


Abstract
Objectives: To compare clinical, anthropometric, and laboratory characteristics in diabetes type 2 patients of 2 genetically-distinct ethnicities living in Jordan, Arabs and Circassians/Chechens.
Methods: This cross sectional ethnic comparison study was conducted in King Abdullah University Hospital, Irbid and The National Center for Diabetes, Endocrinology, and Genetics, Amman, Jordan between June 2013 and February 2014. A sample of 347 (237 Arab and 110 Circassian/Chechen) people living with diabetes were included in the study. Data were collected through direct interviews with the participants. Clinical data were collected using a questionnaire and anthropometric measurements. Laboratory data were extracted from the patients’ medical records.
Results: More Arabs with diabetes had hypertension as a comorbidity than Circassians/Chechens with diabetes. Arabs living with diabetes were generally more obese, whereas Circassians/Chechens living with diabetes had worse lipid control. Arabs with diabetes had higher means of glycated haemoglobin (HbA1c) and fasting blood sugar, and more Arabs with diabetes had unsatisfactory glycemic control (60.6%) than Circassians/Chechens with diabetes (38.2%) (HbA1c ≥7.0%). Most participants (88.8%) had at least one lipid abnormality (dyslipidemia).
Conclusion: Multiple discrepancies among the 2 ethnic diabetic populations were found. New diabetes management recommendations and policies should be used when treating people living with diabetes of those ethnicities, particularly in areas of glycemic control, lipid control, and obesity.
Type 2 diabetes mellitus (DM) is a chronic systemic metabolic disorder characterized by high blood glucose, caused by defective insulin secretion from the pancreas and/or altered insulin function in cells around the body. These cellular changes are caused by both genetic and environmental factors making the pathogenesis, of the disease complex.1 As a systemic disease, DM encompasses many short-term and long-term complications caused by chronic hyperglycemia, including the risk of cardiovascular, cerebrovascular, ophthalmic, renal, and neurologic disease, along with acute life-threatening conditions. These complications negatively affect the quality and duration of the individual’s life, and pose a huge burden on the patient, their families, and the health system as a whole.2 Worldwide, DM is an increasing problem reaching epidemic proportions.3 The International Diabetes Federation (IDF) estimated the number of affected individuals in 2012 to be more than 371 million.4 Arab countries are also affected by this surge. Studies demonstrate increasing prevalence of DM in Middle Eastern and North African Arab countries.5 In 2012, the IDF reported a DM prevalence of 9.1% in the Middle East and North Africa.4 In Jordan, the prevalence of type 2 DM is on the rise; data show an increase from 13% in 1994 to 17.1% in 2008.6,7 These worrisome results solidify DM status as a burden on an already strained health system in the Middle-Eastern country. Studies show that in addition to the variation of DM prevalence among different countries resulting in a unique geographic distribution, DM prevalence varies among different ethnic groups and subpopulations within the same country.8 This reflects the role of ethnicity in developing and treating DM. Studying ethnically and genetically isolated diabetic populations sharing the same environment could be of high yield in the search of unanswered questions regarding the factors contributing to the development of DM. Furthermore, such studies could guide new management policies and recommendations for DM patients of the studied ethnicity. The Jordanian population consists of multiple ethnic constituents; most Jordanians are of Arab ethnicity and descent. Two other culturally and demographically important ethnicities in Jordan are Circassians who originally from Caucasus and Chechens originally from Chechnya. These 2 populations are sharing the same environmental factors, dietary habits, and lifestyle with the Jordanians of Arab ethnicity and are ethnically and genetically isolated, mainly due to the endogamous marriages and preservation of traditions and language.9,10 Dajani et al11 studied the prevalence of DM, clinical characteristics, and glycemic control of these 2 populations, and reported a DM prevalence of 9.6% in Circassians and 10.1% in Chechens. This discrepancy with the results of previous analyses on the Jordanian population raises the possibility of a different pathogenic process and etiologic factors in those different ethnicities sharing the same environment in Jordan. A previous study12 compared the prevalence of metabolic syndrome and its components between the Circassian/Chechen population living in Jordan with the Arab population living there, and reported multiple differences. The objective of this study is to compare the demographic details, clinical characteristics, and laboratory parameters between a genetically-isolated combined Circassian/Chechen diabetic population, and an Arab diabetic population, both sharing the same environment in Jordan. Differences among the 2 groups could be used to guide public health programs and treatment policies that account for such differences. They would also pave the way for a genome wide association study to discover the genetic factors responsible for these differences, and therefore novel genetic factors in the pathogenesis and management of type 2 DM.
