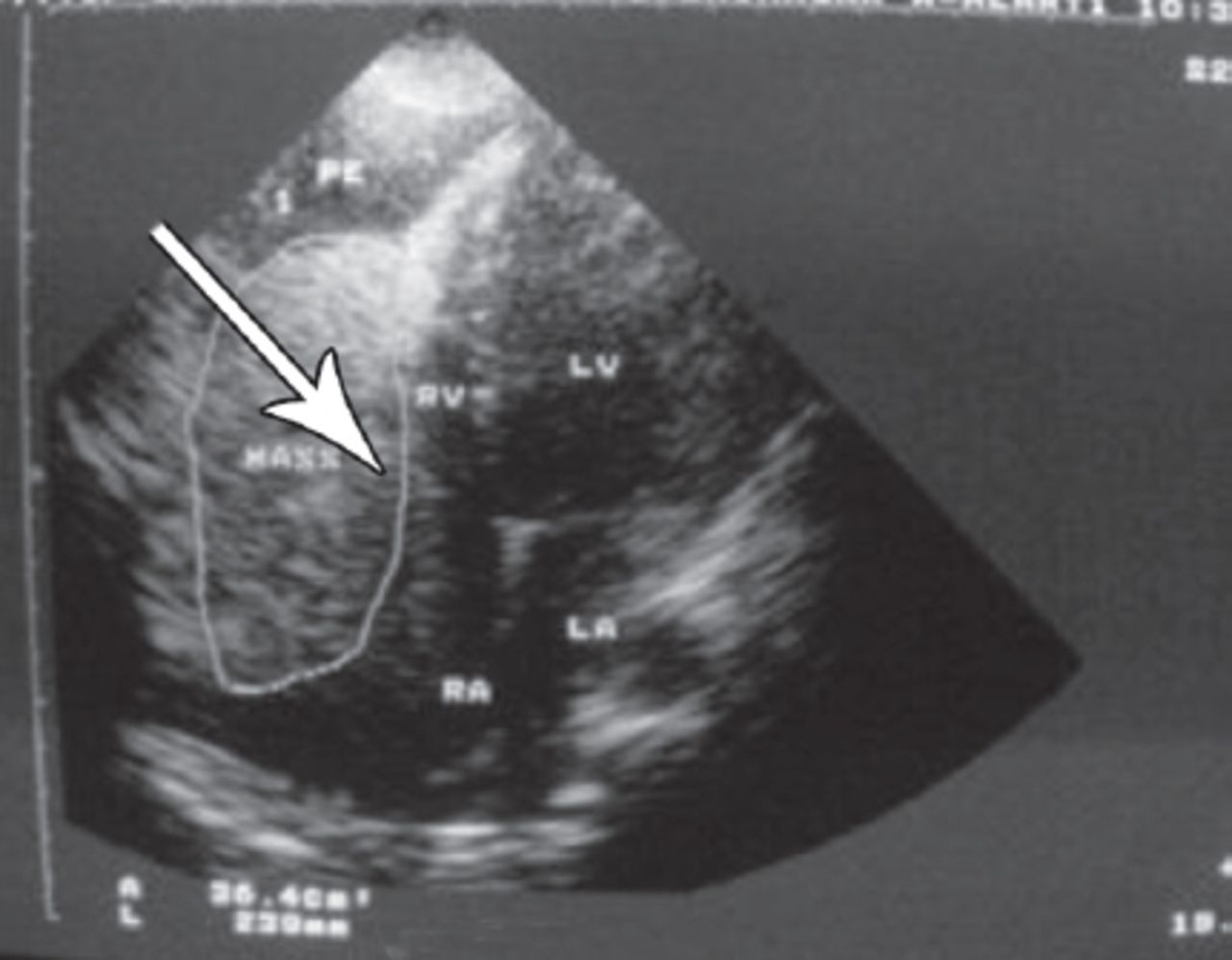
A chamber view showing the cystic mass in pericardial cavity with compression of the right atrium and right ventricle.

