


Abstract
Objectives: To determine the 2-year outcome of acute kidney injury (AKI) following admission to pediatric critical care units (PICU).
Methods: A retrospective cohort study was conducted between January 2012 and December 2013. We followed 131 children admitted to PICU, King Abdulaziz University Hospital, Jeddah, Kingdom of Saudi Arabia with a diagnosis of AKI, based on pRIFLE (pediatric risk, injury, failure, loss, and end-stage renal disease), for 2 years. During the study period, 46 children died and 38 of survivors completed the follow-up. Factors affecting long-term progression to chronic kidney disease were also evaluated.
Results: The 2-year mortality was more than 40%. The main determinant of the 2-year mortality was the pediatric risk of mortality (PRISM) score, which increased the risk of mortality by 6% per each one score (adjusted odds ratio, 1.06: 95% confidence interval: 1.00-1.11). By the end of the 2 years, 33% of survivors had reduction in the glomerular filtration rate and proteinuria, and 73% were hypertensive. Patients with more severe renal impairment at admission, based on the pRIFLE criteria, had higher mortality rate. This association, however, was not independent since it was influenced by baseline disease severity (PRISM score).
Conclusion: Large proportion of patients admitted to PICU with AKI either died during the first 2 months of follow-up or developed long-term complications. The severity of AKI, however, was not an independent risk factor for mortality.
Acute kidney injury (AKI) is common in critically ill children admitted to pediatric intensive care units (PICU), and is associated with a significant increase in mortality.1 Furthermore, significant percentage (approximately 10%) of them develops chronic kidney disease (CKD).2 The estimated risk of mortality and morbidity among critically ill children admitted with AKI is variable across different studies, and factors influencing such variation are yet to be determined. In adults, studies showed that the severity of underlying CKD rather than AKI predicts medium- to long-term mortality.3,4 Acute kidney injury in children, however, has been reported to be associated with increased risk of CKD and mortality.5 Factors that have been found to increase the risk of CKD progression are acute on chronic kidney disease6 and the need for dialysis post AKI, which was reported to increase the risk of progression to end-stage renal failure in 5 years follow-up.7 In this study, we evaluated the long-term outcome of critically ill children admitted to the PICU with AKI, defined by pediatric risk, injury, failure, loss, and end-stage renal disease (pRIFLE) classification scheme.8 We also evaluated the risk factors for developing CKD among those children. We looked into the risk of CKD in children with AKI stratified according to the pRIFLE classification in order to answer the question: Do all AKI children need long term follow up?
Methods
We designed a retrospective cohort study to evaluate all children who were admitted to PICU with a diagnosis of AKI, based on pRIFLE criteria, at King Abdulaziz University (KAU), Jeddah, Kingdom of Saudi Arabia (KSA) during the period from January 2012 to December 2013. We included all children fulfilling the following criteria: 14 years of age or younger, admitted to PICU with AKI based on pRIFLE criteria, and their data regarding the exact duration of follow-up and the outcome (death) during their follow-up were determined. The pRIFLE staging was carried out according the most severe stage of AKI reached during PICU admission using enzymatic serum creatinine and urine output criteria. Children with evidence of CKD stage 3 or more were excluded. Data, which were collected from medical records, included patients’ demographic characteristics at presentation, length of stay in PICU and regular ward, requirement of mechanical ventilation, requirement of renal replacement therapy, baseline creatinine, baseline glomerular filtration rate (GFR), blood pressure, proteinuria, and results of renal ultrasound studies. Baseline creatinine was defined as the last creatinine within the previous 6 months prior to PICU admission. For patients without baseline creatinine data, average normal creatinine values (based on age and gender) were used. We have calculated the pediatric risk of mortality (PRISM) score for all children.9
Data regarding blood pressure, creatinine, GFR, and proteinuria were collected after 3, 6, 12, 18, and 24 months after hospital discharge. The GFR was calculated using the Schwartz formula.10 Hypertension was defined as blood pressure between 95th and 99th percentile for age and height.11 Proteinuria was defined as early morning urine protein level of 30 mg/dl or more.12 Reduction in the GFR was defined by change in GFR by at least one stage based on CKD staging.
