


Abstract
Objectives: To evaluate the effect of pregnancy on the natural course of Mycosis fungoides (MF) and compare the obtained results with previous reports.
Methods: The medical records of 140 patients with cutaneous T-cell lymphoma (CTCL) treated at the University Hospital of Isfahan (the academic referral center for CTCL) Isfahan, Iran. Between 2000 and 2013 were retrospectively reviewed to retrieve all cases of pregnancy during the course of MF disease.
Results: A total of 8 pregnancies were recorded. The median age of patients at the time of diagnosis was 26.7 (range 21-30 years) and pregnancy 29.4 (range 27-31 years). Most of patients had early-stage MF (Ia and Ib). All patients experienced aggravation of disease during pregnancy or immediately postpartum. Mycosis fungoides did not cause any complications during pregnancy.
Conclusion: Pregnancy appears to have a negative impact on the course of MF, probably due to immune system deteriorations during the pregnancy. Further studies are needed to clarify the interplay between pregnancy and MF.
Mycosis fungoides (MF) is an extra-nodal non-Hodgkin’s lymphoma with primary involvement of the skin.1,2 Mycosis fungoides usually has an indolent course and a good prognosis when identified in its early stages.3-5 The peak age at presentation of the disease is 55-60 years, with a 2:1 male to female ratio in Western countries.6,7 Due to the low prevalence of MF, the peak age at presentation (middle age), and the male gender preference, MF coincident with pregnancy is rare. Nevertheless, the prevalence of MF in Isfahan, Iran, has been estimated at 3.91 per million persons with a median age at presentation of 43 years and a male to female ratio of 3:4.8 Thus, these unique epidemiological characteristics have enabled us to study a number of concomitant pregnancy and MF cases. The literature reviewing concomitant MF and pregnancy is strikingly limited; therefore, the correlation between pregnancy and MF remains unknown. Some reports have shown that MF does not worsen during pregnancy and the postpartum period, and concluded that MF did not adversely affect pregnancy outcomes;9 however, there is a continued controversy regarding the effect of pregnancy on the progression of MF.10 The aim of this study is to evaluate the effect of pregnancy on the natural course of MF and compare the obtained results with previous reports.
Methods
This is a single-center, retrospective cohort analysis of cases treated at the Primary Cutaneous Lymphoma Center of Isfahan, University of Medical Sciences, which is the main referral center for primary cutaneous lymphoma. This study was approved by the Ethics committee of Isfahan, University of Medical Sciences. Isfahan, Iran. The medical records of 140 MF patients dating between 2000 and 2013 were retrospectively evaluated to detect female patients who had been pregnant during the course of the disease. For pregnant cases with MF, the patient’s demographic characteristics, details of staging, treatment modalities, disease status before and after pregnancy, and complications during pregnancy were retrieved. The definition of MF in our study is consistent with the International Society for Cutaneous Lymphoma algorithm for uniform diagnostic criteria in MF.3 Descriptive statistics were performed to summarize the patients’ characteristics. For statistical analysis, the Statistical Package for Social Sciences version 20 (IBM Corp., Armonk, NY, USA) was used.
Results
We identified 6 MF patients who had been pregnant during the course of their disease. Four patients were on their first gestation and 2 patients had 2 pregnancies during the course of their disease; therefore, a total of 8 pregnancy cases, were reviewed. The median age of patients at the time of diagnosis 26.7 (range 21-30 years) and pregnancy 29.4 (range 27-31 years). The patient characteristics are summarized in Table 1. Immunohistochemistry was possible in all cases. Five cases showed predominant CD4-positive epidermotropic infiltrates (Figure 1) and in one case the lymphocytic infiltration was CD4- and CD8-negative. Four of the patients had monoclonal TCR gene rearrangement. Most patients were staged as Ia or Ib and only one case was stage IIIa. All patients were in complete remission before pregnancy, except for one case, which had been newly diagnosed (patient 3). In all cases, the erythematous scaly patch/plaque areas were histologically confirmed as present during the course of pregnancy and at postpartum (Figure 2). One case was afflicted by erythrodermic and tumoral lesions. Except for one case that had anaplastic large cell transformation, none of the other patients experienced progression to advanced stages (Table 2). Most relapse cases occurred in the first 2 months after childbirth; however, 2 cases showed progression (patient 3) and relapse (patient 6) of disease during pregnancy. The patient who was diagnosed as stage IIIa before pregnancy refused the recommended treatment during pregnancy, but underwent combination chemotherapy during the puerperium period. Other patients who had flares shortly after delivery were treated with narrow-band ultraviolet B phototherapy. All patients had normal pregnancy and normal delivery, except for one ectopic pregnancy (patient 2). No complications were observed during the gestational period. The outcomes of the 7 pregnancies were normal and healthy neonates were delivered (Table 2).