Methods
Study population and data collection
A comparative study between diabetes patients of Arab descent and diabetes patients of Circassian/Chechen descent was conducted. Ethical approval to carry out the study was granted by the Ethics Committee of Jordan University of Science and Technology, Irbid, Jordan and all procedures followed were in accordance with the 1964 Declaration of Helsinki. All participants signed a written informed consent to the study. Data were collected in the period from 2013 to 2014 through direct interviews with the participants at King Abdullah University Hospital in Irbid, and at The National Center for Diabetes, Endocrinology, and Genetics in Amman, Jordan. Six hundred DM type 2 patients were approached to participate in the study. Of those, 347 fulfilled the inclusion criteria mentioned previously and consented to be included in the study as seen in Figure 1. The sample consisted of 237 (68.3%) participants of Arab ethnicity, and 110 (31.7%) of Circassian and Chechen ethnicity and descent. Ethnicity and pedigree information of the previous 3 generations was analyzed in the Circassian, Chechen, and Arab populations to verify their ethnicity and origin. Inclusion criteria included: diagnosis with type 2 DM more than 6 months prior to data collection, confirmed ethnicity (Circassian, Chechen, or Arab) in the last 3 generations using pedigree information, living in Jordan, age >30 years old, and age of diagnosis >18 years old. Patients with type 1 DM were excluded from the study. Circassian and Chechen subjects were combined into one group as analysis showed no significant demographic, clinical, or laboratory differences between them. Information was obtained using a questionnaire designed for the study. The questionnaire consisted of 3 parts. The first part focused on social-demographic details, including gender, age, marital status, and level of education. The second part included questions regarding the patients’ lifestyle; including regular exercise, a healthy dietary plan (reduced sugar, salt, and fat intake), and smoking history. The third part explored the patients’ clinical characteristics, including a family history of type 2 DM and hypertension and the presence of comorbidities, specifically asking regarding hypertension, coronary artery disease, and dyslipidemia.
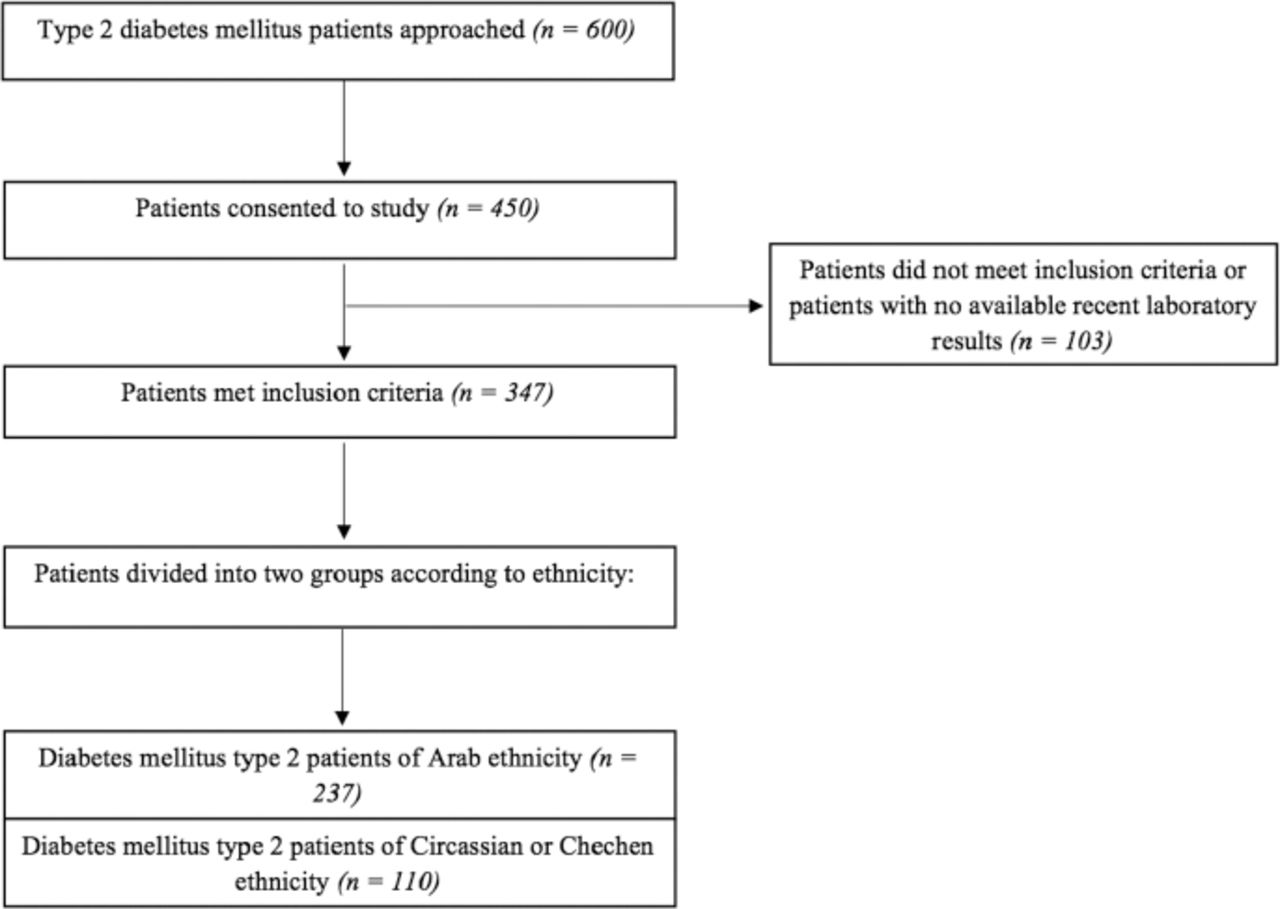
A flowchart of subjects and the studied sample.
Measurements and laboratory analysis
