


Abstract
Objectives: To assess the safety and effectiveness of transthoracic echocardiography (TTE) in monitoring transcatheter closure of atrial septal defect (ASD), in comparison with conventional technique using transesophageal echocardiography (TEE).
Methods: A retrospective review of all cases of transcatheter closure of isolated ostium secundum ASDs operated from 2005 to 2015, at the Pediatric Interventional Cardiology Department, King Abdulaziz University Hospital, Jeddah, Kingdom of Saudi Arabia. Exclusion criteria included age ≤3 years at the time of the procedure and rim size ≤3 mm. Patients were divided into 2 groups: TTE and TEE group. Demographic and clinical baseline data, procedure data, and outcomes were compared between the 2 groups.
Results: We included 77 cases: 45 in TTE group and 28 in TEE (mean ± standard deviation age=8.18 ± 5.85 versus 17.68 ± 14.88), with no significant difference in ASD size, rim adequacy, or other anatomical difficulties. All (100%) patients in TEE group underwent general anesthesia, versus 8.9% in TTE group. Device deployment was comparably successful (97.8% versus 92.9%, p=0.554); while procedure time (76.27 ± 31.80 versus 119.85 ± 19.90 minutes, p<0.001) and fluoroscopy time (11.29 ± 9.04 versus 18.73 ± 11.54 minutes, p=0.003) were significantly reduced in TTE versus TEE. Prevalence of postprocedural complications was comparable in the 2 groups.
Conclusion: Transthoracic echocardiography has non-inferior efficacy in device deployment with reference to TEE and superior safety features including significant reduction of procedure and fluoroscopy times and lesser use of general anesthesia.
Echocardiography is a precious tool in interventional cardiology including in percutaneous closure of atrial septal defects (ASDs), as it enables real-time guidance of the device and intraprocedural functional and structural evaluations.1 Atrial septal defect is a common congenital heart disease (CHD) that represents nearly 13% of all CHDs, as reported in different countries including Saudi Arabia.2,3 There are different types of ASDs, classified according to their site relative to the fossa ovalis; and the most common types are the ostium secundum defects, accounting for approximately 7% of CHDs.4 Structural features of ASDs including defect number, size, and location, rim size, shunt volume, and associated anatomical lesions are characterized by great individual fluctuations.5 The success of the procedure judged upon complete closure of the shunt and relies critically on accurate estimation of all these parameters in order to choose the adequate size of the closure device, follow-up its deployment and further complications. Conventionally, trans-esophageal echocardiography (TEE) is the imaging technique of choice in intraprocedural assistance of cardiac catheterization due to its higher resolution images.6 On the other hand, there are no practical guidelines in literature regarding feasibility or appropriateness of transthoracic echocardiography (TTE) to guide transcatheter occlusion of ASD;7 although several authors support that TTE constitutes a less invasive and more cost-effective alternative that can be performed in considerable number of patients with uncomplicated lesions and adequate anatomical features; in addition to its non-negligible advantage over TEE in that it avoids general anesthesia for the patient.8-11 This study aimed to evaluate the safety and effectiveness of using TTE imaging in comparison with the conventional technique using TEE, in intraprocedural monitoring of percutaneous transcatheter closure of ostium secundum ASDs. The other objectives were to investigate risk factors of procedural failure; and to compare outcomes between different operators, in an attempt to assess whether an operator-factor may presumably impact failure or success.
Methods
Design
This was a retrospective chart review of all cases of transcatheter closure of ASD who were operated from 2005 to 2015 at the Pediatric Interventional Cardiology Unit in King Abdulaziz University Hospital (KAUH), Jeddah, Kingdom of Saudi Arabia to 2010. transesophageal echocardiography was the exclusive technique used in percutaneous ASD closure in our department; but since 2010, the TTE was progressively used for both assessment of the ASD size and guidance of the occlude transcatheter deployment. The study was approved by the unit of biomedical ethics of KAUH.
Study population
Indications for ASD closure included echocardiographic and clinical evidence of ASD with left-to-right shunt or right ventricular overload,12,13 with the exclusion of cases with severe pulmonary arterial hypertension. Only patients who underwent ostium secundum ASD closure were included in the study. Exclusion criteria included age ≤3 years old at the time of the procedure; other associated CHDs; and rim size ≤3 mm from the mitral and tricuspid valves. According to the echocardiography technique used, patients were divided into 2 groups: TTE group and TEE group. Demographic and clinical baseline data, procedure data and early and late outcomes data were anonymously collected for comparison between the 2 groups.
