


Abstract
Objectives: To evaluate the performance of GeneXpert MTB/RIF assay for direct diagnosis of pulmonary tuberculosis (PTB).
Methods: This is a cross-sectional study conducted between October 2013 and February 2016 at Abbassaia Chest Hospital and Ain Shams University Hospital, Cairo, Egypt. Inclusion criteria were adults between 18 and 60 years with suspected PTB and classified into 5 clinical categories based on their clinical, radiological, and laboratory findings: confirmed TB, probable TB, possible TB, unlikely TB, and not TB. Two sputum samples from each participant were analyzed by GX and the results were compared by conventional culture.
Results: In total, 218 participants were enrolled: 71 had confirmed TB; 112, highly probable TB; 20, probable TB; 10, unlikely TB; and 5, no TB. The sensitivity and specificity of the GX assay were 93% and 98.3% respectively. GeneXpert was positive in 93% of confirmed TB and 2.2% of probable TB cases.
Conclusions: GeneXpert is a rapid and promising technique with good sensitivity (93%) and specificity (98.3%), but it cannot be used as a standalone PTB diagnostic tool. There is a need for more GX evaluation studies in countries with low TB incidence.
Tuberculosis (TB) is a pandemic that causes serious morbidity and mortality. It is estimated that TB causes approximately 9.0 million cases annually, with approximately 1.5 million deaths.1 Egypt is classified by the World Health Organization (WHO) as a country with middle/low level of TB prevalence. Egypt’s population was 90 million in 2015, with an estimated TB burden of 11 cases per 100 000 population who had smear positive active pulmonary tuberculosis (PTB), and 24 per 100 000 who had all types of TB annually.2 Diagnosis of TB is still a challenging health care problem due to its nonspecific symptoms, or radiological signs.3 Although conventional culture is the gold standard for TB diagnosis, it is time-consuming and may extend anywhere between 2-8 weeks.4 Detection of acid-fast bacilli (AFB) by smear microscopy is a fast and cheap test for TB diagnosis, but it has low sensitivity and positive predictive value (PPV).5 Rapid diagnosis and detection of rifampicin (RIF) resistance is necessary for TB control, as transmission and emergence of multi-drug resistant tuberculosis (MDR-TB) cause serious health problems. GeneXpert MTB/RIF and GenoType MTBDRplus were approved by the WHO in 2011 and recommended for diagnosis of TB and MDR-TB in developing and high prevalence countries.6,7 GeneXpert MTB/RIF is a real time PCR (RT-PCR)-based molecular assay that amplifies a specific sequence of rpoB gene in Mycobacterium tuberculosis (MTB) and detects RIF resistance mutations as a marker for MDR-TB.8,9 The sensitivity of GX is closely related to the bacilli concentration in the specimen, and subsequently depends on sputum smear status.10 Some validation studies in adults described GX as a rapid, sensitive, and specific test for TB diagnosis and detection of RIF resistance.10,11 GeneXpert MTB/RIF could detect MTB in all smear-positive clinical samples and approximately 75% of smear-negative samples.8,10 Although there are many GX evaluation studies, the information is still limited in size and geographic representation.12 There are a few studies on GX evaluation in low-burden countries.13,14 The aim of this study was to evaluate GX for the rapid diagnosis of PTB and RIF resistance in sputum specimens from patients with suspected PTB compared with conventional culture methods as a gold standard in Egypt, a middle/low TB burden country.
Methods
This is a cross-sectional study conducted in at Abbassaia Chest Hospital and Ain Shams University Hospital, Cairo, Egypt. . The enrollment was between October 2013 and February 2016.
Patients enrolled in the present study were between 18 and 60 years of age with clinical signs of PTB. Excluded patients were those with symptoms of extra-pulmonary TB or any disease other than PTB (Table 1). Patients were classified into 5 groups depending on the results of their clinical, radiological, and laboratory investigations.15 Confirmed TB group included clinical investigations suggesting TB and acid fast smear or culture positive. Probable TB group included clinical investigations suggesting TB and radiological investigation consistent with TB and one of the following: a) good response with anti-TB therapy, b) documented exposure to MTB, c) positive results of TB immunological investigations. Possible TB group included clinical investigations suggesting TB and either one of the following: a) good response to anti-therapy, b) documented exposure to MTB, c) positive results of TB immunological investigations. Unlikely, the TB group included symptomatic patients, but did not agree with any previously mentioned definitions. Not TB group included diseases that were proven to be not TB.15 All enrolled patients in this study were HIV negative.
Comparison of acid fast smear and GeneXpert MTB/RIF tests.