Anthropometric measurements were obtained at the interviews. The height was measured to the nearest centimeter using a standard height scale equipped with a headpiece, the weight was measured to the nearest kilogram using a standard mechanical weighing scale, and the waist circumference was measured to the nearest centimeter at the area of maximal circumference midway between the iliac spines and the lowest costal margin using a measurement tape during minimal respiration Laboratory data (fasting blood sugar, HbA1c, and lipid status components) was extracted from the patients’ medical records after acquiring their consent. The most recent lab data at the time of the interview were included, which had to be no more than 3 months prior to the interview, and the patient had to be on the same treatment plan he was on at the time of the interview.
Definition of variables
Level of education was divided into 3 categories: basic education (defined as not successfully finishing 12 years of school); secondary education (defined as successfully finishing 12 years of school but not holding a college/university degree); and graduate/postgraduate (defined as holding a college/university degree). Regular exercise was defined as 30 minutes of exercise at least 3 days a week as per the Jordanian health authorities’ guidelines. A person who had quit smoking more than 6 months prior to the interview was defined as a former smoker. A positive family history of a disease was defined as a confirmed diagnosis of that disease in a first degree relative. Patients were considered to have abdominal obesity if their waist circumference was 102 cm or greater in males and 88 cm or greater in females. The body mass index (BMI) was calculated using the equation: BMI = weight in kg / (height in m2). Patients were considered to be overweight if they had a BMI of 25-29.9 kg/m2, and obese if they had a BMI of 30 kg/m2 or greater as defined in the WHO Technical Report Series 894 / 2000. The following definitions and cutoff points were used in the study according to the ADA guidelines / 2015: glycemic control was considered satisfactory if HbA1c levels were <7.0%, and unsatisfactory if HbA1c levels were ≥7.0%. Elevated LDL was defined as ≥100 mg/dL, low HDL was defined as <40 mg/dL in males and <50 mg/dL in females, elevated cholesterol was defined as ≥200 mg/dL, and elevated triglycerides was defined as ≥150 mg/dL. Patients were considered dyslipidemic if they had at least one of the previously mentioned lipid abnormalities.