Procedures
Interventions were performed in aseptic conditions, by one of 2 certified and qualified interventional pediatric cardiologists in our department. Both TTE and TEE images were acquired using Vivid E9 echocardiography machines (General electric, NY, USA). Moderate sedation or general anesthesia was performed according to the case followed by the administration of heparin with consequent monitoring of activated coagulation time.14 In TTE group, size and location of the defect, as well as the superior and inferior rim sizes were reevaluated before catheterization on 3 standard echocardiography views: parasternal short axis, apical 4 chamber, and subcostal sagittal. Sedation used single or repeated doses of ketamine IV 0.25- 0.5 mg/kg, midazolam 1-2 mg IV, or fentanyl IV 25-50 mcg.15-17 In both groups, selection of device size was decided upon intraprocedural measurement of ASD size, using color flow technique:18 an ASD closure device, Amplatzer double disc septal occluder (St. Jude Medical, St. Paul, MN, USA), with a waist diameter of at least 2 mm larger than the ASD diameter was used. On sedated patient, the right femoral vein was punctured and an appropriate sheath was introduced after hemodynamic study was carried out An appropriate long sheath is positioned over a wire until reaching the proximal portion of the left upper pulmonary vein. The closure device was loaded into the delivery cable and introduced through the long sheath, guided by fluoroscopy and echocardiography (TTE or TEE) until reaching the tip of the long sheath. The device was then pulled with the sheath into the left heart cavity, where the left disc of the device was opened. The sheath and device were then gently pulled as one unit until the left disc lied against the atrial septum. The sheath was pulled further until the right device disc was opened in the right atrium, embracing the atrial septum. The correct position of the device was assured by fluoroscopy and echocardiography, after which the device was released. Successful deployment of the device was judged upon stable implantation of the device without embolization or malposition.19 Residual shunt was assessed by color Doppler both in TTE and TEE cases. A final assessment of the position of the device was performed by echocardiography (TTE or TEE, according to the group) and fluoroscopy before removal of the femoral catheters and sheath.
Clinical baseline data
Rim size was defined adequate as ≥5 mm or and inadequate as ≥3 mm of margin from the mitral and tricuspid valves and right upper pulmonary vein as measured by echocardiography. Associated anatomical abnormalities interfering with the deployment of the device, or good echo-visibility, such as deformities, calcifications, or surgical scares in the chest structures were classified on operator’s evaluation into 3 levels of difficulty: none, mild, or significant anatomical difficulty. Heart cavities including right ventricle volume were collected for all participants in baseline, early and late outcomes.
Procedure data
Procedure time was defined as the time from skin puncture to achievement of hemostasis at procedure end.14 Other procedural data included fluoroscopy time and sedation technique.
Outcomes
Deployment (success/failure) was analyzed as the primary outcome; while residual shunt was analyzed as a secondary outcome. Other significant events occurring before patient’s discharge were collected and analyzed as early postprocedural complications. These included device migration (or embolization), arrhythmia, erosion, and thromboembolic complications.20 Embolization was defined as the movement of the device outside of the ASD after its release from the delivery system; arrhythmia as the development of a transient or permanent tachyarrhythmia or heart block during or after the procedure; while erosion was defined as an atrial tissue abrasion consecutive to the procedure.13,20 Further cardiovascular adverse events, such as heart block, femoral bleeding, and transfer to surgery were analyzed in both early and late postprocedural assessments.19
Statistical Methods
Statistical analysis was carried out using the Statistical Package for Social Sciences version 16 for Windows (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to calculate frequencies and percentages on categorical variables; and means and standard deviations (SD) on continuous variables. Comparison of means between the 2 groups TTE versus TEE was performed using independent t-test; while comparison of the proportions was performed using the Chi-square test. Statistical significance was assumed for a p<0.005.
