


Abstract
Objectives: To discuss our center’s experience with acute respiratory distress syndrome (ARDS) secondary to pulmonary tuberculosis (TB) in a major tertiary referral hospital in the Kingdom of Saudi Arabia.
Methods: A retrospective review of medical records of all patients with community-acquired pneumonia secondary to mycobacterium TB infection who were admitted for critical care in a single center of King Abdulaziz Medical City, Riyadh, Kingdom of Saudi Arabia from 2004 to 2013.
Results: In our review of 350 patients with community-acquired pneumonia admitted to Intensive Care Unit, 11 cases of TB complicated with ARDS were identified. The mean age of patients was 51.9 years. The median time from hospital admission to pulmonary TB diagnosis and start of therapy was 5 days, while the median time from onset of symptoms to initiation of treatment was 18 days. The mortality rate was 64%, and the median length of hospital stay before death was 21.4 days. Delayed treatment, as well as high acute physiology and chronic health evaluation II and CURB-65 scores at presentation, were independent risk factors for death.
Conclusion: Patients with pulmonary TB infrequently present to intensive care with acute symptoms that meet all criteria for ARDS. Such a presentation of TB carries a high mortality risk.
Tuberculosis (TB) is the seventh-leading cause of death in the world, and pulmonary TB is, by far, the most common presentation of this infection.1 Usually, pulmonary TB presents as chronic pneumonia, with approximately 4 weeks between symptom onset and the first health consultation.2 The reported frequency of acute respiratory failure in patients with active TB ranges from 1.5-5%.3,4 The presentation ranges from acute respiratory failure in miliary TB to acute respiratory distress syndrome (ARDS).3 Agrawal et al4 reported that up to 4.9% of TB cases presented as ARDS in India, and in 22% of these cases, ARDS occurred after treatment for miliary TB.4-6 Kingdom of Saudi Arabia (KSA) is an intermediate-risk country for TB.7,8 According to the Saudi Ministry of Health, the incidence of pulmonary TB was 16 cases per 100,000 annually.8 Acute respiratory failure and ARDS complicating pulmonary TB are associated with high mortality, and early recognition and treatment initiation are crucial in our patient population. There is still limited information on this syndrome from KSA despite a relatively high incidence rate. In this study, we present our experience with ARDS secondary to pulmonary TB in a major tertiary referral hospital in KSA.
Methods
We retrospectively reviewed the patient database of the intensive care unit (ICU) of King Abdulaziz Medical City, Riyadh, KSA for all patients with severe community-acquired pneumonia (CAP) who were admitted to this unit from 2004 to 2013. Out of the CAP cases, we selected and reviewed the records of all patients with a final diagnosis of pulmonary TB.
The King Abdulaziz Medical City Hospital is a 1,500-bed, tertiary-care, referral hospital located in Riyadh, KSA. The ICU, which includes general, trauma, surgical, neurosurgical, and intermediate care units, has a total capacity of 62 beds and is among the largest in the city.
The following data on the patients admitted with a CAP diagnosis were recorded: age, gender, coexisting medical problems, medications, acute physiology and chronic health evaluation (APACHE) II scores, CURB-65 severity score for pneumonia, blood gas analyses, blood chemistry analyses, respiratory culture results, length of stay in the ICU, requirement and duration of mechanical ventilation (MV), complications developed in the ICU, and mortality status. Radiological data, including chest x-rays and CT scan findings, were obtained from radiology reports in the electronic health records. For patients with pulmonary TB, we obtained further lab results including human immunodeficiency virus (HIV) status, TB Gold test results, acid-fast bacilli (AFB) stain and polymerase chain reaction (PCR), TB culture, and drug sensitivity of the Mycobacterium TB (MTB) complex. The Ethics and Scientific Committee of King Abdulaziz Medical City approved the study.
Definitions
Tuberculous pneumonia was defined as a parenchymal, pulmonary TB disease that was neither miliary nor disseminated. A diagnosis of pulmonary TB requires a positive culture from respiratory samples or a suggestive histopathological sample from an open lung biopsy. A diagnosis of pulmonary TB is also made if there are clinical and radiological improvement after starting anti-TB drugs that cannot be explained by any other intervention. Miliary TB was defined as active TB with micronodules in a miliary pattern seen on chest x-rays or CT scans. Disseminated TB was defined as active TB without a miliary pattern, but involving at least 2 extrapulmonary sites.