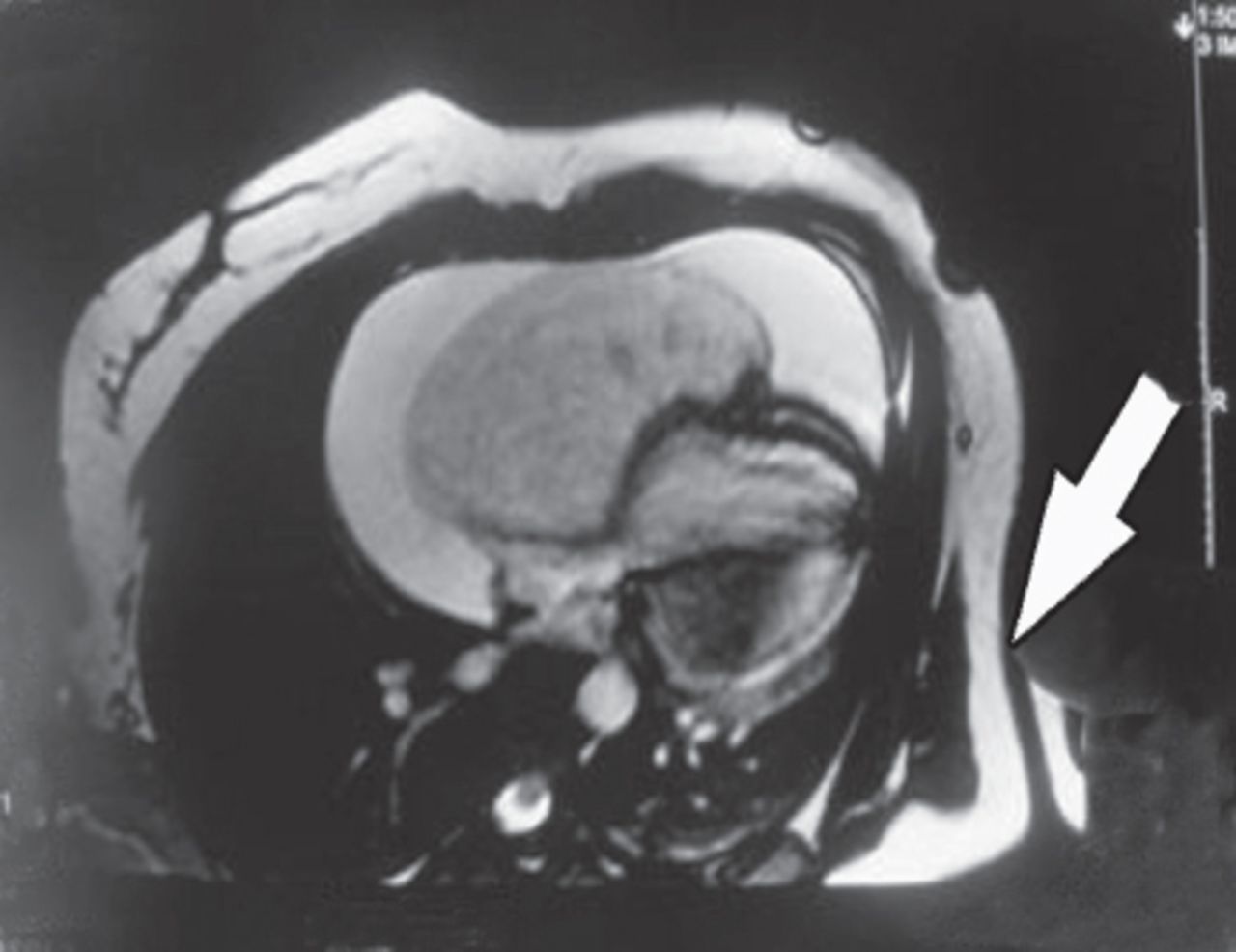
Cardiac MRI shows multi cystic lesions in right atrioventricular groove with compression of the right atrium and right ventricle.