The related studies, which have been used within and throughout our study discussion were obtained from a variety of reliable online databases, such as PubMed and WebMD. Permission to conduct the study was granted by the Biomedical Ethics Research Committee of Faculty of Medicine at KAU, KSA. Obtaining consents from participant was waived as it is retrospective study using anonymous subjects. The study was conducted according to the principles of Helsinki Declaration.
Statistical analysis
All analyses were performed using STATA (StataCorp. 2011. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP) software. The proportion and mean for dichotomous and continuous variables were measured to describe patients’ characteristics. The 2-year survival among patients who required admission to PICU with AKI was estimated using the Kaplan-Meier Curve. The impact of AKI on the 2-year mortality was estimated using the Cox proportional-hazards regression model. Multivariate regression analysis was performed to control for potential confounding factors including baseline age, gender, BMI, proteinuria, hypertension, and PRISM. All patients with determined follow-up duration, including censored patients, were included in the survival analysis. Long-term outcomes among patients who survived after acute AKI were estimated (proportion and 95% confidence intervals [CI]) at 3, 6, 12, 18, and 24 months post admission to PICU. Statistical significance was determined using the 95% CI and p-value of 0.05.
Results
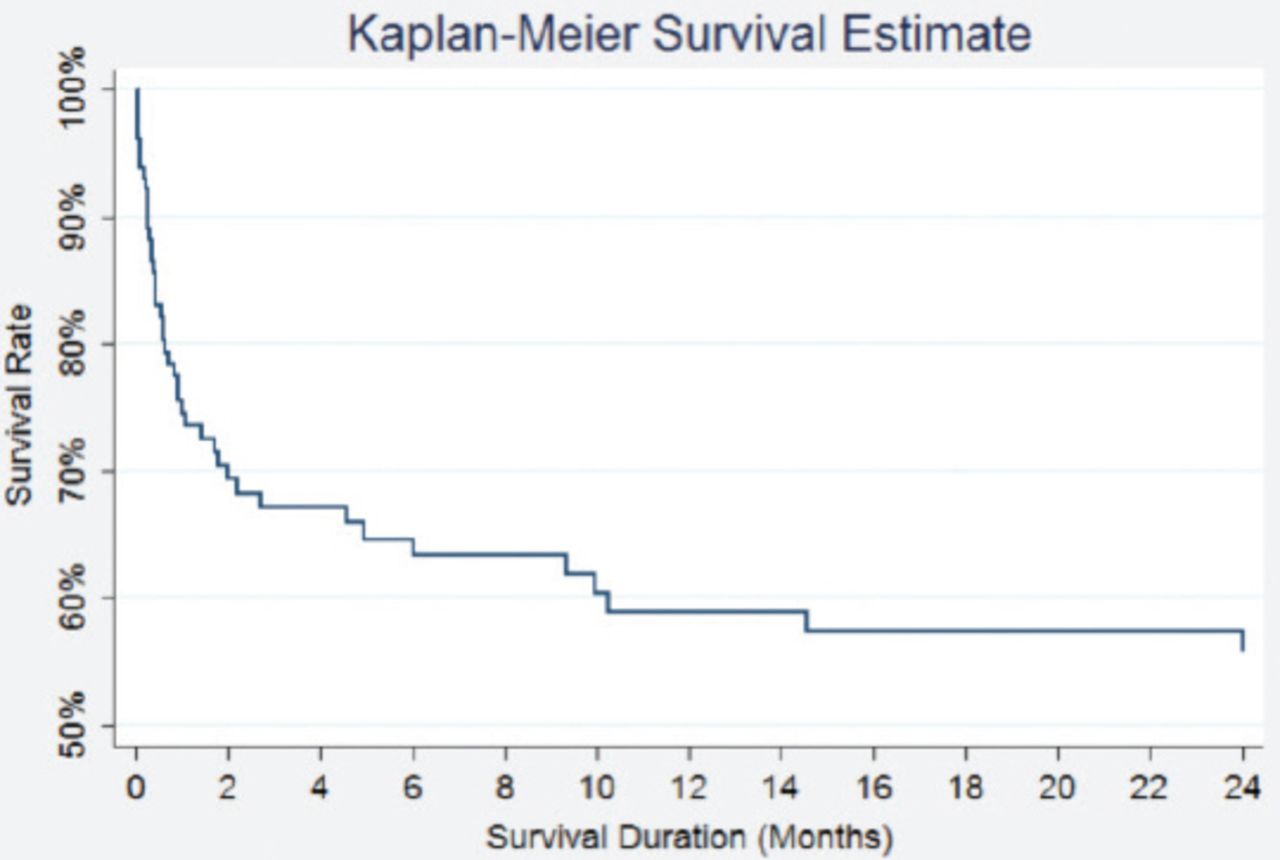
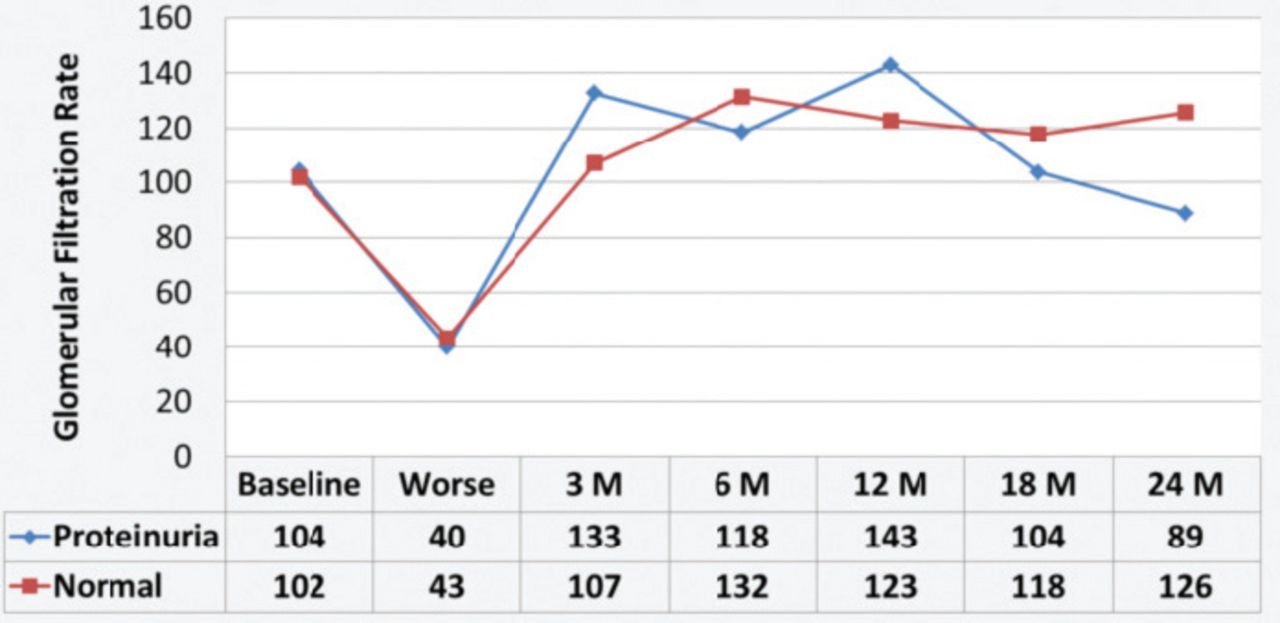
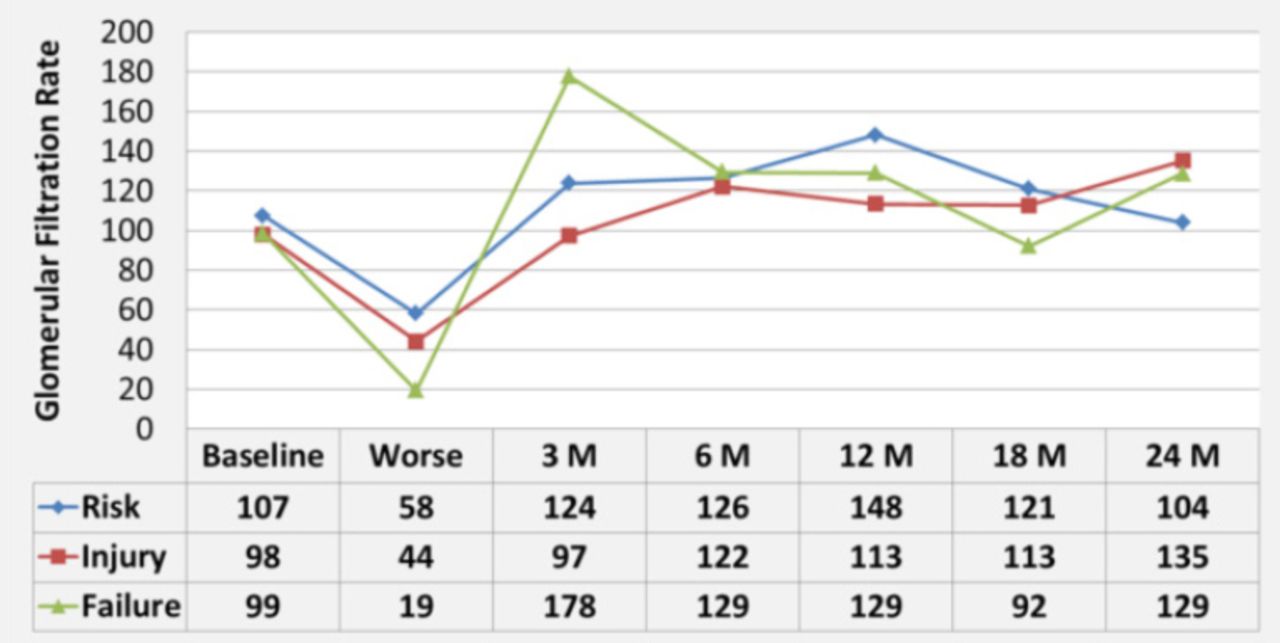
Of the 131 children included in the study, 46 died during the follow-up period. Among the survivors, 38 subjects completed the 2 years follow-up. Baseline demographic and disease characteristics are shown in Table 1. The 2-year mortality among children admitted to PICU with AKI was more than 40%, most of which was during the first 2 months of follow-up (Figure 1). In hospital mortality was 28% (95% CI: 21-37%). The AKI severity, based on pRIFLE criteria (comparing failure to risk stages), had a significant association with the 2-year mortality (crude odds ratio [OR]: 2.6; 95% CI: 1.29-5.36). However, after adjusting for potential confounding factors this association became insignificant, as it was confounded by the baseline characteristics (Adjusted OR: 2.3; 95% CI: 0.79-6.54) (Figure 2 &Table 2). PRISM score, on the other hand, increased significantly the risk of mortality by 6% per each one score (adjusted OR: 1.06; 95% CI: 1.00-1.11). At one-year follow-up, 64% (95% CI: 47-79%) of survivors had normal GFR, 2.5% (95% CI: 0.1-14%) had stage 1 CKD, 26% (95% CI: 13-42%) had stage 2 CKD, 5% (95% CI: 1-17%) had Stage 3 CKD, and 2.5% (95% CI: 0.1-14%) had stage 4 CKD. At the end of 2-year follow-up, 73% (95% CI: 52-88%) of survivors developed hypertension, 33% (95% CI: 15-57%) developed proteinuria, and 33% (95% CI: 17-54%) developed renal impairment. However, the severity of renal impairment and proteinuria at baseline did not significantly influence the risk of long-term renal impairment (Figures 3 & 4).
Baseline patients’ demographic and disease characteristics.