The diagnostic criteria of TB-destroyed lungs include: the presence of radiological findings of destroyed lung parenchyma, lung volume loss, or secondary bronchiectasis changes as seen on plain chest x-ray images or CT scans with or without a history of TB.9-11 The diagnosis of ARDS was based on the Berlin definition of this syndrome: acute; diffuse; inflammatory lung injury; leading to increased pulmonary vascular permeability; increased lung weight; and loss of aerated lung tissue with hypoxemia and bilateral radiographic opacities; associated with increased venous admixture; increased physiological dead space; decreased lung compliance; and a ratio of partial pressure arterial oxygen and fraction of inspired oxygen (PaO2/FiO2) lower than 300.12
Statistical analyses
Continuous variables, such as age, weight, glucose levels, partial pressure of oxygen, and CURB-65, were reported as medians by mortality status (survivors versus non-survivors). Categorical variables, such as gender, diabetes mellitus, and smoking status, were reported as numbers and percentages by mortality status. Fisher’s exact test was used to compare the demographic and clinical presentation characteristics of survivors and non-survivors. The Mann-Whitney U test was used to conduct unadjusted comparisons between mortality status groups regarding patient age, weight, glucose levels, APACHE II score, and laboratory test results. P-values of less than 0.05 were considered significant.
Results. Out of the 350 patients with severe CAP who were admitted to ICU during the study period, 11 patients (6 men and 5 women) were diagnosed with pulmonary TB, which represented 3.1% of total admissions. All of these patients were also diagnosed with ARDS. The mean patient age was 51.9 years. The mean duration of symptoms was 11 days (2 to 28 days). Cough was present in all 11 cases and was productive in 9 patients; no hemoptysis was documented for any of the patients. Fever was present in 5 patients, and weight loss was observed in 4 patients. The median time to TB diagnosis was 5 days, whereas the median time from onset of symptoms to completion of treatment was 18 days. Only one of the 11 patients had been diagnosed with pulmonary TB 6 months before admission to the hospital, but was not receiving treatment, whereas the rest of the patients were not known to have TB before their presentation with severe CAP. Only one patient had a prior TB history. Tuberculosis as a cause of CAP was suspected upon admission in 6 (54.5%) of the patients. However, in 5/7 (71.4%) of the survivor group and 1/4 (25%) of the non-survivor group, p=0.242. The suspicion was derived mainly from radiological findings in 5 cases and in one patient by clinical history. Empirical treatment was commenced in only one patient before TB confirmation. Acute respiratory distress syndrome developed in 2 patients after starting anti-TB medication. One patient had a previous positive culture that had been missed and was started on therapy upon admission, while the other was admitted to medical ward as CAP and started on empirical therapy complicated with ARDS. His culture turned out to be positive.
One patient had a miliary pattern in the chest x-ray scan, whereas 3 met the criteria for disseminated TB. Eight patients had bilateral involvement, whereas multiple lobe involvements were present in 9 patients. Upper lobe involvement was present in 6, pleural effusion in 5, a cavitary disease in 4, and an interstitial pattern in 3 patients. Chest CT scans were performed in 6 patients and suggested a diagnosis of TB in 5 patients. Human immunodeficiency virus testing was conducted for only 6 patients, and one patient tested positive. Sputum smears were positive for AFB in 6, whereas PCR analysis of sputum was positive in 3 of the 4 patients tested. Bronchoalveolar lavage was carried out in 6 patients, and AFB smear was positive in 3.
Of the 11 patients, 8 required MV on admission, whereas 3 patients were initially managed with nasal intermittent positive pressure ventilation, but required MV within 48 hours. Four patients were eventually discharged from the ICU, whereas 7 patients died resulting in a mortality rate of 64%. The median APACHE II score was 19, while the CURB-65 severity index score was 2 for the whole group. Non-survivors had a significantly higher CURB-65 severity score (p=0.042). The APACHE II score was not statistically different among survivors and non-survivors (20 versus 13, p=0.267). The median duration of hospital stay was 21.4, and treatment before death was 10.8 days (Table 1).
Demographic and presentation variables of patients with community-aquired pneumonia secondary to mycobacterium tuberculosis infection.
