


Abstract
Objectives: To investigate the tensile strength of repaired flexor profundus tendons in young lambs, which would be equivalent to repairs in children older than 2 years of age.
Methods: A comparative in-vitro experimental study conducted at King Saud University, Riyadh, Kingdom of Saudi Arabia from October 2014 to December 2015. We utilized 30 flexor profundus tendons of young lambs with a width of 4 mm. All tendons were repaired with a 4-strand repair technique using 4/0 polypropylene core sutures. In group I (n=10 tendons), 2 separate figure-of-eight sutures were applied. In group II (n=10 tendons), simple locking sutures were added to the corners of 2 separate figure-of-eight sutures. In group III (n=10 tendons), the locked cruciate repair was used. All tendon repairs were tested to single-cycle tensile failure.
Results: There was no significant difference between groups II and III with regards to gap and breaking forces; and all forces of these 2 groups were significantly higher than the forces in group I.
Conclusion: It was concluded that 4 mm-wide pediatric flexor tendons allow a 4-strand repair and the use of 4/0 sutures. The use of locking sutures increases the tensile strength to values that may allow protective mobilization in children.
The strength of suture techniques used to repair flexor tendon lacerations in zone II has attracted the attention of hand surgeons for decades.1,2 The most important factor that prevents tendon adhesions and joint stiffness following flexor tendon repair is the institution of an early active rehabilitation protocol. Hence, the repair technique must be strong enough to withstand the gliding forces during early postoperative mobilization. The most important factors affecting the tensile strength of suture techniques used in zone II flexor tendon repairs are: increasing the number of suture strands across the repair; the use of locking rather than grasping suture techniques; the use of larger core sutures; and suture technique configuration.3,4 The size of flexor tendons in children is smaller than adults, both in width and in thickness.5 The application of 6-strand repairs is not easy in these small tendons due to the limited space available for the multi-strand core sutures. The use of 3/0 sutures (commonly used in adult repairs) is also not practical and one has to use 4/0 or 5/0 sutures depending on the age of the child and the size of the tendon.5 Our literature review revealed one biomechanical study investigating the tensile strength of flexor tendon repairs in children less than 2 years of age (the width of flexor profundus tendon in this age group is 1-2 mm).6 There are numerous studies investigating the tensile strength of flexor tendon repairs in adults (the width of flexor profundus tendon in adults is 6-7 mm).3,4 We were unable to find any study investigating the tensile strength of flexor tendon repairs in older children (the width of flexor profundus tendon in older children is 3-5 mm).5 The current biomechanical study utilized flexor profundus tendons of young lambs with a diameter of 4 mm and compared the tensile strengths of 3 suture repair techniques. Our model was meant to simulate and test suture techniques in small flexor tendons, such as those encountered in the pediatric population and the hypothesis was that the strength would be weaker than adults; but locking would increase the tensile strength to values that may allow protective mobilization in this age group.
Methods
The project was approved by the Institutional Review Board of the Ministry of National Guard Health Affairs, Riyadh, Kingdom of Saudi Arabia. The study was conducted at King Saud University from October 2014 to December 2015. Thirty fresh flexor digitorum profundus tendons (4 mm in width and 2 mm in thickness) were harvested from the hind feet of young lambs. The 30 tendons were divided into 3 groups with 10 tendons in each group: groups I, II, and III as shown in Figures 1-3. The 4/0 polypropylene sutures were used for the core sutures in all groups. The core sutures in group I were 2 separate figure-of-eight sutures as described by Al-Qattan and Al-Turaiki.7 Four simple locking sutures (using 5/0 polypropylene sutures) were added to the corners of the 2 separate figure-of-eight core sutures in group II. The figure-of-eight core sutures were applied first (purchasing 7 mm from the tendon) and the sutures were not tied. Next, the locking sutures at the corners were applied so that each locking suture holds one thread of the figure-of-eight suture. After the insertion of the 4 locking sutures, the core sutures were tied first and then the locking sutures were tied. In group III, the locked cruciate repair as described by Barrie et al8 was used. Note should be given that all 3 techniques used were 4-strand repairs.