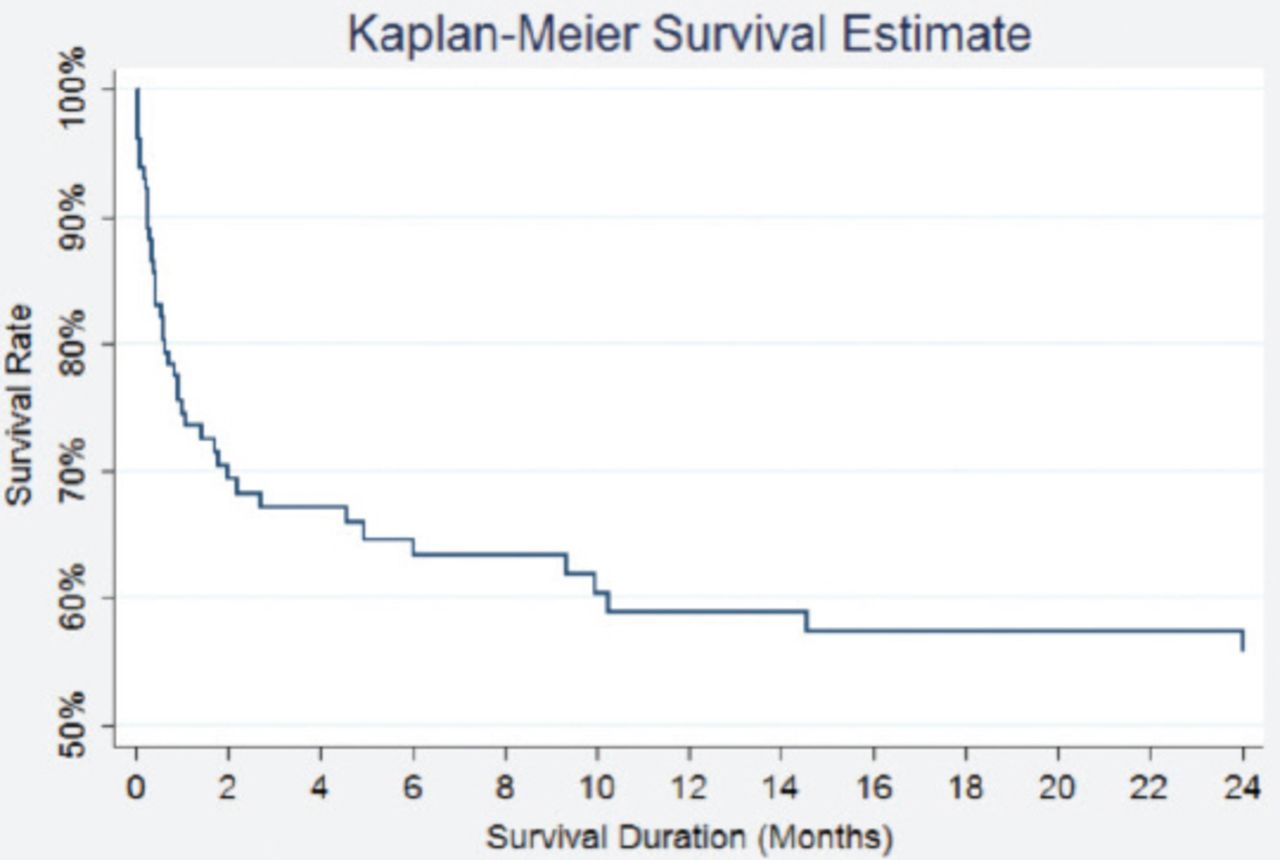
Kaplan-Meier curve showing survival rate among patients admitted to pediatric intensive care unit with renal impairment
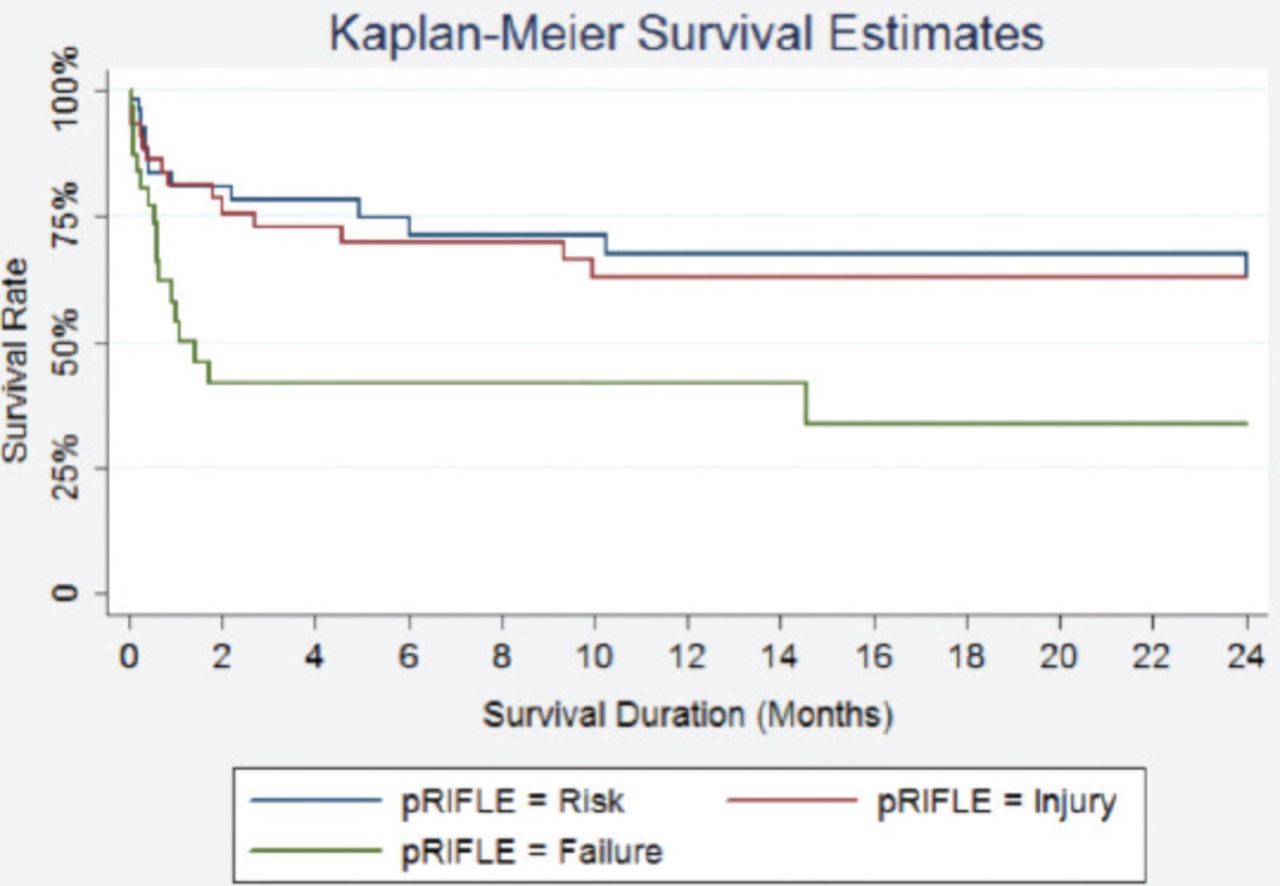
Kaplan-meier curve showing survival rate among patients admitted to pediatric intensive care unit stratified by the extent of renal impairment, based on pediatric risk, injury, failure, loss, and end-stage renal disease (pRIFLE).
Hazard ratio of death among patients admitted to pediatric intensive care unit with different characteristic features.
