


Abstract
Objectives: To assess the association of adenomyotic foci with co-existing benign ovarian cysts.
Methods: This prospective cross-sectional study consisted of 100 consecutive hysterectomy specimens referred to Histopathology Section of Pathology Department, Peshawar Medical College, Peshawar, Pakistan by its attached teaching hospitals from January 2011 to December 2012. Hematoxylin and eosin stained sections were examined for adenomyotic foci and the presence of co-existent ovarian cysts. For evaluation of estrogen receptor (ER) status immunohistochemical stains were applied and H-scoring system was used with a score >50 as positive.
Results: Out of the 100 hysterectomy specimens, 25 cases had both adenomyosis and ovarian cysts. The ER status of adenomyotic foci was positive in 20% cases and negative in 80% cases. The commonest type of ovarian cyst was hemorrhagic luteal cyst (28%), followed by serous and mucinous cystadenoma (20%) each. Out of the 28% cases of functional cysts, 71.5% were ER positive and 28.5% were ER negative. The p-value for association of ER status of adenomyotic foci with functional cysts was 0.0004; however, p-value was not significant in comparing cases with controls. All 72% cases of nonfunctional cysts were ER negative. However, 44% of functional cysts were not associated with adenomyotic foci.
Conclusion: This study concludes that besides functional ovarian cysts, other local factors may be responsible for the development of adenomyosis.
Adenomyosis is a common debilitating gynecological disorder, which affects women of reproductive age group. It was first described by German Pathologist Carl von Rokitansky in 1860. The name adenomyosis was first used by Frankl in 1925. The current definition of adenomyosis has been given by Bird in 1972 as “benign invasion of endometrium into the myometrium, producing a diffusely enlarged uterus which microscopically exhibits ectopic, non-neoplastic, endometrial glands and stroma surrounded by the hypertrophic and hyperplastic myometrium”.1 The clinical manifestations include abnormal uterine bleeding, colicky dysmenorrhea, dyspareunia, and pelvic pain, particularly during the premenstrual period.2 Traditionally, the diagnosis is made with certainty by microscopic examination of the hysterectomized uterus, but now the accuracy of transvaginal ultrasound and magnetic resonance imaging (MRI) in the preoperative diagnosis of adenomyosis has been established.3 Adenomyotic foci are commonly found in fourth and fifth decade mostly in multiparous women.4 They are also frequently associated with uterine leiomyoma and endometrial hyperplasia.5 In the absence of knowledge on exact etiology, theories including hereditary origin, hormonal factors, endomyometrial junctional zone disruption, viral transmission, and postpartum emdometritis have been put forward.6 It has been suggested that adenomyosis is an estrogen-dependent disease caused by a downward extension of the endometrium into the uterine myometrium due to migratory and invasive properties induced by estrogen on epithelial-mesenchymal cells.7 Therefore, there is an increased risk of adenomyosis with prior uterine surgery, for example, cesarean section, myomectomy, endometrial ablation, dilation and evacuation, and dilation and curettage has been found.8 Recent studies indicate a significant role of localized aromatase activity,9 and tissue injury and repair mechanisms10 in the evolution of adenomyotic foci. Mutations of somatic ERa gene have also been identified in cases of adenomyosis, which suggests that genetic changes could be of relevance for the pathophysiology of adenomyosis.11 Although plenty of work has been carried out on estrogen receptors (ER) distribution and positivity in the growth of adenomyosis,7,12,13 but little data is available on ER positivity of adenomyotic foci in women having co-existing functional ovarian cysts. The objective of this study was to compare the ER status of adenomyotic foci with and without co-existing benign ovarian cysts in total abdominal hysterectomy specimens.
Methods
This prospective cross sectional study consisted of 100 consecutive specimens of total abdominal hysterectomy with bilateral salpingo-oophorectomy (BSO) referred to the Department of Pathology, Peshawar Medical College, Peshawar, Pakistan by its attached teaching hospitals (Kuwait and Mercy Teaching Hospitals) from January 2011 to December 2012.