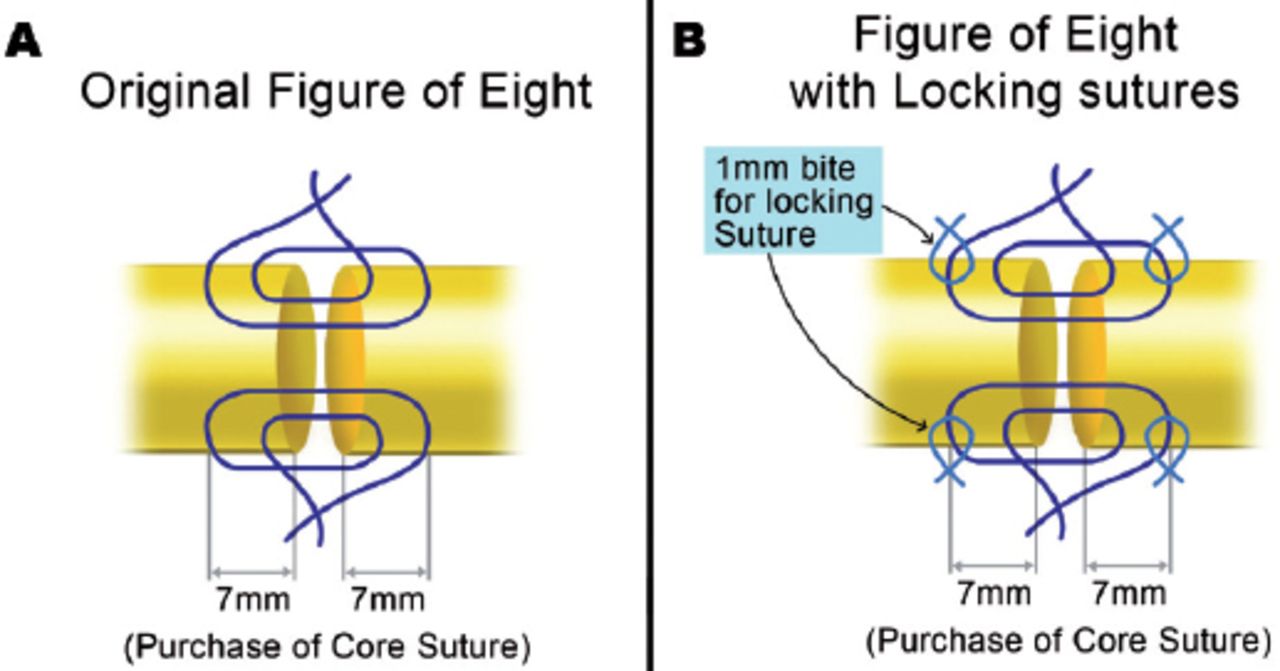
Diagrammatic representation of the 2 techniques of flexor tendon repair used in groups I and II: A) 2 figure-of-eight core sutures (group I), and B) 2 figure-of-eight sutures and 4 separate simple locking sutures (group II).
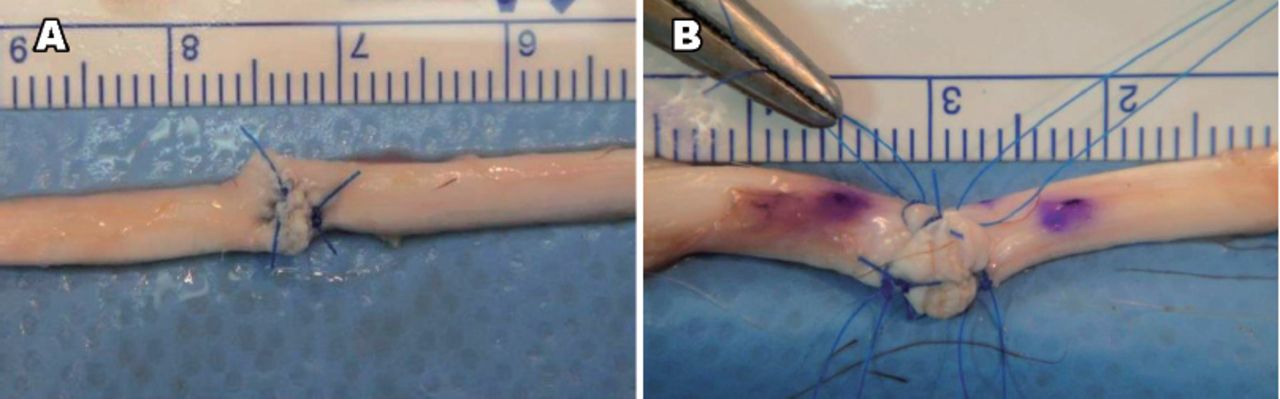
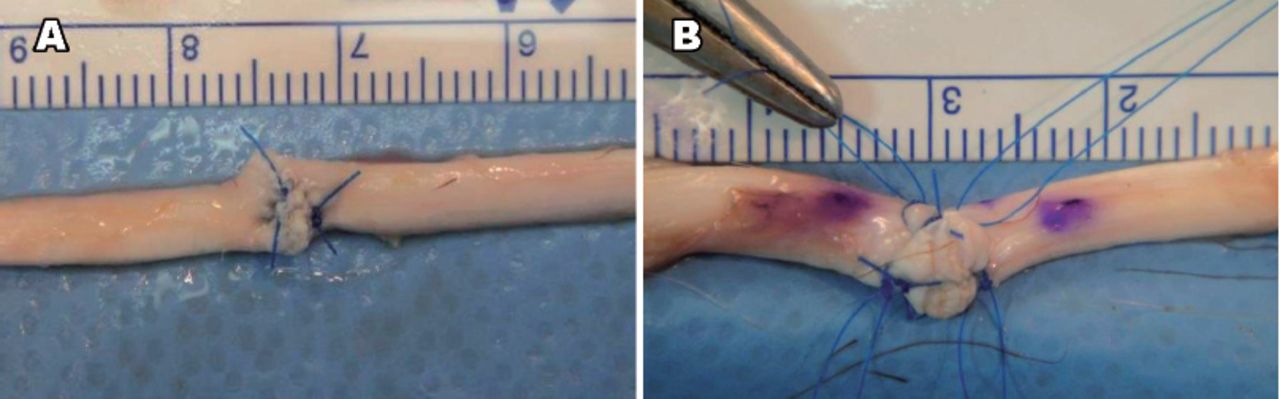
The appearance of the repaired sutures in groups I and II: A) 2 figure-of-eight core sutures (group I), and B) 2 figure-of-eight sutures and 4 separate simple locking sutures (group II).

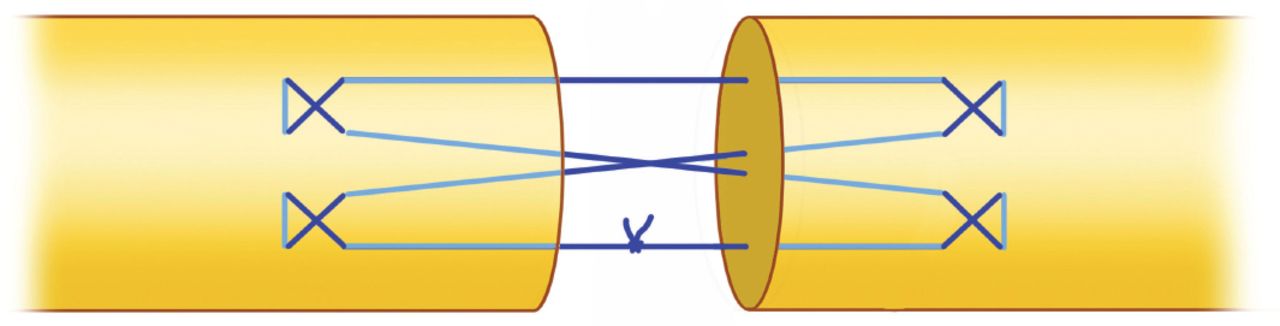
The locked cruciate repair used in group III.
All tendon repairs were tested to single-cycle tensile failure using a tensometer (Intron Canada Ltd., Burlington, Canada). The testing machine has clamps to hold the 2 ends of the tendon being examined. The length of the tendon segment between the clamps was 4 cm. The machine is computerized and the loading speed was set at 20 mm/minute. Two parameters were recorded for each tested tendon: the 2-mm gap force and the breaking strength. The mode of failure (knot failure, suture material breakage, or pulling out of the sutures from the tendon) was also noted.