Results
Demographic and clinical characteristics
In (Table 1), a total of 77 cases of ASD closure were included, of which 45 were guided by TTE and 28 by TEE. Patients from the TTE group were younger than those from the TEE group: mean ± SD, [range] age = 8.2 ± 5.9, [3-27 years] in TTE versus 17.7 ± 14.9, [3-45 years] in TEE, (p=0.003). Gender distribution showed no statistically significant difference between the 2 groups (p=0.684). Other baseline characteristics showed no significant difference in body mass index (BMI), although there were significant disparity in weights and heights in relation with the significant age discrepancy. Clinical baseline data including mean ± SD ASD size (p=0.165), frequency of preoperative right ventricle dilatation (p=0.635), rim adequacy (p=1.000), and other anatomical difficulties (p=0.405) were comparable between the 2 groups.
Demographic and clinical baseline data in TTE and TEE groups.
Procedure characteristics
In (Table 2), in the TTE group, most of the procedures (91.1%) were performed under sedation; while in TEE group, all (100%) were performed under general anesthesia, (p<0.001). With respect to device deployment, success rate was comparably high in both groups (97.8% in TTE group versus 92.9% in TEE group) without statistically significant difference. Procedure time (mean ± SD = 76.3 ± 31.8 versus 119.9 ± 19.9, p<0.001) and fluoroscopy time (11.3 ± 9.0 versus 18.7 ± 11.5, p=0.003) were significantly reduced with TTE as compared with TEE.
Comparison of procedure data and deployment success rate between TTE and TEE groups
Early and late complications
Analysis of the early (≤24 hours) and late (>1 day) postprocedural outcomes showed comparable results between the TTE and the TEE groups regarding the prevalence of residual flow, device complications (migration or embolization), arrhythmia, and right ventricle dilatation. However, subjects from the TEE group were followed up for a longer period as compared with the TTE group (p=0.029), which is related to the relatively recent use of TTE in ASD closure procedures in our department. Comparisons of early and late outcomes between the 2 study groups are depicted in Table 3.
Comparison of early and late complications between the TTE and TEE groups.
Inter-operator performance comparison
Procedure data and early postprocedural outcomes were compared between the 2 operators, to assess whether the interventional performances in ASD closure using TTE may significantly change from an operator to the other. Analysis showed no significant difference between the 2 operators regarding the sedation method used (p=0.285), deployment success rate (p=0.33), device complications, and procedure time (p=0.50); however, only fluoroscopy time was significantly longer in one operator as compared with the other (p=0.004) as shown in Table 4.
Comparison of procedure data and short-term outcomes between the 2 operators in the transthoracic echocardiography group (n=45).
Correlation of device-to-defect ratio
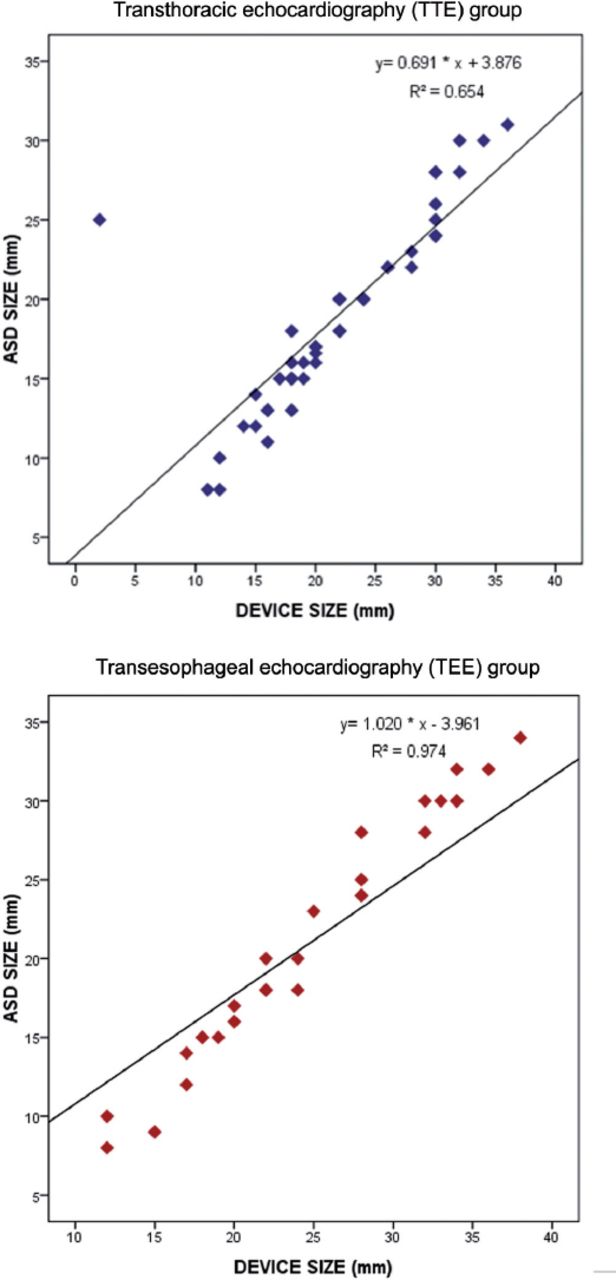
In Figure 1, we analyzed the correlation between the device size and defect size in both groups using Pearson’s correlation. Results showed better correlation between defect size and device size in the TEE group (R2=0.974, p<0.001) than in the TTE group (R2=0.691, p<0.001).