Inclusion criteria
Total abdominal hysterectomy with BSO specimens in the above study period were taken. Out of these cases, patients having an ovarian cysts with concomitant adenomyosis were included in the study. An identical number of cases of adenomyosis without ovarian cysts were taken as controls.
Exclusion criteria
Patients having any malignancy were excluded from the study.
Ethical considerations
Informed consent from the patients was obtained before recording the data of history, clinical findings, and relevant investigations. The integrity and impartiality of the research was ensured according to the Ethical Principles of Medical Research involving human subjects in accordance with the Declaration of Helsinki 1964.14 The study was Also approved by the Institutional Ethical Committee.
Tissue processing of specimen
The tissue processing of specimen was conducted at the Histopathology Section of the Department of Pathology, Peshawar Medical College, Peshawar, Pakistan. Each hysterectomy with BSO specimen was grossly examined in detail. The representative sections from the wall of the uterus, adenomyotic lesion, and both ovaries were taken and processed for hematoxylin and eosin stain. The microscopic findings were recorded.
Diagnostic criteria
The criteria for the diagnosis of adenomyosis was taken by the presence of: 1) Endometrial glands/stroma or both at one low power (2.5 mm) depth from the basal endometrium; and 2) Plump/hypertrophied smooth muscle fibers immediately surrounding the endometrial tissue deep in the myometrium.
Immunohistochemistry
Immunohistochemical (IHC) stain was performed at the Department of Pathology, Institute of Medical Sciences, Islamabad, Pakistan. A section from the adenomyotic lesion was taken from both cases and controls for IHC staining for ER by using the Novocastra Max Polymer Detecting System (Leica Biosystems Ltd., Newcastle, United Kingdom). The immunohistochemically stained slides were examined microscopically, and the ER positivity was assessed by using the H-scoring system taking nuclear staining with a score >50 as positive.15
Statistical analysis
The statistical analysis was carried out using the Statistical Package for Social Sciences version 19 (IBM Corp., Armonk, NY, USA). The difference between positive and negative ER status of adenomyotic foci and ovarian cysts was analyzed by using Fischer’s exact test. The difference between the ER status of the cases and controls was analyzed using the Chi Square test. The value of p≤0.05 was considered statistically significant.
Results
Out of the 100 specimens of hysterectomy with BSO, 25% had adenomyotic foci with ovarian cysts. The age of the patients with adenomyosis ranged from 30-60 years, and was more commonly found between 40-49 years (60%) standard deviation ±5.2. Out of these 25 cases, 76% were multiparous and 24% nulliparous. Histologically, all the cases were diagnosed as having chronic cervicitis. Besides, most also had leiomyoma (80%) followed by endometrial hyperplasia (44%), chronic endometritis (12%), and endometrial polyp (12%). Among adenomyotic foci, 20% cases were positive for ER, while 80% cases were negative. The details of histologic type of ovarian cyst and its relationship with ER positivity of adenomyotic foci are given in Table 1.
Ovarian cysts with ER status of adenomyosis.
In ER positive adenomyosis cases with cystic lesions in ovary 03 (60%) had follicular cysts, while 02 (40%) showed cystic follicles (Figure 1). The ER expression of adenomyotic foci in relation to functional and nonfunctional ovarian cysts was statistically highly significant (p=0.0004). The ER expression of cases and controls is given in Table 2. The p-value of ER status of adenomyotic foci in cases and controls was found to be insignificant. Furthermore, the details of ovarian cysts without concomitant adenomyosis is given in Table 3. The comparison of functional and nonfunctional ovarian cysts with and without adenomyosis resulted with a value of p=0.1572, which is statistically insignificant (Table 4).
Estrogen receptor (ER) expression of adenomyotic foci with concomitant ovarian cysts.
Estrogen receptor (ER) status of cases and controls.
Ovarian cysts without concomitant adenomyosis.
Comparison of functional and nonfunctional ovarian cysts with and without adenomyosis.