Demographic data of 6 pregnant patients with mycosis fungoides.

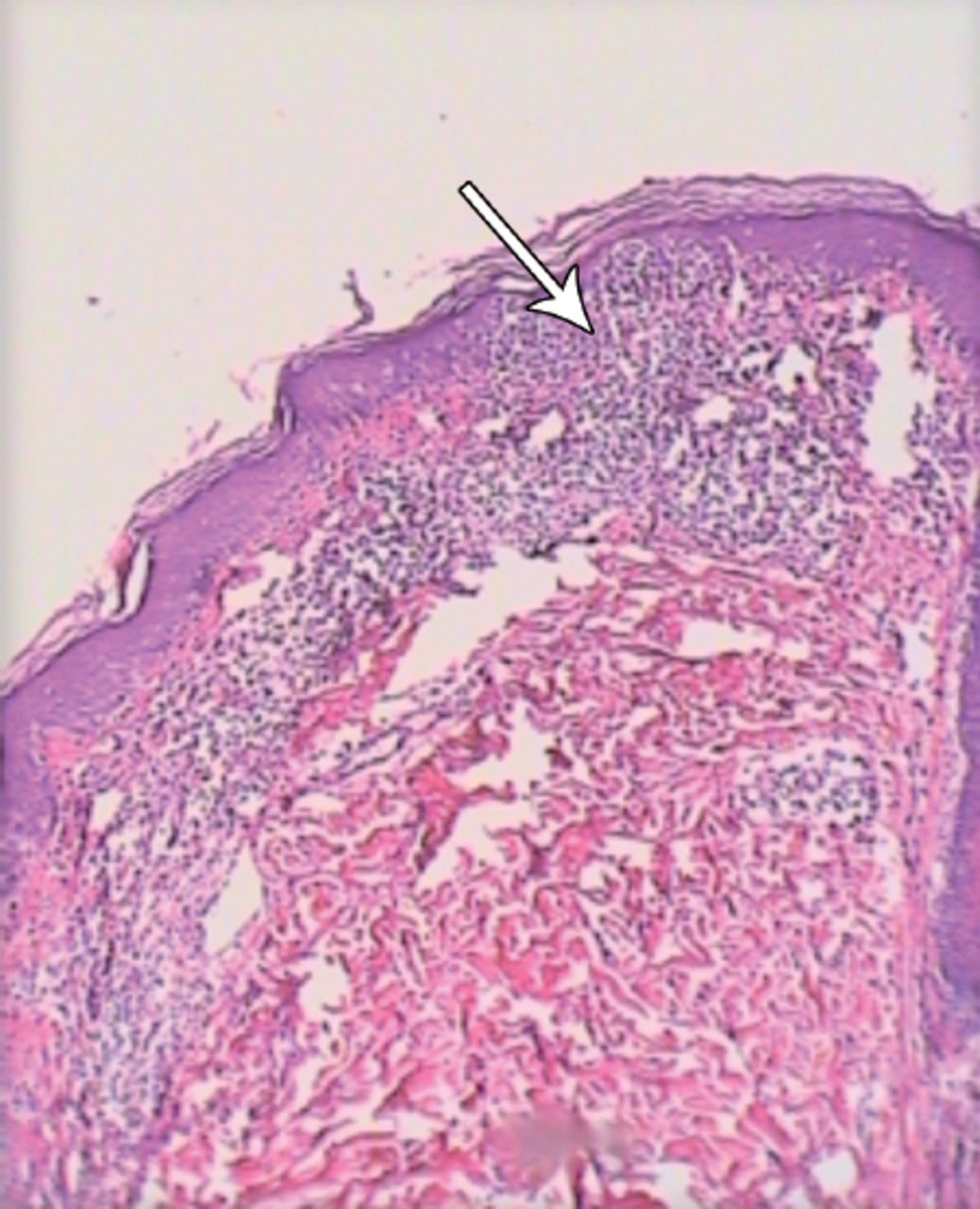
Histopathological feature of the patch stage of mycosis fungoides. Sections from the patch show epidermotropism of atypical lymphocytes, mostly in basal layer and dermis, mild interstitial infiltrate of small lymphocytes are seen (Hematoxylin and eosin ×100) (arrow).