Pearson’s correlation of device-to-defect size in TTE and TEE groups correlation between defect size and device size in transthoracic echocardiography (upper panel, R2= 0.691, p<0.001) and transesophageal echocardiography (lower panel; R2=0.974, p<0.001). ASD- atrial septal defects
Discussion
This retrospective study gives evidence of the appropriate use of TTE to guide transcatheter closure of ASD in a majority of patients. Analysis of safety parameters demonstrated that there is advantage in using TTE, in that it reduced the resort to general anesthesia and shortened procedure and fluoroscopy times, without increasing the incidence of periprocedural or late complications, in comparison with TEE. In addition, efficacy parameter represented by the 97.8% deployment success rate suggests that TTE could be the technique of reference in monitoring percutaneous ASD closure. Review of literature provides generally comparable data. A prospective study by Bartakian et al14 compared outcomes of percutaneous ASD closure in patients randomly assigned to either the TTE or TEE group. Authors reported 100% of success in both groups with comparable postprocedural complication rates. Similarly, in a retrospective study, Ding et al11 reported 100% of success in both TTE and TEE groups, including 82 adults. A study by Li et al10 assessed safety and efficacy of TTE in monitoring ASD transcatheter closure in correlation with the ASD diameter. Authors reported 98.4% of successful deployment in all patients, regardless of their ASD diameter, which ranged between 5 and 38 mm. Another study by Behjati et al21 showed 90.5% of successful deployment in ASD closure in a cohort of 63 children and adolescents; all underwent the procedure using TTE. Conversely, other authors reported less enthusiastic results; such as Kardon et al,22 who reported only 75.7% of success rate in a series of 74 patients; and the failed cases were either proceeded with TEE or referred to surgery. These discrepant results are probably explained by differences in respective population characteristics and selection criteria. For example, in our study we included only patients with isolated ASD, as with Bartakian et al14 who also excluded cases with inadequate TTE windows; while Ding et al. carried out his study on adult patients.
Regarding procedure data, we demonstrated that both procedure and fluoroscopy times were significantly reduced in the TTE group (76.3 ± 31.8 versus 119.9 ± 19.9 minutes [min]) in comparison with TEE group (11.3 ± 9.0 versus 18.7 ± 11.5 min). Concordant findings were reported by Bartakian et al14 showing shortened procedure (51 ± 17.6 versus 70.6 ± 23.0 min) and fluoroscopy (13.6 ± 6.2 min versus 8.9 ± 8.5 min) times in TTE versus TEE groups. In their cohort, Behjati et al21 similarly reported shorter procedure (47.8 ± 11.2 min) and a fluoroscopy (9.4 ± 4.5 min) times. Aytemir et al,23 who compared TEE-guided ASD closure with TTE-guided patent formen ovale (PFO) closure also concluded to even shorter procedural (12.4 ± 3.2 versus 22.3 ± 4.7 min) and fluoroscopy (3.1 ± 1.2 versus 4.1 ± 1.9 min) times in PFO-TTE group versus ASD-TEE group. On the other hand, Pearson correlation showed better device-to-defect ratio in TEE group (R2=0.974, p<0.001) than in the TTE group (R2=0.691, p<0.001); which reflects better accuracy in case of TEE. Although these results did not affect the outcomes, either at early or late assessments, they are in contradiction with the results reported by Bartakian et al,14 who found that scaled diameter in TTE was more accurate for sizing the device than stop flow technique in TEE. Additionally, we demonstrated that TTE is associated with fewer resort to general anesthesia. This constitutes a major advantage over TEE that contributes to the reduction in procedure time, as well. In their randomized study, Bartakian used general anesthesia for all patients, in both TTE and TEE groups;14 while Behjati et al.21 used both moderate sedation or general anesthesia in their cohort of TTE-guided ASD closure. Further, we demonstrated that the benefits of TTE in term of safety and efficacy are maintained from an operator to another. Although fluoroscopy time was significantly longer in one operator, this did not affect procedure time that was comparable between the 2 operators. Also, other major parameters including success rate and complications were comparable between the 2 operators. We could not investigate further operator-related factors, being limited by the retrospective data collection. Still, the comparison we presented indicates that there is no strong operator-factor impacting TTE outcome in term of safety and effectiveness. Another notable outcome of the procedure was the improvement of the right ventricle functions in a consequent number of patients. This was indicated by a decrease in the prevalence of right ventricle dilatation from early to late assessments, which was equally observed in the TTE group (from 91.1 to 4.4%) and TEE group (from 92.9 to 7.1%). These observations are concordant with what was reported by Ding et al,11 who observed no significant difference between the TTE and TEE groups at 3, 6, and 12 months postprocedural assessments of heart cavities dimensions, evidencing a gradual decrease in right ventricular dimension concomitant to increase in left ventricular end-diastolic dimension.