Ethical approval
The study was approved by the local ethics committee of the Faculty of Women for Education, Arts and Sciences, Ain Shams University according to the principles of the Helsinki declaration. Written informed consent was obtained from all the enrolled patients.
Clinical procedure
Patients were diagnosed and treated by national TB program following the recommendations of the WHO. Anthropometric and clinical data were collected from patients’ files. Chest radiograph and tuberculin skin test (TST) were performed at recruitment visit.
Specimen collection and laboratory procedures
Two sputum specimens were collected from each participant. They were asked to expectorate sputum and in case expectoration was not possible, induced sputum (IS) specimen was obtained by a well-trained nurse as previously described by Zar et al.16 Sputum acid fast smear and culture on Lowenstein-Jensen (LJ) medium were performed within 2 hours at the hospital as routine procedures for TB diagnosis using standard techniques for mycobacterial laboratories.17Mycobacterium tuberculosis was confirmed by GenoType MTBDRplus assay (Hain LifeScience, Nehren, Germany) for both acid fast smear-positive and culture-positive samples following the manufacturer’s instructions. Conventional agar proportion on Middlebrook 7H11 was used for isoniazid (INH) and rifampicin RIF susceptibility testing, following the Clinical and Laboratory Standards Institute (CLSI) recommendations and recommended critical concentrations.18
Sputum samples were also analyzed by GX (Cepheid, USA) following the manufacturer’s instructions and aliquots were stored at 4ºC for duplicate testing within one week, if needed. All GX results were read and interpreted separately from that of the clinical, culture, and radiological results in a blinded fashion.
Statistical analysis
Receiver operating characteristic (ROC) curve was plotted from the data. Sensitivity, specificity, and positive and negative predictive values were calculated for TB diagnosis using GX, and 95% confidence interval (CI) was also determined.19 These were compared with the gold standard (conventional culture). The data were analyzed with MedCalc software (MedCalc, Mariakerke, Belgium).
Results
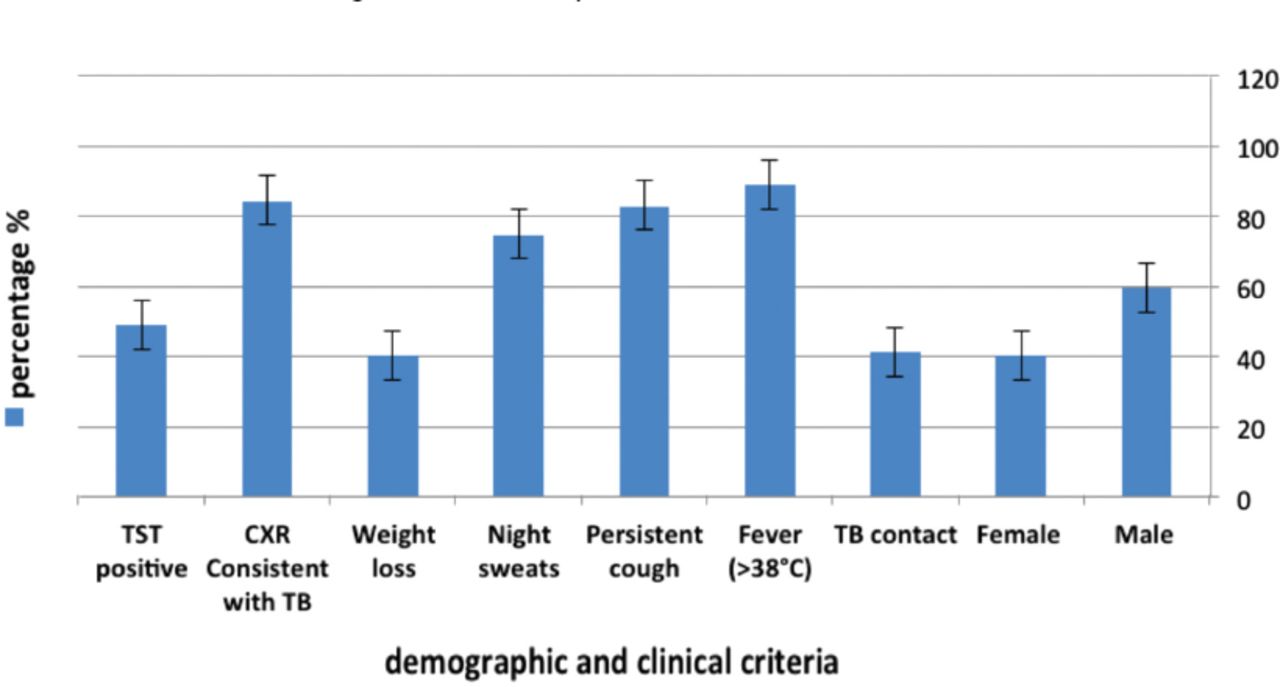
In this study, 230 patients were enrolled, of which 12 were excluded as they were diagnosed with extra-pulmonary tuberculosis. Of the 436 sputum samples collected, 4 samples showed invalid results by GX. Four hundred thirty-two (406 expectorated and 26 induced) sputum samples from 218 patients were eligible (Figure 1). The demographic and clinical characteristics of 218 selected patients are shown in Figure 2.