The tensile strength data were calculated as means and standard deviation and the data of the 3 study groups were compared using the student t-test for independent groups (2-tailed). P-values less than 0.05 were considered significant. Comparison of the mode of failure in the 3 groups were also compared using the Fisher exact test; with p-values less than 0.05 considered significant.
Results
The tensile strength data for the 2 mm gap and breaking forces are shown in Table 1. There was no significant difference (p-values greater than 0.05) between groups II and III with regards to gap and breaking forces; and all forces of these 2 groups were significantly higher (p-values less than 0.05) than the forces in group I.
Gap and breaking forces of the 3 techniques used in flexor tendon repair.
In groups I and II (n=20 tendons repaired with figure-of-eight core sutures), the mode of failure of the repair was pulling out of the sutures from the tendon in 18 cut of 20 repairs. In the remaining 2 repairs (both were in the second group), the mode of failure was core suture breakage. In contrast, the mode of failure in group III (n=10 tendons repaired with locked cruciate core sutures) was suture breakage in 7 repairs and pulling out of the sutures from the tendon in 3 repairs. Statistically, there was no significant difference in the mode of failure between groups I and II. However, the difference was significant for group I versus III; as well as for group II versus III (Table 2).
Comparison of the mode of failure of the 3 techniques used in flexor tendon repair.
Discussion
The current study examined the gap and breaking forces of repairs in 4 mm-wide flexor tendons of young lambs, which would be equivalent to the size of tendons in children older than 2 years of age.5 Our study demonstrated that these small tendons can accommodate 4-strand core sutures using 4/0-sized sutures. We used figure-of-eight core sutures in 2 of the 3 study groups because these core sutures were used in the only available biomechanical study of 1-2 mm-wide flexor tendons of new-born lambs (equivalent to the size of tendons in children less than 2 years).6 Furthermore, data are also available on the breaking forces of repaired adult sheep flexor profundus tendons using the figure-of-eight core sutures.7 This allowed us to compare the tensile strengths of repairs in the same animal (sheep) model using the same core suture technique. In the third group, we used the locked cruciate repair8 since it is a commonly used repair in the clinical setting and we also wished to compare the tensile strength of this locking technique with the 4-corner locking technique in our second group (the latter locking technique has not been previously investigated).
Al-Qattan et al6 demonstrated that the 1-2 mm-wide lamb tendons (which would be equivalent to the size of flexor tendons in children less than 2 years of age) could only accommodate a single figure-of-eight core suture utilizing 5/0 polypropylene suture and the breaking force was 7.5-8.0 Newtons. In another study, Al-Qattan and Al-Turaiki7 measured the breaking forces of 2 and 3 figure-of-eight core sutures used to repair adult sheep flexor profundus tendons (6-7 mm in width) utilizing 3/0 polypropylene. The mean breaking forces in these adult tendons were 73.1 and 95.3 Newtons. The mean breaking force of our first technique (2 figure-of-eight sutures in 4 mm-wide tendons using 4/0 polypropylene) was only 25.2 Newtons. The lower values in pediatric tendons are multi-factorial and are not only related to the use of smaller core sutures and the smaller number of strands crossing the repair. The figure-of-eight core sutures grasp the full-thickness substance of the tendon. Al-Qattan5 stressed on the fact that pediatric tendons are not only narrower in width, but they are also thinner than adult tendons. There is less tendon substance to grasp by the core sutures in thinner tendons; and this is expected to affect the tensile strength.3,4 Another potential factor is the different stiffness/collagen fiber diameter of flexor tendons in children, which will also influence the tensile strength.9 For example, tendon repairs applied to the palmar aspect of the profundus tendon is weaker than repairs applied to the dorsal aspect of the tendon; and this has been linked partly to the smaller collagen bundle size within the palmar aspect.10
Using adult tendons and 3/0 sutures, Barrie et al8 showed that the mean breaking strength of the locked cruciate repair was 78 Newtons. Our study showed that a similar repair (with 4/0 sutures) in 4 mm-thick tendons would have a much smaller strength (a mean of 35.2 Newtons); once again, emphasizing the influence of tendon and suture sizes on the tensile strength values. We noted that the application of the locked cruciate repair in small tendons was more technically demanding than the figure-of-sutures. In the former repair, the multiple entrances and exits of the needle had to be applied carefully through the 2 mm-thick tendons. The thickness of the tendon was not an issue while placing the figure-of-eight sutures, because these core sutures grasp the full-thickness substance of the tendon.