In early and late follow-up, residual shunts were detected 15.9% in the TTE and 11.1% in the TTE group, and 29.6% in the TTE and 25.0% in the TEE group. Residual shunts can be of varying degree and are commonly the consequence of a mismatch between, the device shape and the defect anatomy.5 Regarding other early postprocedural complications, device migration occurred in 3 patients from the TTE group and only one patient from the TEE group; arrhythmia occurred in 3 patients from TTE group and 4 from the TEE group; while the only case of embolisation belonged to the TTE group. Similarly, no notable differences were observed between the 2 techniques in late assessments. These showed comparable prevalence of residual shunts and device migration; with the exception of one patient from the TTE group who had the closure device dislodgement into the right ventricle. In concordance with our findings, Behjati et al21 reported 21% of cases of arrhythmia and only one case of device dislodgement and one other case of device embolization; Chen et al24 reported 12.8%; Bartakian14 observed one case of arrhythmia in the TTE group and 2 in the TEE group, but no major complication in either group; while Aytemir23 reported 2 (0.5%) cases of periprocedural device embolization and 4 (1.8%) cases of recurrent embolic events during follow-up. Arrhythmia is considered as a minor but prevalent complication of ASD device closure; it accounts for 5% of the medical device reported events. It is more frequently represented by a transient or permanent tachyarrhythmia; and less frequently by a bundle branch block, which is reported in only 0.3% of the patients.20 Device embolization is classified as a major complication and requires surgical retrieval in most cases. It is principally favored by an undersized device or an inadequate rim, besides operator-related technical issues. Safety reports present it as a rare (approximately 0.6% of prevalence) but potential complication of every attempted ASD closure; although the Manufacturer and User Facility Device Experience (MAUDE) database statistics showed it as the most frequent major adverse event.20 These data are supported by a meta-analysis by Abaci et al,6 who reported up to 9.4% of major periprocedural complications in percutaneous ASD closure, with device embolization being the most frequent complication. Other potential or rarely reported major complications in transcutaneous ASD closure include infections, thromboembolic events, erosion, cardiac perforation, postoperative cardiac arrest, and allergies.20,24
We reported a single case of referral to surgery for removal of the device that migrated to right ventricle; however, this case belonged to the TEE group. There are different motivations for surgical referrals reported in literature. Kardon et al,22 reported 16.2% out of 74 patients who were referred to surgery for surgical closure of ASD after TTE evaluation; while Behjati et al,21 and Chen et al,24 resorted to surgery for retrieval of embolized and dislocated devices. Surgical repair used to be the management of choice in ASD closure. It was first attempted in late 1930’s; and consecutively, several surgical techniques have been developed.20 However, surgery carries a relatively high risk of complications and necessitates the use of cardiopulmonary bypass; which increases the odds of postoperative complications including pulmonary complications.25,26 Consequently, minimally invasive percutaneous transcatheterization with the aid of fluoroscopic imaging and echocardiography has become the preferred method for ASD closure.27,28 In addition, it was demonstrated that percutaneous procedures are more cost-effective and allow reducing the physical and psychological distress to the patients, as well as the operative time and hospital stay.29,30 On the other hand, surgical techniques still have an advantage over percutaneous transcatheterization, in that they allow closure of larger ASDs regardless of the types and rims.20
In a practical sense, it is becoming crucial to establish standard criteria and guidelines for the choice of the ASD closure technique, on basis of preprocedural evaluations of each patient’s morphological and clinical features. Based on the previously presented literature data supported by our findings, we propose the following decision-tree for optimal selection of the ASD closure technique according to the patient’s and setting’s parameters. Table 5 summarizes advantages, appropriate indications, and further restrictions of each technique, and the following section details the appropriate indications of each technique.
