


Abstract
Objectives: To investigate whether an inflammatory marker of neutrophil to lymphocyte ratio (NLR) predicts appropriate implantable cardioverter defibrillator (ICD) therapy (shock or anti tachycardia pacing) in idiopathic dilated cardiomyopathy (IDC) patients.
Methods: We retrospectively examined IDC patients (mean age: 58.3 ± 11.8 years, 81.5% male) with ICD who admitted to outpatient clinic for pacemaker control at 2 tertiary care hospitals in Ankara and Edirne, Turkey from January 2013-2015. All ICDs were implanted for primary prevention. Hematological and biochemical parameters were measured prior procedure.
Results: Over a median follow-up period of 43 months (Range 7-125), 68 (33.1%) patients experienced appropriate ICD therapy. The NLR was increased in patients that received appropriate therapy (4.39 ± 2.94 versus 2.96 ± 1.97, p<0.001). To identify independent risk factors for appropriate therapy, a multivariate linear regression model was conducted and age (β=0.163, p=0.013), fasting glucose (β=0.158, p=0.017), C-reactive protein (CRP) (β=0.289, p<0.001) and NLR (β=0.212, p<0.008) were found to be independent risk factors for appropriate ICD therapy.
Conclusions: Before ICD implantation by using NLR and CRP, arrhythmic episodes may be predictable and better antiarrhythmic medical therapy optimization may protect these IDC patients from unwanted events.
The implantable cardioverter defibrillator (ICD) is an important treatment option for selected high-risk patients to reduce sudden cardiac death. Recent studies revealed that ICD implantation reduces mortality in heart failure patients with reduced left ventricular function.1-4 A significant amount of these patients receive appropriate or inappropriate ICD therapies5,6 and it has been shown that shocks cause impaired quality of life, psychiatric disturbances, and increased mortality.5,7,8 Therefore, it is important to identify high arrhythmic risk patients before ICD in order to avoid unwanted negative events. Hematological parameters are used as predictive and prognostic markers for cardiovascular diseases9-11 and neutrophil to lymphocyte ratio (NLR) has become as a marker of underlying inflammation.12 Recent studies showed that NLR is a useful marker for predicting arrhythmic events.13-15 The aim of this study was to explore the association between NLR and appropriate ICD therapy [shock or anti tachycardia pacing (ATP)] in patients with idiopathic dilated cardiomyopathy (IDC) patients.
Methods
Study population
A total of 205 IDC patients (mean age: 58.3 ± 11.8 years, 81.5 % male) with ICD who referred to outpatient clinic for pacemaker control at 2 tertiary care hospitals in Edirne and Ankara, Turkey from January 2013-2015 were included in the study. The ICDs were implanted in Yuksek Ihtisas Hospital in Ankara, Turkey and Trakya University Hospital in Edirne, Turkey for primary prevention from 2003 to 2013 and the database of patients were reviewed retrospectively. The implanted devices were manufactured by Medtronic (Medtronic Inc., Minneapolis, MN, USA) and St. Jude (St. Jude Medical Inc. Sylmar, CA, USA) and all of them were single coil. idiopathic dilated cardiomyopathy patients were selected for ICD implantation for primary prevention when Left ventricle ejection fraction ≤35% and symptomatic heart failure (NYHA II-III) despite ≥3 months of treatment with optimal medical therapy.16 The patients with ischemic cardiomyopathy, atrial fibrillation-flutter, coronary arterial disease, primary valvular pathology, advanced chronic obstructive pulmonary disease, persistent biventricular cardiac pacemaker, recent infection, malignancy, blood dyscrasia, autoimmune or inflammatory disease, renal failure, hepatic failure, or current therapy with corticosteroids, and nonsteroidal anti-inflammatory drugs were excluded from the study.
Information, including age, gender, diabetes mellitus, hypertension, hyperlipidemia, and smoking status was gathered. Hypertension was defined as blood pressure >140/90 mm Hg on >2 occasions during office measurements or use of antihypertensive treatment. Diabetes mellitus was defined as fasting blood glucose >126 mg/dl or use of antidiabetics. Hyperlipidemia was considered to be present in patients with fasting total cholesterol ≥200 mg/dl or triglyceride ≥150 mg/dl. The study was in compliance with the principles outlined in the Declaration of Helsinki and was approved by the Institutional Ethics Committee.