Discussion
Adenomyosis is always disguised behind other associated uterine pathologies until discovered with the help of ultrasound, or more commonly found on hysterectomy for other complaints. Therefore, patients have suffered and gynecologists are confused on how to handle adenomyosis. The clinical presentation is often masked by signs and symptoms due to leiomyomata, endometrial hyperplasia, and endometritis so that timely treatment for the adenomyosis is delayed. We aimed to find an association of adenomyosis with co-existent benign ovarian cysts and their possible role in its causation.
Adenomyosis peaks when a woman enters the menopausal transition period with ovarian ageing and concomitant hormonal changes, and characteristically presents as abnormal uterine bleeding in most of the cases.5 Similarly, most of our patients with adenomyosis (60%), fell in the age range of 40-49 years. This fifth decade predominance was reflected as 67%16 and 69.3%17 nationally, 46.3%18 and 51%19 regionally, and 45%20 internationally. In our study, the age range coincides with parity, because the prevalence was twice as high in multiparous women than in nulliparous, a relationship, which has been reflected in other studies.20,21 Repeated pregnancies may facilitate formation of adenomyosis by allowing adenomyotic foci to be included in the myometrium due to the invasive nature of the trophoblast on the extension of myometrial fibers.22
Adenomyosis was found in 25% of hysterectomies in our study. Figures ranging from as low as 5% and as high as 70% have been reported,23 but most studies corroborate our findings nationally 20.6%,16 regionally 23.4%,24 and internationally as 24.9%.20 The results from Karachi are exceptionally high (56.5%),17 which the authors claim that the condition might have been underdiagnosed in the past, but it could be due to the sampling technique, because when 3 routine sections were taken in a study, 31% of hysterectomy specimens contained adenomyosis and at 6 sections, the rate increased to 61%.25
Among other pathological entities in our study, association of adenomyosis with uterine leiomyomata was found in 80% of cases, which was equally common in the group without adenomyosis and is much higher than another study carried out in Khyber Pakhtunkhwa province in Pakistan (39%),16 and a study conducted in India (12.2%).18 Conversely speaking, in a study of leiomyomata 33.3% cases also had adenomyosis.22 The reason for a higher figure in our cases can be because all the 25 cases had concomitant benign ovarian cysts, which may influence the formation of leiomyomata through production of estrogen and progesterone besides other factors.26
Endometrial hyperplasia was seen in 44% cases, endometrial polyp and chronic endometritis in 12% each. The comparable figures are for endometrial hyperplasia 13%16 and 23%27 and for endometrial polyps 4%27 and 25%.16 Although endometrial polyps show a lower figure in our study, endometrial hyperplasia appears significantly on the higher side and the explanation can be the same as for a high percentage of leiomyomata. In our study, the endometritis appears to be a coincidental finding and may not have a direct association with adenomyosis.