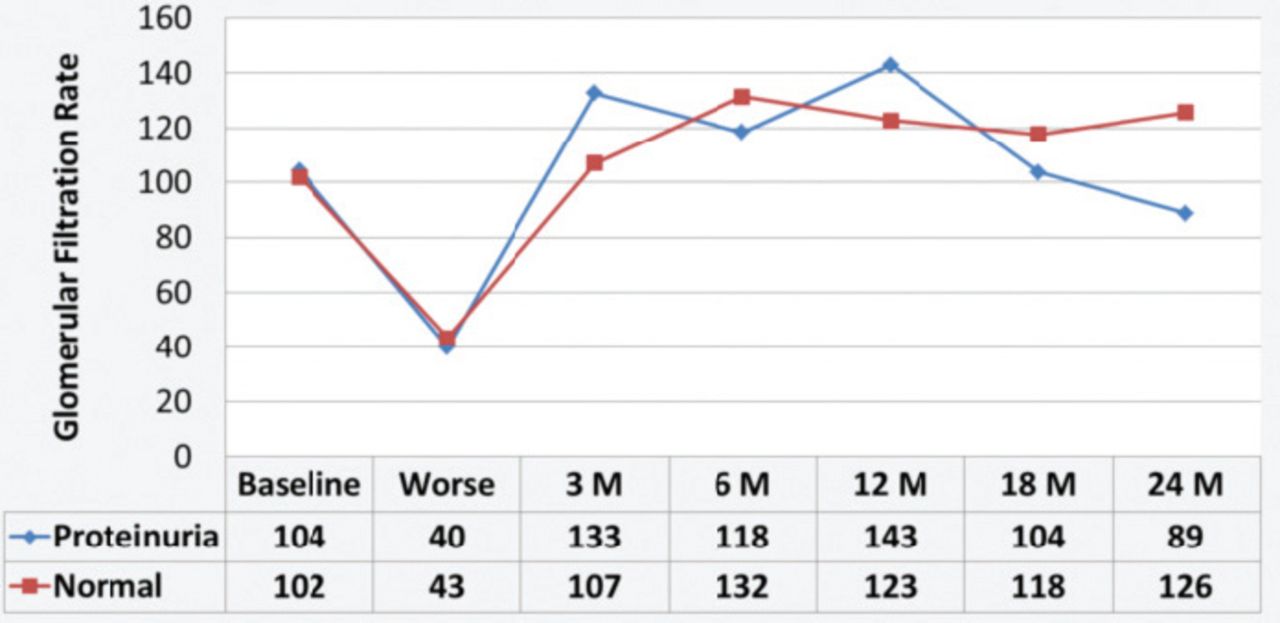
Glomerular filtration rate level during 2 years follow-up among patients with normal versus high (30 mg/dl or more) urine protein level at baseline.
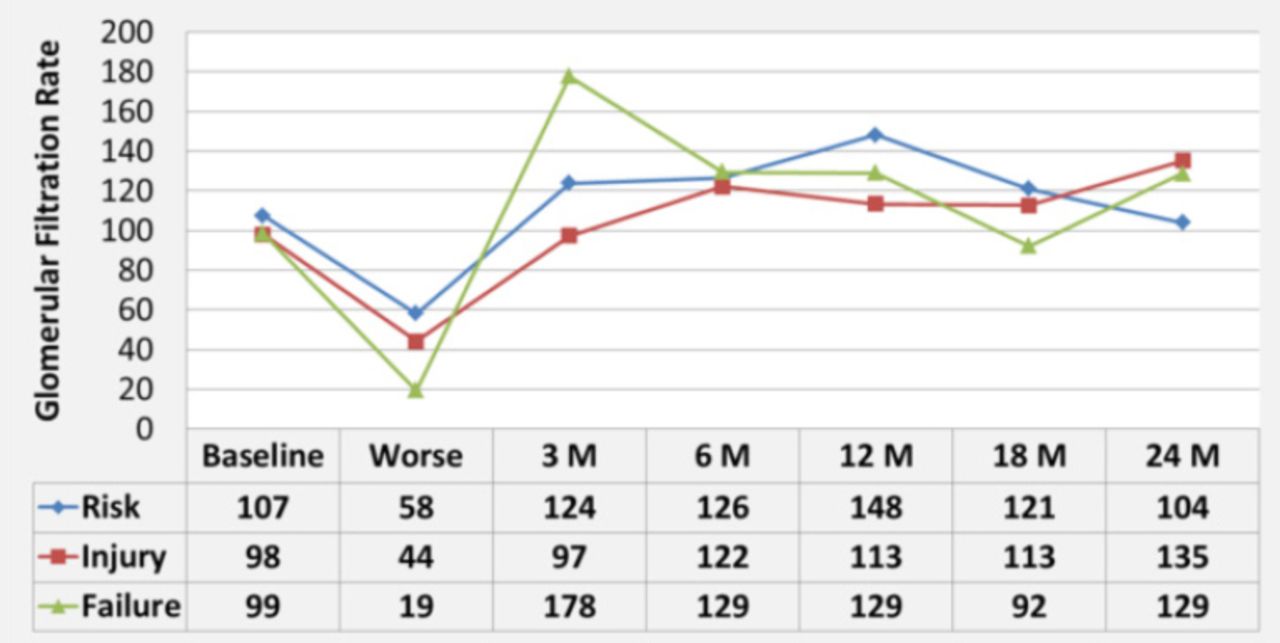
Glomerular filtration rate level during 2 years follow-up after admission to pediatric intensive care unit, stratified by the modified pediatric risk, injury, failure, loss, and end-stage renal disease criteria at the time of admission.