Summary of advantages, proposed specific indications and restrictions of the currently available options for atrial septal defect (ASD) closure.
Indications of TTE
Transthoracic echocardiography represents a safe, cost-effective, and efficacious technique in transcatheter ASD device closure. These advantages justify its use as the technique of choice in order to systematize the related safety benefits. In addition, TTE could be proposed for patients with contra-indications for TEE, such as esophageal malformations or surgically repaired tracheoesophageal fistula or failure of the transesophageal probe,9 or those with contraindication for general anesthesia. Furthermore, TTE could be an excellent option for low-resources settings.31
Indications of TEE
The use of TEE could be indicated in patients who are eligible for ASD device closure but present with difficult echo windows, such as obese and overweight persons, or those with morphological deformities that impair trans-thoracic echogenecity.22 However, indications of TEE are limited by general anesthesia-related risks.
Indications of surgery
Surgical repair could be indicated in patients with complex anatomical features, such as large ASDs, insufficient rims or severe associated malformations, such as multiple ASDs and ventricular septal defect.20
Indications of intracardiac echocardiography
Intracardiac echocardiography was recently introduced in ASD device closure; although there is controversy regarding its superiority over TEE in delivering high quality images. It remains, however, a costly technique that requires special training.32,33
This study is limited by the retrospective design; where many confounders, such as demographic and anthropomorphic characteristics have not been controlled. In addition, there is discrepancy in the follow-up periods between the TTE and TEE groups, which is related to relatively recent use of TTE in precutaneous ASD closure in our department; this discrepancy may bias the secondary endpoint represented by the late complications. However, the practical objective expected from this study is to feed into a constructive clinical reflection on best indicated technique of ASD device closure, on the basis of preprocedural criteria.
In conclusion, ASD closure guided by TTE showed non-inferiority with regards to achievement of the device deployment and superiority with regards to reduction of procedure and fluoroscopy times, as compared with TEE. Moreover, TTE considerably reduced the use of general anesthesia, which minimized the related risks for patients. The operator-factor did not have impact on TTE outcomes in term of safety and effectiveness; and other factors of failure could not be analyzed due to of the low rate of complications and procedure failure. These findings encourage the use of TTE as the technique of choice of ASD device closure, restricting TEE to specific cases with impaired transthoracic echogenecity or after a prior failed attempt by TTE.
References
*References should be primary source and numbered in the order in which they appear in the text. At the end of the article the full list of references should follow the Vancouver style.
*Unpublished data and personal communications should be cited only in the text, not as a formal reference.
*The author is responsible for the accuracy and completeness of references and for their correct textual citation.
*When a citation is referred to in the text by name, the accompanying reference must be from the original source.
*Upon acceptance of a paper all authors must be able to provide the full paper for each reference cited upon request at any time up to publication.
*Only 1-2 up to date references should be used for each particular point in the text.
Sample references are available from: http://www.nlm.nih.gov/bsd/uniform_requirements.html
Acknowledgment
The author acknowledges Dr. Jamil Al Ata, King Abdulaziz University, Jeddah, for his support and esteemed partnership; and Dr. Mohamed Amine Haireche, Makkah, Kingdom of Saudi Arabia for his precious support in the data analysis of this paper.
Footnotes
Disclosure. Author have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 6, 2016.
- Accepted August 8, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.