Laboratory
Following a 12-hour fasting period, blood samples for the complete blood count analysis were collected before procedure in ethylenediamine- tetraacetic acideanticoagulated Monovette tubes (Sarstedt, Leicester, United Kingdom). Total and differential leukocyte counts were measured by an automated hematology analyzer (Abbott Cell-Dyn 3700; Abbott Laboratory, Abbott Park, Illinois, USA). Fasting blood glucose was analysed using the hexokinase method. Serum level of C-reactive protein (CRP) was measured by rate turbidimetry on the Beckman Coulter (California, USA).
Echocardiography
All echocardiographic examinations were performed by a certified cardiologist experienced in this field using a Vıvıd-7 (GE Vingmed, Horten, Norway) device in compliance with American Society of Echocardiography (ASE) guidelines.17 Left ventricular ejection fraction was measured by using modified Simpson’s rule on apical 4-chamber views.
Implantable cardioverter defibrillator Interrogation
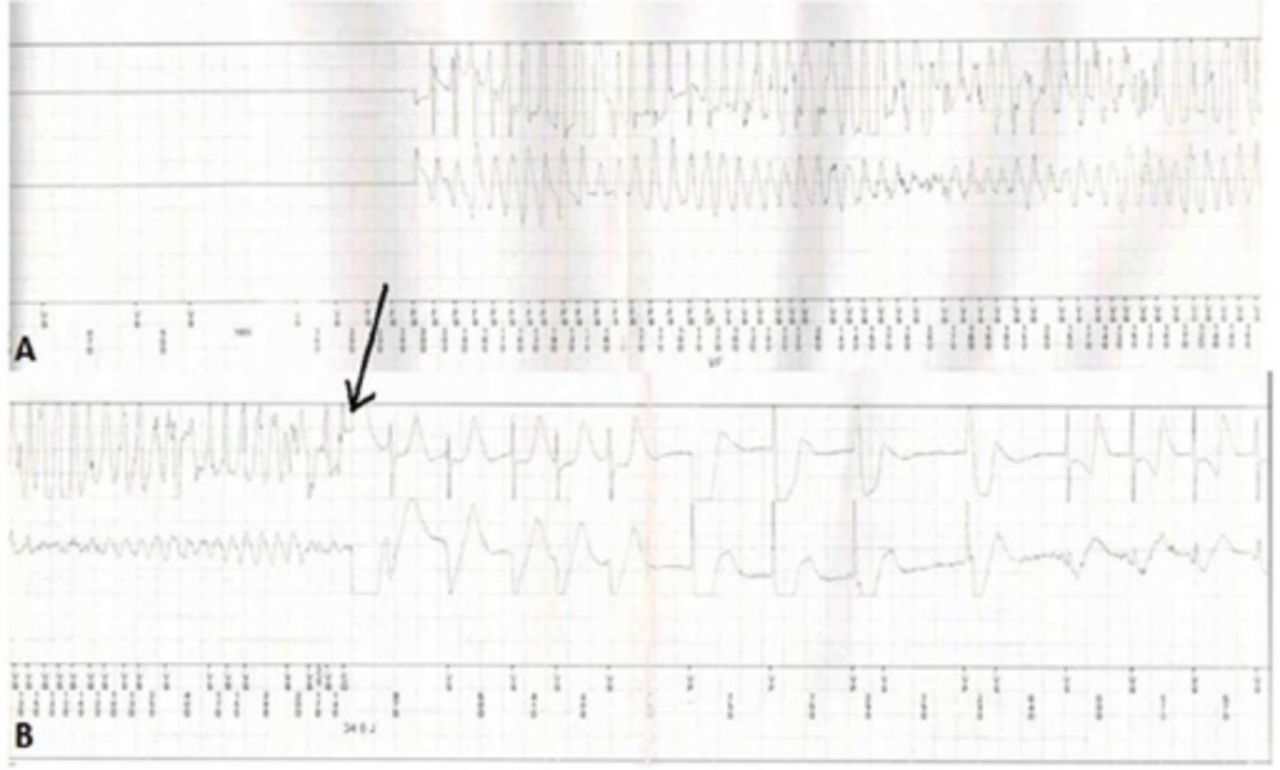
The end points for the study were appropriate ICD therapy (shock or ATP) due to ventricular tachyarrhythmia (Figure 1). Appropriate ICD therapy was defined as an antitachycardia pacing or shock therapy for ventricular tachycardia or fibrillation. All ICD’s zones were programmed as VT1 (167-182 bpm) with discriminators, VT2 (182-200 bpm) with discriminators, and VF (>200 bpm). The ICD programming included therapy for standard ventricular tachycardia (VT) with 3 antitachycardia bursts pacing therapy combined with low-energy shock and for ventricular fibrillation (VF) shock therapy with a 300-ms cut-off cycle interval. Standard VT was defined as sustained tachycardia with a cycle interval ranging 300 to 360 ms. The VF was defined as when the cycle interval was shorter than 300 ms.