Mycosis fungoides, an erythematous scaly patch in the upper part of left tight in a 31 years-old female during pregnancy.
Exacerbation and progression of MF in pregnant patients and their treatment plan.
Discussion. The results of the present study showed that all patients experienced disease relapse, or aggravation during the course of pregnancy, or shortly after delivery. Nevertheless, MF did not adversely affect pregnancy outcomes, as suggested in previous reports. Immunophenotyping studies11 have revealed that MF is one of many cutaneous T-cell lymphomas, typically of the CD4 helper T-cell phenotype. Recent studies,12,13 suggest that CD8-positive cytotoxic T-cells play a crucial role in the antitumor response in MF; a correlation between high percentages of CD8-positive cytotoxic T-cells in the dermal infiltrates and better survival has been described. The CD8-positive T-cells exert their antitumor effect through a direct cytotoxic effect as well as by the production of cytokines, particularly interferon. Further more, they can mediate tumor cell lysis by exocytosis of cytotoxic granules containing perforin, granzymes, and T-cell intracellular antigen, and by expression of the Fas ligand, which interacts with Fas on the neoplastic T-cells.12,13 Both pathways ultimately lead to the activation of caspase 3 and tumor cell death.14 Decline in the number of peripheral blood CD8-positive T-cells, natural killer cell, and increasing circulating malignant T-cell totally associated with progression of MF.15 A gradual shift from a predominantly type I cytokine profile in MF plaques to a predominantly type 2 cytokine profile in MF tumors has been suggested.16 Also, a similar shift toward T-helper type 2 immunity has been suggested during the pregnancy.17 Therefore, the lack of strong maternal cellular immune response, and a more dominant humeral immune response toward the fetus have been thought to promote maternal acceptance of the fetal allograft.18 Thus, the decreased immune response accounts for the findings of the present study regarding flares and the occasional progression of MF during pregnancy and postpartum. Nevertheless, very little is known regarding the exact relationship between MF and pregnancy, and there is no clear consensus concerning the effect of pregnancy on MF flares and the effect of MF on pregnancy outcomes. Castelo-Branco et al,19 reported of a pregnant woman with advanced-stage MF around the conception time that managed with photon radiotherapy during the pregnancy, the outcome of her pregnancy was good and a healthy neonate was delivered. In another case report in 2001, Echols et al,20 described 3 cases of pregnancy with MF, but only one case of a 26-year-old black woman diagnosed to be suffering from MF showed an increase in skin lesions. At the commencement of her third trimester, she presented with an acute exacerbation of MF, and complete remission with trial treatment with alpha-interferon was achieved. In a series of 9 pregnant women with MF,21 there was no evidence confirming the change of course of MF during pregnancy. They reported that pregnancy appeared to have had no impact on the course of early-stage of MF.21 In 2012, Ozturk et al,22 described a 30-year-old pregnant woman with MF in its early stages. They concluded that there were no changes in the severity and frequency of the lesions both during pregnancy and in the postpartum period. Our findings regarding the exacerbation or even the progression of MF, correlate well with some of the previously mentioned reports. The limitations of this study were the short mean duration of follow-up, and the small sample size of subjects. Nevertheless, larger, long-term studies must be performed in order to firmly establish the exact relationship between MF and pregnancy.
In conclusion, on the basis of cases presented and the observed immunosuppression that occurs during pregnancy, in particular, the relative bias toward T-helper type 2 immunity, it follows that pregnancy may cause exacerbation or even progression of MF. However, on the contrary, MF does not have an adverse impact on pregnancy.
Illustrations, Figures, Photographs
All figures or photographs should be submitted in a high resolution (minimum 300 DPI) (electronic version saved in jpeg or tiff format. Original hard copies of all figures may be requested when necessary. Photographs will be accepted at the discretion of the Editorial Board. All lettering, arrows, or other artwork must be done by an artist or draftsman. If arrows are used please ensure they appear in a different color to the background color, preferably black with a white border, or white with a black border. If arrows distinguish different items on the figure then different arrow styles should be used ie. long, short, wide, narrow. Written informed consent for publication must accompany any photograph in which the subject can be identified. Written copyright permission, from the publishers, must accompany any illustration that has been previously published.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received May 26, 2016.
- Accepted June 29, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.