Discussion
We have observed high mortality rate, particularly in the first 2 months after AKI episode and with increasing PRISM score in children admitted to the PICU. The high initial mortality rate is similar to a report from Hong Kong with mortality rate of 41% in children with AKI during PICU admission compared with 8% of those without AKI.13 However, the authors in this study did not follow the children after discharge from the PICU. High mortality rate (47%) was also reported in adults with AKI (RIFLE stage failure) who required renal replacement therapy with mortality at one (65%), 5 (75%), and 10 years (80%) following the episode of AKI.4 Furthermore, CKD developed in considerable percentage of survivors.4 Similarly, a Swedish multi-center study5 found increase in short- and long-term risk of death and progression to CKD among adults admitted to the intensive care unit with AKI.5 Other studies, on the other hand, reported lower mortality (15.5%) among children admitted to PICU with AKI.14
In our study, patients with higher pRIFLE score had increased risk of the 2-year mortality. This association, however, became insignificant after adjusting for potential confounding factors. Previous studies showed that the risk of mortality is in association with AKI as well as RIFLE class (5.1% for risk, 16.2% for injury, and 29.6% for failure stages).14 Consistent with our study, this association disappeared after adjusting for confounding factors in multivariate analysis.14 Naik et al14 found that the need for mechanical ventilation and the number of failed organs, but not the presence of AKI, were the factors that independently influenced mortality. In our study, PRISM score was the factor that was independently associated with mortality. These findings indicate that AKI and its severity are not independent risk factors for mortality, and other factors related to underlying disease severity influenced mortality among patients admitted to PICU with AKI.
At the end of the 2 years, in our cohort, considerable percentage of children developed CKD with evidence of proteinuria, hypertension, or reduction in GFR. This is similar to recent reports from both adult and pediatric studies.2-7,15 The percentage of children with worsening GFR in our study is much higher when compared with what has been published in a recent meta-analysis of 10 cohort studies with 346 children included (33.4 % versus 6.3%). We also observed higher percentage of proteinuria (33.3% versus 3.1) and hypertension (73.3% versus 1.4).15 This could be explained by the difference in severity, the underlying etiology of AKI and the presence of associated factors as chronic illness. The severity of renal impairment and proteinuria at baseline did not significantly influence the risk of long-term renal impairment. The small number of survivors who completed the follow-up, however, limits the power to confidently extract conclusion from these findings; therefore, larger multicenter studies are required.
We have several limitations, including the fact that the recruitment was confined to a single center and the retrospective nature of the study, which limited our access to follow-up data for some patients. Although the number of included subjects for survival analysis was reasonable, it was small for measuring other long-term outcomes among survivors.
In conclusion, children with AKI had high mortality in our population, particularly in early months after admission to PICU. Considerable proportion of survivors developed hypertension, proteinuria, and renal impairment after 2 years of follow-up. Children with more severe AKI at admission to PICU had higher 2-year mortality rate. This association, however, was not independent since it was influenced by baseline PRISM score. Impact of AKI severity on other long-term outcomes among survivors requires further multicenter studies.
Footnotes
Disclosure. Authors have no conflict of interest and the work was not supported or funded by any drug company. This project was funded by King Abdulaziz City for Science and Technology, Riyadh, Kingdom of Saudi Arabia (Grand number 27-35 -T-A).
- Received July 28, 2016.
- Accepted November 16, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.