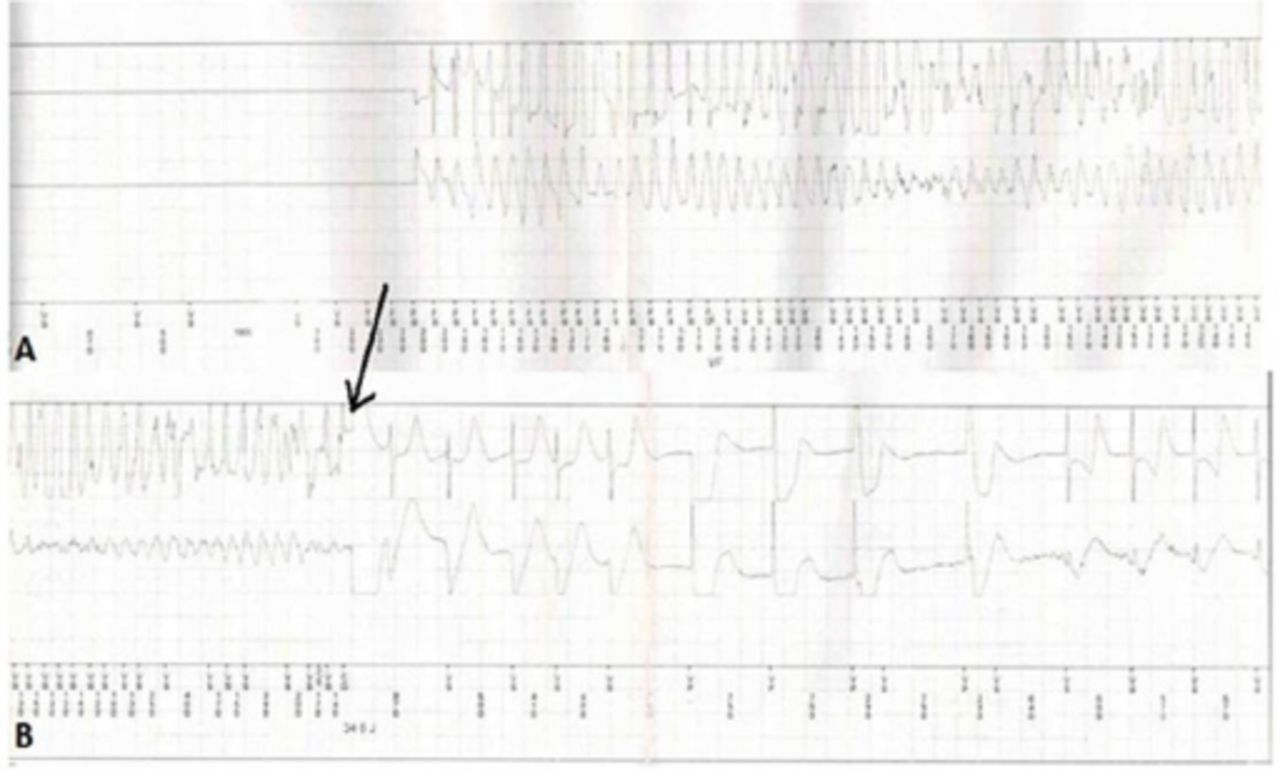
Appropriate implantable cardioverter defibrillator therapy of a study patient.