In the past, the modified Kessler 2-strand repair was used by most surgeons in repairing flexor tendons in zone II.11,12 The breaking strength of this repair in adult tendons varied in the literature and ranged from 13 Newtons (using 4/0 sutures) to 35 Newtons (using 3/0 sutures).11,12 Our study showed that the use of locking sutures (in groups II and III) in 4 mm-wide tendons will increase the breaking forces to mean values greater than 35 Newtons (namely, greater than the tensile strength of the modified Kessler repair in adult tendons using 3/0 sutures). Early active mobilization has been used successfully in adults for several decades following the modified Kessler repairs.
Al-Qattan5 reviewed the literature and found that most hand surgeons will completely immobilize the hands of pre-school children following flexor tendon repair in zone II. The results of our study support this concept due to the relatively low tensile strength of repairs in 4 mm-wide tendons. These young children are known to have frequent inadvertent grasping leading to rupture of the repair even when the hand is completely immobilized in a cast.13 Hence, the search for stronger repairs (such as, with the addition of locking or anchor points) is still worthwhile in these young children.
In our study, we measured both the gap and the breaking forces. Excessive gapping at the repair site allows excessive scarring, and is known to affect the clinical outcome of flexor tendon repair.14 Our study showed that the gap forces of the 2 locking techniques (groups II and III) were significantly higher than the non-locking technique (group I) (Table 1). Biomechanically, gapping following flexor repairs may be viewed in different ways according to core suture configuration. The presence of a transverse component in the core suture (such as, the Kessler repair) allows early gapping. Upon loading of the repair, the transverse part of the Kessler sutures narrows, allowing the 2 longitudinal parts to lengthen; leading to early gapping15 (Figure 4A). The core sutures in our 3 experimental groups have no transverse component. The repair in group I is a grasping technique without locking; and this is expected to allow early teasing-out of the core sutures; leading to early gap formation (Figure 4B). The presence of the corner locking sutures in group II helps to decrease this early gapping (Figure 4C). In group III, the initial tension upon axial loading occurs at the locking parts of the core suture; and these act as anchor points to prevent gapping11 (Figure 4D).
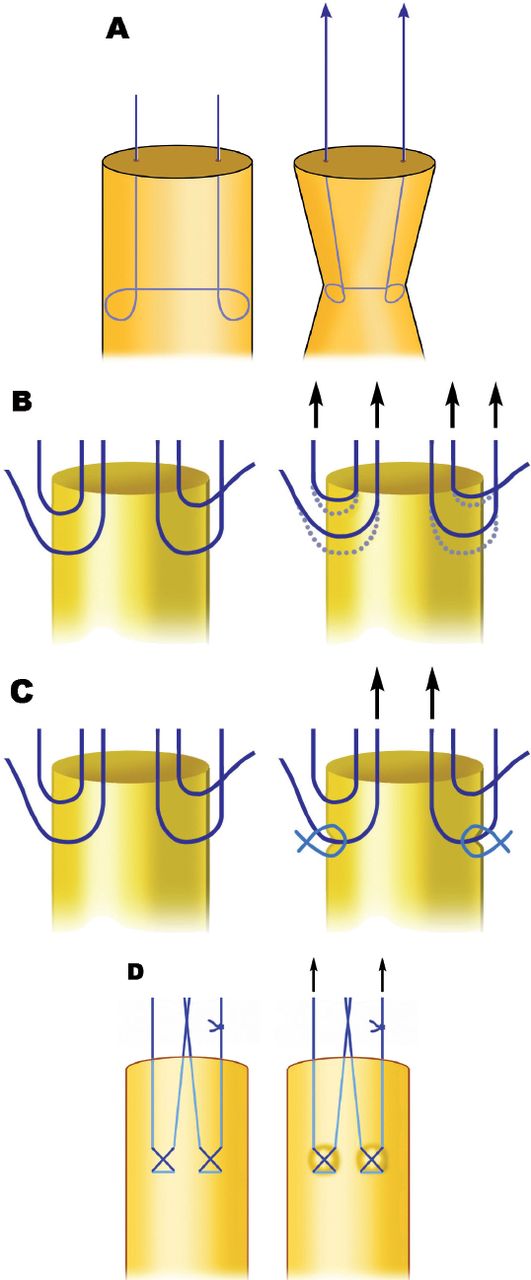
Gap formation upon axial loading with different core sutures showing: A) a grasping suture with a transverse component such the Kessler core suture, B) a grasping suture without a transverse component such the figure-of-eight core sutures, C) figure-of-eight core sutures with corner locks, and D) a locking technique with cross-locks, such as the locked cruciate repair.