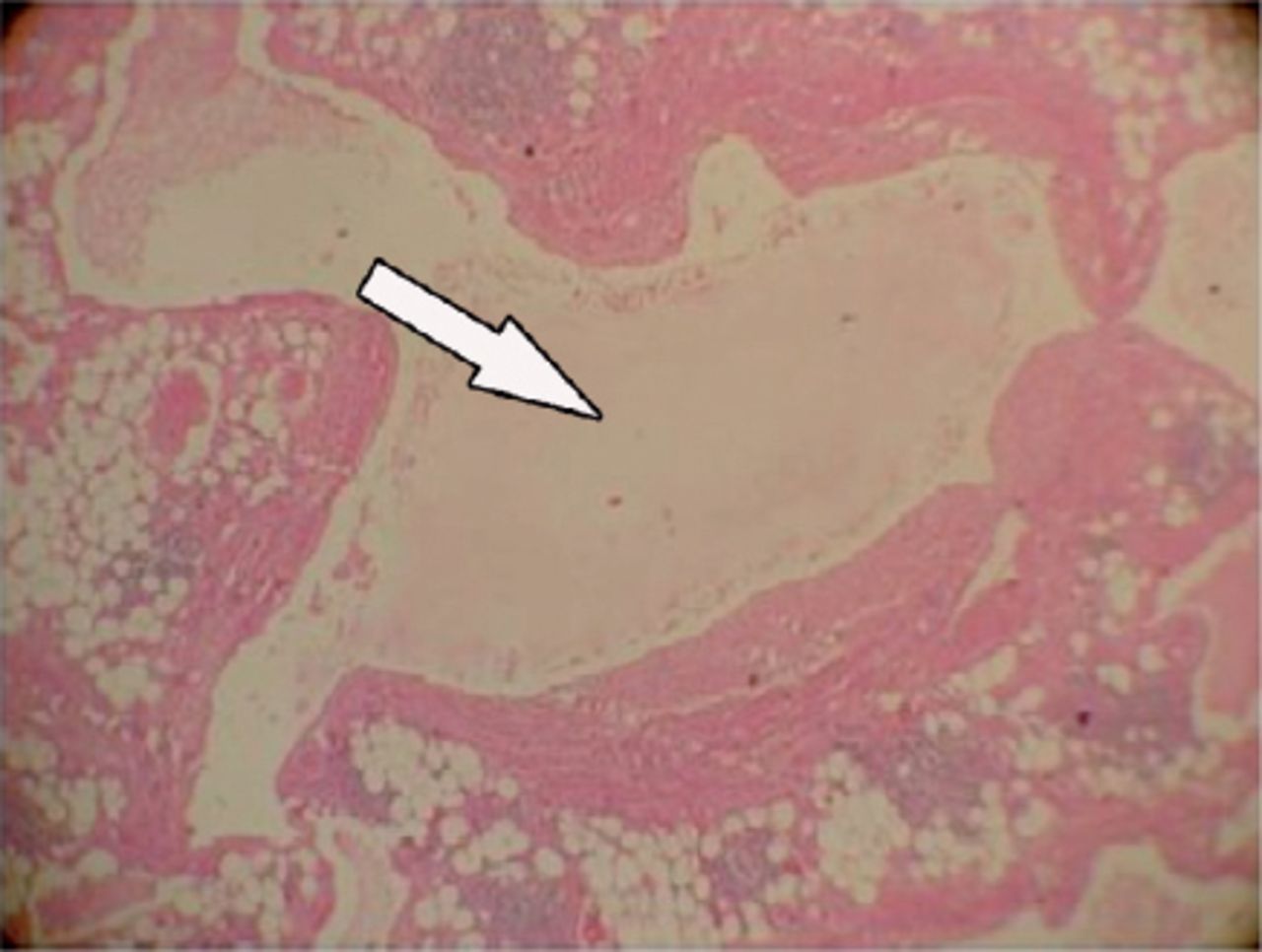
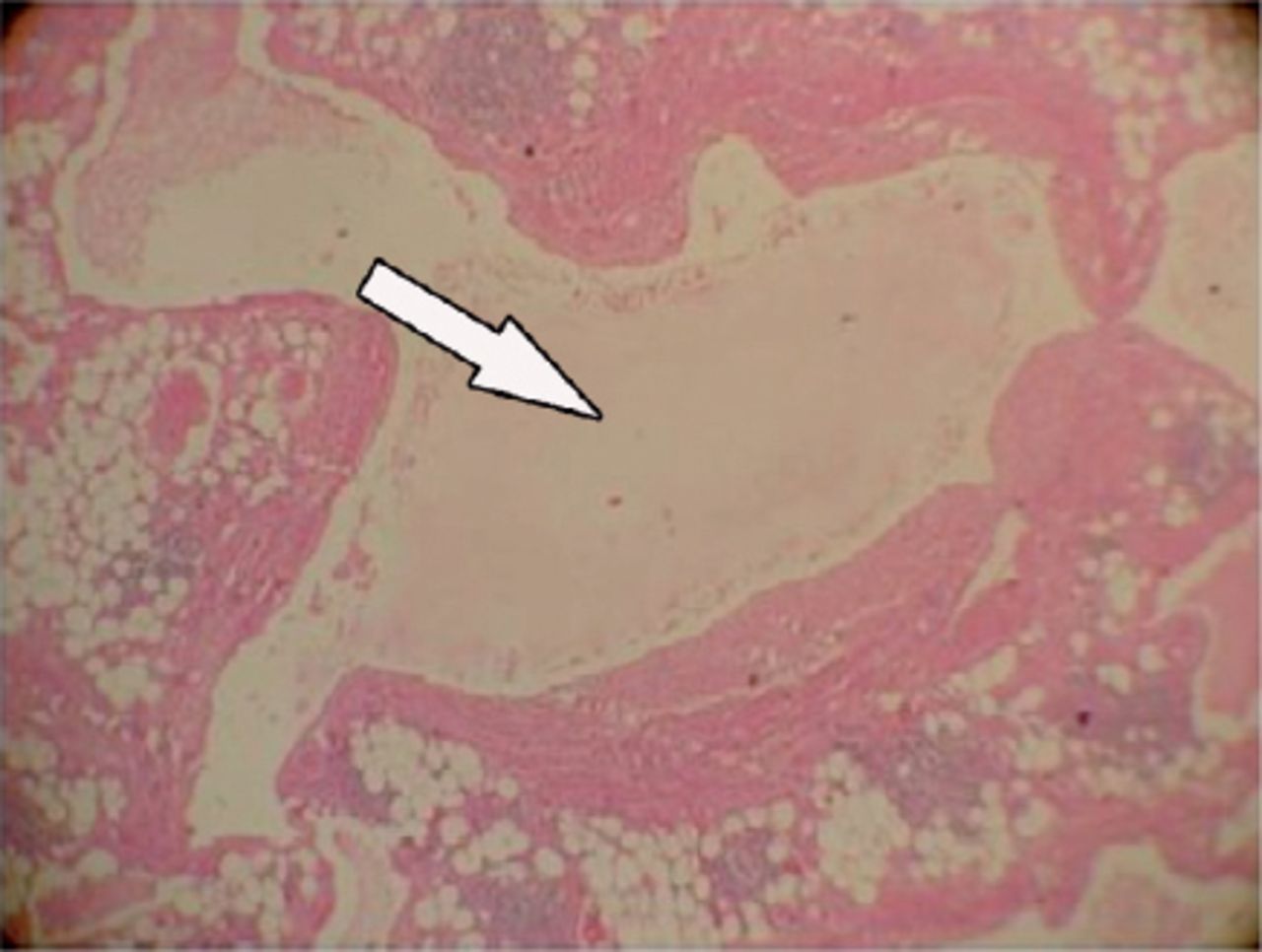
Cystic lymphatic space with surrounding adipose tissue and lymphoid follicles.(Hematoxylin & Eosin stain x100)

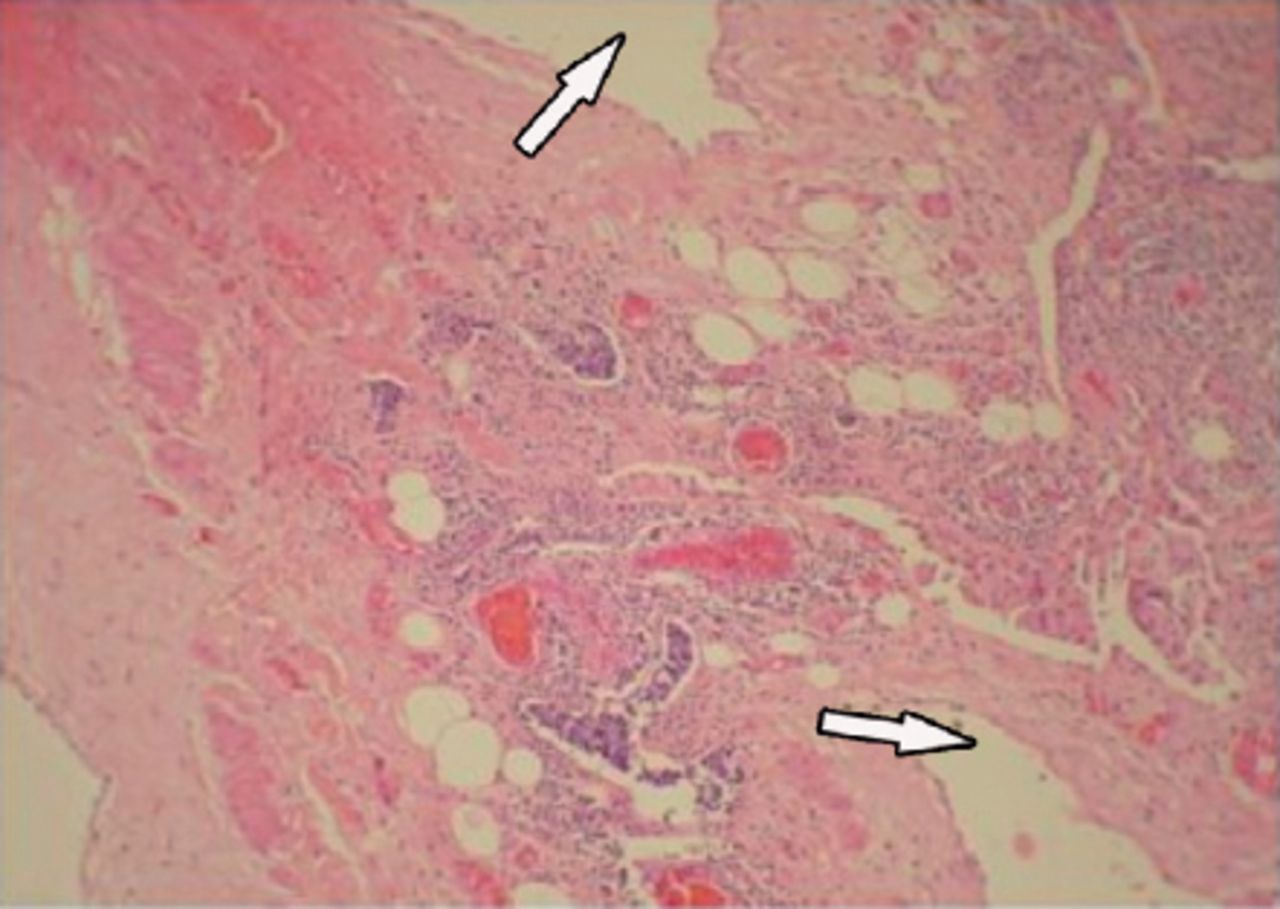
A Hematoxylin & Eosin stain x100 tiny lymphatic spaces filled with lymphocytes. Myocardial tissue is seen on the left. (Hematoxylin & Eosin stain x400)
Discussion
Cardiac lymphangioma is a rare benign vascular tumor of the heart, first reported in 1911 by Armstrong and Monckeberg.1,7 So far, only 9 cases have been reported in the medical literature.1,5 More than half of the reported cases have occurred in patients under 10 years of age. Cardiac lymphangiomas in these cases have been revealed during congestive heart failure, syncopal or embolic pathology, arrhythmias, palpitations, or cardiac tamponade.4,5 Our patient was not in heart failure nor had any features of tamponade, but had history of exertional breathlessness and palpitations without any history of syncopy or