Implantable cardioverter defibrillator Data Storage and Retrieval
After ICD implantation the patients were followed up in our outpatient ICD clinic on 3 months intervals and when receiving high voltage therapy. The devices were interrogated at each controls and the complete set of data (including intracardiac electrograms) were recorded on USB flash memories and they were used in this study to retrieve all sustained arrhythmia episodes resulted in the ICD therapy. Two independent electrophysiologists Fatih Mehmet UCAR and Burak ACAR blinded to study design performed ICD interrogationsreviewed, and classified the arrhythmia episodes. In case of discrepancy in diagnosis the final analysis of the arrhythmia episode was made by a consensus of 3 electrophysiologists Fatih Mehmet UCAR, Burak ACAR and Serkan CAY After diasgnosis arrhythmic event time and the therapy mode were recorded.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation or as median with interquartile range; and categorical variables were expressed as number and percentages. A χ2 test or Fisher’s exact test was performed to compare the categorical variables. Student’s t-test or Mann- Whitney U test was used for continuous variables, as appropriate. One-way analysis of variance (ANOVA) test was used to compare 3 groups of functional class. Independent associations between appropriate ICD therapy and independent variables included were in the multivariate regression model as covariates. Coefficients of standardized β regression along with their significance from the multivariate regression analysis were also reported. The Pearson correlation test was used for correlation analysis. Receiver operating curve (ROC) analysis was used to calculate the required NLR cut-off values to to detect appropriate ICD therapy (shock or ATP) with maximum sensitivity and specificity. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL, USA) version 17. A p-value of less than 0.05 was considered statistically significant.
Results
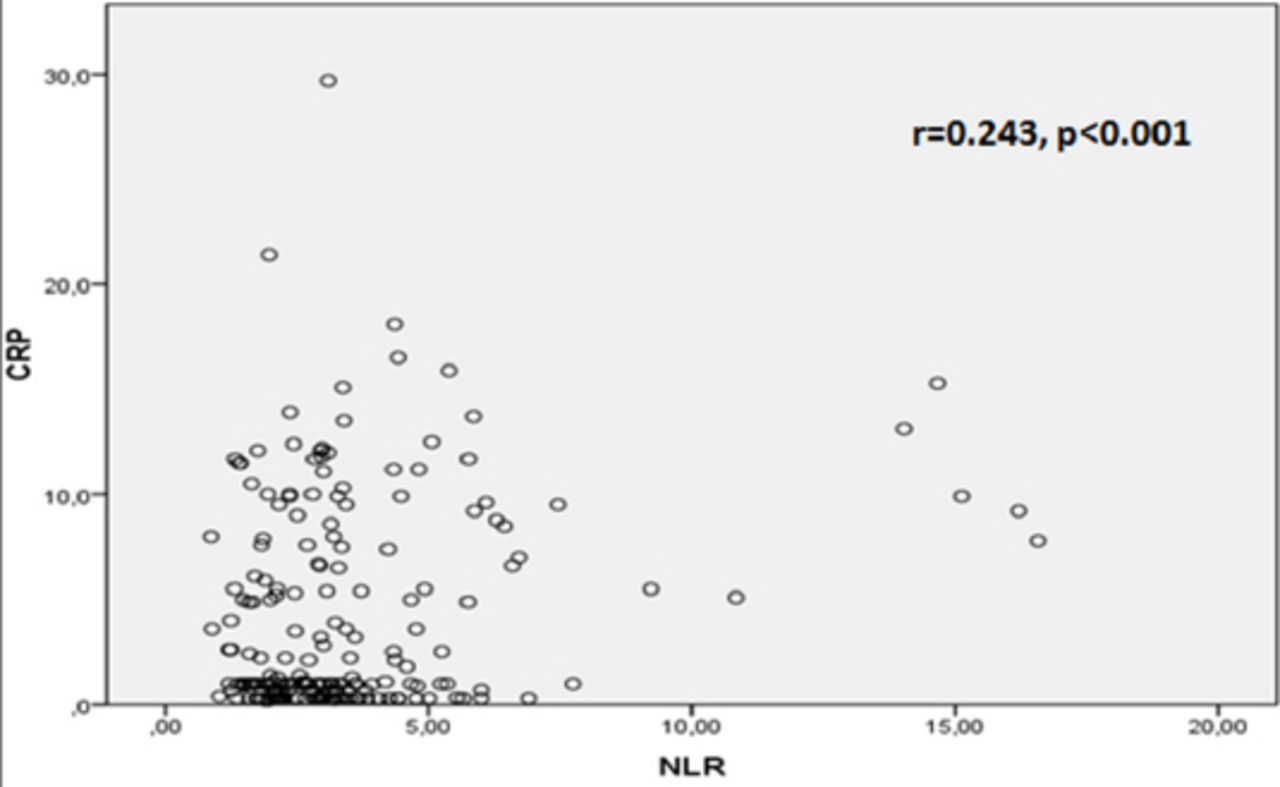
Over a median follow-up period of 43 months (range 7-125), appropriate ICD therapies were observed in 68 (33,1%) of 205 IDC patients [shock 38 (55.9%) was patients, ATP 30 (44.1) patients]. The study population divided into 2 groups due to the presence of appropriate ICD therapy (control group: 137 patients and therapy group: 68 patients). The baseline characteristics of the study population are shown in Table 1. Baseline characteristics were similar between groups. The results of the hematological and biochemical parameters are listed in Table 2. The NLR levels were higher in the therapy