The failure of locking repairs usually occurs due to suture breakage; whereas pulling out of sutures is usually seen in grasping repairs. One of the most popular locking suture techniques is the locked cruciate repair. When tested biomechanically, most locked cruciate repairs fail by suture breakage.16 In our study, all 10 grasping repairs (group I) and 8 out of 10 locking repairs (group II) failed by pulling out of sutures; and the difference in the mode of failure between these 2 groups was not significant (Table 2). In contrast, 7 out of the 10 cruciate repairs (group III) failed by suture breakage; and this significantly different from the mode of failure of groups I and II (Table 2). This indicates that the corner locking sutures are not as effective anchors as the cross locks of the cruciate repair. It is important to note that the corner locking sutures in group II were simple separate sutures, while the locking sutures of all other locking repair techniques in the literature (including the locked cruciate repair) were incorporated in the configuration of the core sutures.
Our model was meant to simulate and test suture techniques in small flexor tendons, such as those encountered in the pediatric population; and this was meant to address a gap in the literature on tensile strength of flexor tendon repairs in young children. The most important message from our model is that 4 mm-wide pediatric flexor tendons would allow a 4-strand repair and the use of 4/0 sutures. Furthermore, we demonstrated that the use of locking sutures may increase the tensile strength to values that may allow protective mobilization in this age group. However, the study has several limitations.
Firstly, being an original ex-vivo study on the topic, the study is not expected to answer all questions; including those with clinical relevance. For example, will the use of locking techniques reduce the rupture rate in those young children in the clinical setting? Furthermore, the applicability of early active mobilization in young children is limited to few hand centers;5,17 since most surgeons completely immobilize the injured hands of young children following flexor tendon repair.
Secondly, our ex-vivo study may not correlate with the in-vivo evaluation of gliding through the flexor sheath. For example, the 4 additional corner locking sutures are expected to add more bulk to the figure-of-eight sutures and would likely require more liberal venting of the pulleys in the clinical setting.
Thirdly, the study does not address other potential factors that may affect the gap and breaking forces in tendon repairs, such as: cyclic loading; the use of braided rather than monofilament sutures used in our study (the latter is known to be weaker in adult tendon repairs);18 and the use of peripheral sutures.18
Finally, pediatric human tendons may not be as stiff as young sheep flexor tendons; and this is expected to affect the tensile strength and gap formation values.9,10 In our model, we used the distal parts of the sheep flexor tendons (to simulate zone II tendon injuries) and we noted that these are much stiffer than human pediatric flexor tendons in zone II. Stiffer tendons hold sutures better and this may explain the effectiveness of the small corner sutures in group II repairs despite the small bites in small tendons. Hence, there is a need for biomechanical studies in human pediatric tendons. All these issues have been well studied in adult tendons and need to be addressed in pediatric tendons in separate research studies.
In conclusion, the use of locking sutures in pediatric tendons may increase the tensile strength to values that may allow protective mobilization in this age group.
Acknowledgment
The authors would like to thank Medical Illustrator Mr. Virgilio Salvador from the King Saud University, Riyadh, Kingdom of Saudi Arabia for drawing Figures 1-4.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company. This study was funded by the College of Medicine Research Center, Deanship of Scientific Research, King Saud University, Riyadh, Kingdom of Saudi Arabia.
- Received March 16, 2016.
- Accepted June 10, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.