any embolic phenomena. These tumors most commonly occur in the pericardial space, but other unusual primary sites include the myocardium, the posterior wall of the left atrium, and AV node regions.4,5 In our case, the mass was arising from the RV wall and was projecting in the pericardial sac. Breast or lung cancers account for the greatest percentage of nonprimary cardiac tumors. Metastatic involvement is frequently located in the pericardium, resulting in pericardial effusion and epicardial involvement.1,3 Although, there was some pericardial effusion in our case, cystic mass was arising from RV and other sites were disease free. Cystic lymphangiomas have a potential risk of recurrence, especially if there has been am incomplete resection.5 Unfortunately, there has been an incomplete resection in our case, and following-up with the patient for 2 years, the mass has not increased in size, and patient is asymptomatic, but that does not mean that everything is fine. Patient needs to be observed for a longer period of time. Although the head, neck, and axilla are sites that account for one-half to three-fourths of all lymphangiomas, these masses may affect almost any part of the body, including the heart, like in our case. The real treatment is complete surgical resection.4
In conclusion, cardiac cystic lymphangioma, although rare benign cardiac tumor can have varied clinical picture, can also occur in adult age. Imaging studies available until today can only provide information regarding anatomic details, and the real treatment is total resection.
Acknowledgment
The authors gratefully acknowledge all who contributed to the work in presenting this case, to Mr. Younus Mohammad Dar for editing this report, especially to Dr. Nasser Ahmad Khan, Asst. Professor, Department of Radio Diagnosis, Government Medical College Srinagar, Karan Nagar, Srinagar, India.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received July 1, 2015.
- Accepted October 11, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.