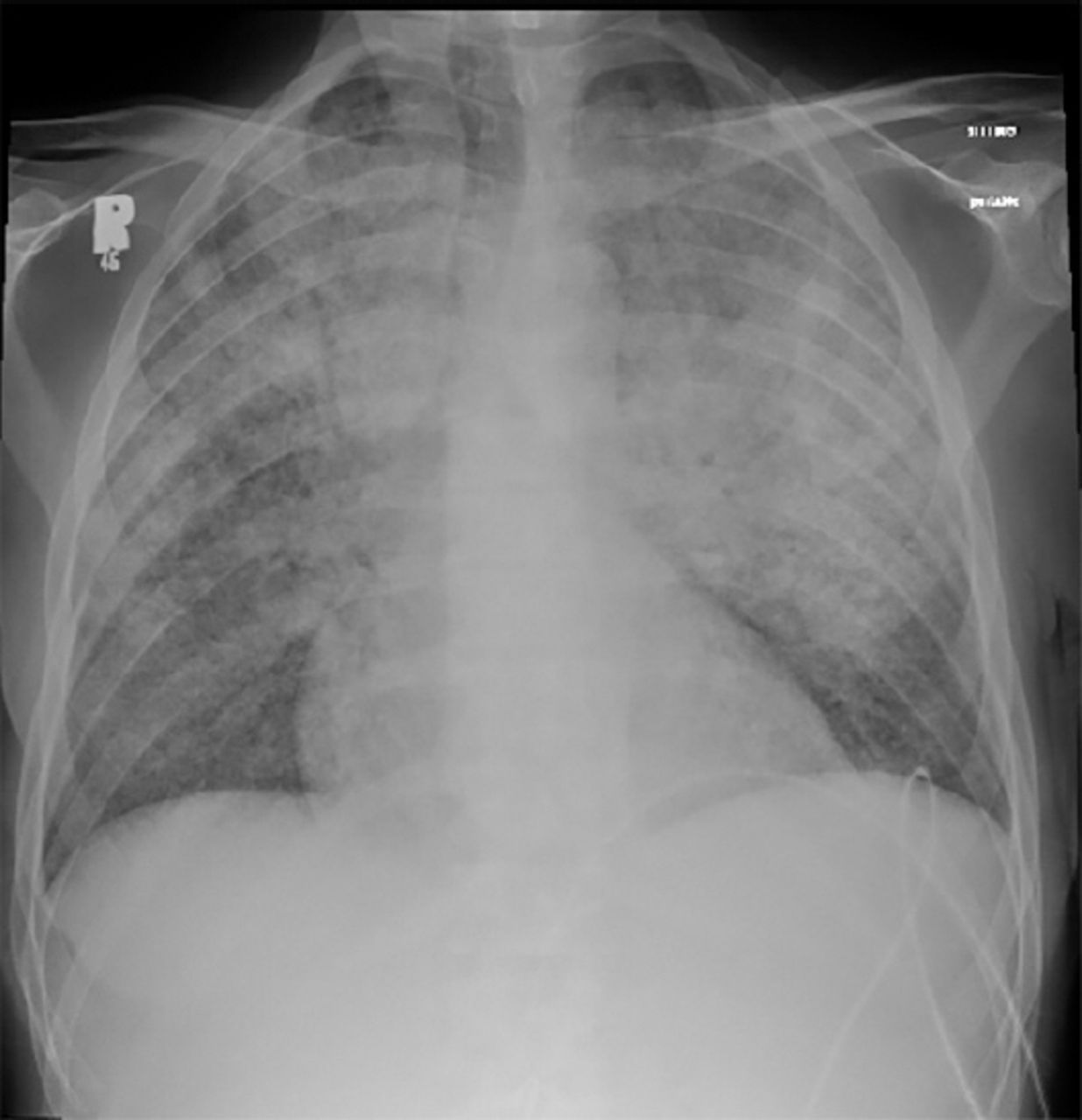
The characteristics of the patients who died are presented in Table 2. The cause of death was reported as septic shock in 3 patients, although a pathogenic organism was documented in only one case. High-frequency ventilation was used in 2 patients who ultimately died of progressive respiratory failure. Two patients died of sudden cardiac arrest despite their relatively stable respiratory status. No further explanation for cardiac arrest was documented. An example of Chest x-ray finding in Figure 1.
Demographics and presentation characteristics of the deceased patients.

Chest x-ray of a 46-year-old male with end stage renal disease who died at initial presentation.