group patients (4.39 ± 2.94) compared with the control group (2.96 ± 1.97) (p<0.001). Additionally the CRP in therapy group patients was (11.0 ± 7.9) and in control group (4.4 ± 4.6) (p<0.001), and the neutrophil in the therapy group patients was (6.0 ± 2.1) and in the control group (5.3 ± 1.7) (p=0.01) levels were higher in therapy group when compared control group. To identify in dependent risk factors for ICD therapy, a multivariate linear regression model was conducted that included the following covariates: age, amiodarone use, glucose, creatinine, neutrophil, CRP, and NLR. Age (β=0.163, p=0.013), glucose (β=0.158, p=0.017), CRP (β=0.289, p<0.001) and NLR (β=0.212, p<0.008) levels were found to be independent risk factors for appropriate ICD therapy. Pre-procedural NLR were found to correlate with CRP values (r=0.243, p<0.001) (Figure 2)
Baseline characteristics of the patients.
Comparison of patients with implantable cardioverter defibrillator (ICD) therapy and control individuals in terms of biochemical and hematological characteristics.

Correlations between neutrophil to lymphocyte ratio and C-reactive protein levels (CPR), Neutrophil to lymphocyte ratio (NLR)
Receiver operating characteristic curves were used to explore the relation between preprocedural ICD implantation NLR and appropriate ICD therapy. The area under the curve was 0.707 (95% Confidence interval: 0.629 to 0.785, p<0.001). Using a cutoff level of 2.93, the preprocedural NLR predicted appropriate ICD therapy with a sensitivity of 71% and specificity of 62% (Figure 3).

Receiver operating curve (ROC) analysis between preprocedural implantable cardioverter defibrillator (ICD) implantation neutrophil to lymphocyte ratio values and appropriate ICD therapy. CI: Confidence interval
Discussion
In our study, we investigate whether NLR in IDC patients with primarily implanted ICD is a predictor of appropriate therapy (shock or ATP). In the average follow up of 43 months (7-125) we found that there is a strong association with appropriate therapy and NLR. However, the number of lymphocytes and neutrophil and CRP levels also showed a strong relationship with the appropriate ICD therapy. Effectiveness of the ICD therapy is assessed by identifying life-threatening rhythm disorders and treating it appropriately. Although ICD has mortality reduction effect, it can cause various complications. Inappropriate shocks are associated with high mortality and morbidity.5 However, inappropriate shocks cause impaired quality of life, psychiatric disturbances, and increased mortality. So the implantation of ICD to eligible patients is very important.