Patients enrolled in this study, collected specimens, and results of culture, acid fast smear, and GeneXpert (GX) Mycobacterium tuberculosis/resistance to rifampicin (MTB/RIF) tests. TB - tuberculosis

Demographic and clinical characteristics of 218 selected patients with clinical signs of pulmonary tuberculosis (TB). TST - tuberculin skin test, CXR - chest x ray
We analyzed 432 samples from 218 eligible patients using GX. Mycobacterium tuberculosis was detected in 132 samples from 67 patients belonging to confirmed TB group. GeneXpert showed negative results in 4 samples from 2 patients belonging to confirmed TB group. Five samples from 3 patients belonging to highly probable TB group were GX-positive and culture negative. The detailed GX results of patients in the various clinical categories are shown in Figure 1. The sensitivity, specificity, PPV, and NPV of GX and AFB compared to the gold standard are shown in Table 1. In this study, there was complete agreement between GX and culture method. Regarding the results of RIF susceptibility, no sample showed resistance to RIF.
Discussion
Diagnosis of TB is one of the most important steps for instituting control measures. Faster TB diagnosis means faster treatment and epidemiological control. GeneXpert is considered one of the recent promising tools for TB diagnosis. In this study, we aimed to evaluate GX for diagnosis of TB and susceptibility to RIF. Acid-fast bacilli is a cheap and rapid method that showed good sensitivity (86.4%) and excellent specificity (99.7%). These results are quite similar to those obtained by Bunsow et al20 where AFB showed sensitivity of 78.5% and specificity of 98.3% when compared with LJ culture as gold standard.20 Other studies21,22 reported low sensitivity and specificity for AFB. Previous studies of the GX assay have reported sensitivities of 57-76.9% in smear-negative, culture-positive respiratory specimens, and 98-100% in smear-positive, culture-positive respiratory specimens, while specificity remained at 99-100%.4,10,23 In this study, GX showed high sensitivity of 94.7% and 92.96%, and specificity 98% and 96.4%. Previous studies24,25 using GX reported quite similar results. A WHO meta-analysis indicated that suspected adult TB patients, when tested by GX against culture for samples of expectorated, or induced sputum, the pooled sensitivity was 66% and specificity was 98%.11 In our study, there was a complete agreement between GX and culture method as neither have detected any RIF resistant cases. Previous studies10,26 reported the sensitivity of GX for detecting RIF resistance to vary from 94.4-100% and specificity from 98.3-100%. The sensitivity of GX for detecting RIF resistance was 100% and the specificity was 96%.20
GeneXpert identified additional 3 TB patients without culture positive results in possible TB patients. It could not detect 4 cases of TB confirmed patients. It could not differentiate between active, or dead bacilli. GeneXpert detected only few patients among clinically diagnosed TB patients, which is similar to findings from previous studies.9,27 Due to these limitations, GX cannot be used alone in PTB diagnosis; clinical and chest radiographs are still important for PTB diagnosis.
Study limitations
This study was aimed at evaluating the performance of GX for diagnosis of PTB directly by detection of MTB in sputum samples. In this study, there were 84% confirmed and probable TB cases. This was due to selection bias and did not reflect disease prevalence. In this study, sensitivity calculations take into account only patients with confirmed TB. The results of sputum GX were closely related to those of sputum AFB smear and they implied that high positive rate would enhance GX sensitivity. Importantly, no samples showed resistance to RIF either by GX or culture method. However, we could not evaluate the accuracy of GX in the detection of RIF resistance.
In conclusion, our findings suggest that GX is powerful tool for PTB diagnosis with good sensitivity (93%) and specificity (98.3%). We recommend using it in routine TB diagnosis as this will expedite management of patients with presumptive TB. However, it should not be used alone, as clinical and radiological assessment are still important components of the diagnosis pathway. There is a need for more studies for evaluation of GX in countries with middle and low TB incidence such as Egypt.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 5, 2016.
- Accepted June 22, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.