Various authors have performed studies related to adenomyotic foci and ovarian cysts, but none of them commented on their co-existence and correlation with ER positivity of adenomyotic foci. For example, in a case-series, 21.4% of hysterectomies with adenomyosis were associated with ovarian cysts, but were not correlated with ER status of adenomyotic foci.28
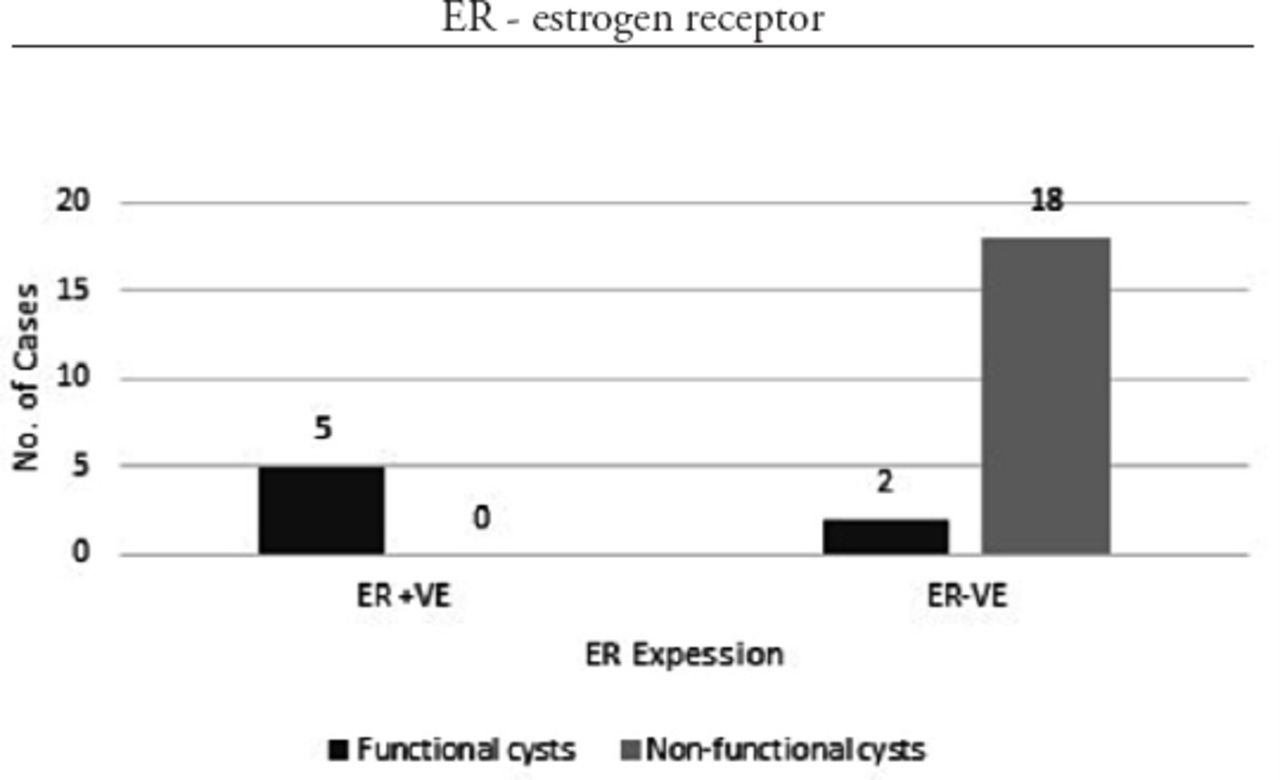
In our study, the adenomyotic foci were ER positive in 71.5% cases of cystic follicles and follicular cysts, but all the adenomyotic foci associated with non-functional cysts were ER negative. The p-value was 0.0004, which is statistically highly significant (Figure 1). Cystic follicles and follicular cysts are functional cysts and contain estrogen in their luminal fluid, especially follicular cysts,29,30 but non-functional ovarian cysts do not secrete estrogen.31
In contrast to the previous findings in our study, there was also a significant number of functional ovarian cysts with no concomitant adenomyosis, which included cystic follicles (22.7%) and follicular cysts (21.3%) (Table 3).
No statistically significant results could be obtained when comparing the ER expression of controls and cases. This indicates other factors, such as aberrant ER gene expression, tissue injury and repair mechanisms, and localized aromatase activity may also be responsible for adenomyosis besides functional ovarian cysts.32 These factors could not be included in our study due to financial constraints.
In conclusion, besides functional ovarian cysts, other factors may be responsible for the development of adenomyosis. Our study also suggests that in a multiparous woman findings of ovarian cysts or leiomyoma on ultrasonography may point at the possibility of concomitant adenomyosis. Patients having abnormal uterine bleeding or diagnosed with endometrial hyperplasia, endometrial polyp, or endometritis should also be investigated for adenomyosis as a cause of their gynecological problem. It is recommended that localized aromatase activity in adenomyotic foci, analysis of contents of ovarian cysts present concomitantly, and genetic aberrations may be studied.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received March 20, 2016.
- Accepted June 22, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.