The IDC is an inflammatory disease with many circulating active cytokines being involved in the pathogenesis. Although the mechanisms responsible for the development of IDC are not fully understood, high production of inflammatory cytokines in leukocytes of patients with IDC and the presence of interleukin-6 (IL-6) and tumour necrosis factor alpha (TNF-α) in the cardiac tissue suggest an inflammatory component in the disease development and progression.18 The relationship between inflammation and mortality is well known in heart failure patients.11 The effects of inflammation and neurohormonal activation in cardiovascular diseases and strong relationship in heart failure and atherosclerosis has been demonstrated in studies. These studies have demonstrated that these mediators are predictors of atrial and ventricular arrhythmias.19,20 Serum collagen turn over markers were shown a predictor of appropriate shock in primarily implanted ICD with IDC patients. These markers are associated with ventricular remodeling and electrical activity of ventricle.21 Another study showed that BNP and nt-BNP levels before ICD implantation are associated with appropriate ICD shocks and BNP may serve as a marker of mechanoelectrical feedback in cardiomyocytes under certain conditions.22 Inflammation is a controversial factor of appropriate ICD shocks. While some previous studies emphasized that IL-6 and CRP are appropriate ICD shock predictors,23,24 others have not.25 In a study by Cheng et al,26 it is observed that appropriate ICD shock rates increased with high IL-6 levels. However, CRP, IL-6, TNF-a, pro-BNP showed a linear progression of the increase of mortality in ICD patients and a scoring system, which created with the combined use of these markers has been shown to be a strong predictor for appropriate ICD shocks and mortality. Inflammatory response play a key role in the pathophysiology of many vascular disorders of both heart and brain.27,28 Neutrophil infiltration in the atherosclerotic plaques allows prediction of the risk of plaque rupture29,30 and activated neutrophils lead to plaque rupture through the effects of various proteolytic enzymes and myeloperoxidase-like oxidants.31,32 Lymphocytopenia is a common finding during the stress response secondary to increased corticosteroids levels.33 In recent years, an index which reflects both neutrophils in acute inflammation that reflects the height of the situation and lymphopenia after acute physiological stress has been used. This index obtained by the ratio of neutrophils and lymphocytes, was used with other inflammatory markers in studies and has been determined as a good indicator of inflammation.14
Previous studies34,35 demonstrated the relationship between NLR and functional capacity and the severity of the disease in IDC patients34,35. And it has been revealed that NLR is a good marker for predicting atrial and ventricular arrhythmias13,15,36. The ICD implantation to IDC patients for primary prophylaxis is controversial. In a Danish Study,37 it was observed that incidence of all-cause mortality was similar in the ICD group versus control group, and younger patients (<59 years) appeared to derive greater benefit from the ICD implantation versus older patients. In the present study, patients’ average age was 58.3 and it can be said that they were young. We found a significant relationship between increased NLR and appropriate therapy in IDC patients before ICD implantation. Additionally, CRP levels were high similar to NLR. Therefore, our findings may be beneficial for the selection of IDC patients for primary prevention ICD implantation.
The study was single-centered and included limited number of patients. Due to the sample size and inadequate power, it is possible that some associations were not detected. Other inflammatory parameters such as IL-6 or TNF-α were not measured. Ischemic cardiomyopahy patients were not involved to study. Further prospective studies are needed to confirm the prognostic role of inflammatory markers for appropriate shock in IDC patients with ICD.
In conclusion, NLR predicts arrhythmic events and appropriate ICD therapy in IDC patients with primary prophylaxis implanted ICD. Our results suggest that NLR and CRP may be used as biomarkers for arrhythmic risk stratification and medical therapy optimization should be carried out better especially in high risk patients.
Acknowledgment
The authors gratefully acknowledge Dr. Serkan Cay, Turkiye Yuksek Ihtisas Training and Research Hospital, Ankara, Turkey for his help in diagnosis the final analysis of the arrhythmia episodes.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received August 28, 2016.
- Accepted November 16, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.