Discussion
Mycobacterium TB is a relatively common etiological agent for CAP. Reports from Asia have shown that the incidence varies from 12% in Hong Kong to 21% in Singapore, whereas a study from the United States of America revealed an incidence of 5% in HIV-negative patients.13-15 The acute presentation of pulmonary TB is infrequently seen even in countries with a high prevalence of TB, and the literature is rare regarding the presentation of TB with ARDS at ICUs. The awareness of such presentation is crucial as the disease carries a high mortality risk and its early recognition and intervention are likely to have an impact on the outcomes. In 2 case series from Korea published in 2 separate studies, Park et al9 and Yon et al16 reported the clinical characteristics of a total of 70 patients with acute respiratory failure who required MV.9-16 Similar to our study, they reported high mortality rates of 60.5% and 59%. The presence of previously TB-destroyed lungs, AFB-smear positivity, low PaCO2 and high disease severity scores at the time of ICU admission (APACHE II ≥20) were independent risk factors for poor outcomes.9 In our study, high CURB-65 severity scores on admission, low PaCO2, and low PaO2/FiO2 ratios were associated with the worst outcomes. Although the median APACHE II scores of the survivors in our study were much lower than those of non-survivors, this difference did not have statistical significance. Although the median time from hospital admission to TB diagnosis and start of therapy were 5 days, there was an apparent association between the delay of TB treatment and mortality; as the median time from hospital admission to beginning of the therapy was 7 days in non-survivors versus 3 days in survivors, which is an important finding. However, due to the small number of patients and not all patients having received treatment, it will be hard to drive conclusions regarding the significance.
According to the Berlin definition of ARDS, diffuse alveolar damage (DAD) was the histological hallmark of ARDS, although it was not included as a diagnostic criterion of ARDS.17 In the last year, 5 studies18-22 have provided relevant information on ARDS and DAD relation, which in conclusion demonstrated that ARDS with DAD differs from the ARDS without DAD, and that DAD is associated with an increased risk of death than non-DAD ARDS. Interestingly, that was not studied before in TB patient with ARDS, and unfortunately, can not be demonstrated in our study whether the patients who died they have DAD in their pathology or not due to the lack of biopsy, but that would be an interesting theory to be tested regarding the pathogenesis of TB ARDS.
Predictors of MTB as the causative agent of CAP have been suggested in many studies. Cavallazzi et al23 evaluated 22 risk factors for pulmonary TB that were proposed by the Centers for Disease Control and Prevention in 6,976 hospitalized patients with CAP.23-26 Five risk factors were found to best predict CAP due to MTB: night sweats, hemoptysis, weight loss, MTB exposure, and upper lobe infiltration. Of these, only upper lobe involvement was frequently present in our sample population. However, such predictors might not have the same sensitivity and specificity in acute uncommon presentations.
In a retrospective study that extended over 7 years, Alshimemeri et al27 reported on 33 patients who were admitted to the ICU of our center and were diagnosed with active pulmonary TB. Twenty-two patients were treated for TB during hospitalization, whereas the other 11 were not diagnosed during hospitalization but were later found to be positive for MTB culture. Of the 22 patients treated for TB during hospitalization, 15 (68%) died. Of the 11 patients who were not diagnosed during hospitalization, 7 (64%) died. The authors stated that most of the patients required MV, but did not mention whether the patients’ symptoms met the ARDS criteria. The total number of cases of pulmonary TB represented 15% of CAP admitted to the ICU during that period. In our study, this percentage was much lower at 3% only. This may be explained by our restriction criteria of only patient with ARDs. However, the overall lower incidence of pulmonary TB cannot be excluded. An interesting finding was among the 9 positive cultures: 7 non-survivors and 2 survivors (all mycobacterium isolates were sensitive to all first-line therapy [isoniazid-rifampicin-ethambutol and pyrazinamide]).
Limitations
The aim of our study was mainly to describe this rare presentation of TB from our region. Unfortunately, we enrolled only 11 patients, and per that, we concluded statistical significant findings (factors predicting such a presentation or associated with mortality would be difficult).
In conclusion, patients with pulmonary TB infrequently present to intensive care with acute symptoms that meet all criteria for ARDS. Pulmonary TB should be considered early as a differential diagnosis by intensivists, especially in intermediate- and high-endemic regions. Empirical treatment should be considered early as this presentation of TB carries a high mortality risk.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received March 30, 2016.
- Accepted June 22, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}