Statistics
The Statistical Package for the Social Sciences (IBM Corp., Armonk, NY, USA) version 22 was used for data entry and analysis. Categorical variables were presented as frequencies and percentages, while continuous variables were presented using mean and standard deviation. A p-value cutoff of 0.05 was used to determine statistical significance of a result.
Results
Participants’ characteristics
The socio-demographic details of the 2 populations are shown in Table 1. No statistically significant differences in age, marital status, or level of education were found between Arabs and Circassians/Chechens.
Socio-demographic characteristics of Arab diabetics and Circassian/Chechen diabetics.
Clinical and lifestyle details
As shown in Table 2, more Arabs (78.1%) reported a first degree relative with DM than Circassians/Chechens (59.1%), but more Circassians/Chechens (77.3%) reported a family history of hypertension than Arabs (65.1%). Of all participants 69.2% were diagnosed with and treated for hypertension. Differences between the 2 groups were found in Arabs having hypertension (75.5%) and dyslipidemia (76.8%), which was more than Circassians/Chechens’ hypertension (55.5%) and dyslipidemia (35.5%). Less than half of the total population (43.5%) were on a healthy low sugar, salt, and fat diet (43.5%), and 51.0% of all participants regularly exercised (30 minutes a day at least 3 days a week). Circassians/Chechens exercised more than Arabs, but there were more current smokers (20.0% versus 9.3%) and former smokers (27.3% versus 14.4%) in the Circassian/Chechen group. A total of 12.7% of participants were active smokers at the time of the interview.
Clinical and lifestyle details and differences between Arab diabetics and Circassian/Chechen diabetics.
Anthropometric measurements and obesity
Table 3 shows the anthropometric measurements and obesity details of the 2 ethnic samples. Arabs had significantly higher weight, waist circumference (WC), and waist-to-height ratio (WHtR)means than Circassians/Chechens. No differences were found in terms of BMI means or obesity status between the 2 ethnic groups. More Arabs (90.0%) were centrally obese according to waist circumference than Circassians/Chechens (69.8%).
Anthropometric measurements and obesity according to universal and Jordanian cutoffs in Arab diabetics and Circassian/Chechen diabetics.
Glycemic and lipid laboratory values
As shown in Table 4, both glycemic parameters studied (fasting blood sugar and glycosylated hemoglobin) were significantly higher in Arabs. Additionally, significantly more Arabs (60.6%) were found to have unsatisfactory glycemic control (HbA1c ≥7.0%) than Circassians/Chechens (38.2%). A total of 53.5% had unsatisfactory control. Most participants (88.8%) had at least one lipid abnormality (dyslipidemia). No significant differences were found in HDL means or percentage of patients with low HDL between the 2 groups. However, Circassians/Chechens had higher means of LDL, cholesterol, and triglycerides than Arabs. Circassians/Chechens elevated cholesterol (47.3%) and triglycerides (60.0%), which was more than Arabs cholesterol (20.3%) and triglycerides (42.6%).
Glycemic and lipid lab parameters in Arab diabetics and Circassian/Chechen diabetics.
Discussion
Factors for developing DM are generally categorized into modifiable (such as, diet, physical activity, lipid levels, and hypertension); and non-modifiable (such as, ethnicity, genetics, age, and family history of DM). Studying both types of factors is important to fully understand the pathogenesis of the disease and its progress, as well as its prevention and optimal management. This study was conducted with the aim of finding significant differences in terms of clinical, anthropometric, and laboratory characteristics between 2 genetically distinct ethnic groups sharing the same environment, and multiple differences were found. These differences should be considered when developing a management plan for Arab, Circassian, and Chechen people living with diabetes. Additionally, these findings are worth further exploration -genetically and clinically- in the hope of finding new risk or protective factors to the development and control of DM. Previous studies had explored hypertension, metabolic syndrome, prevalence of DM and glycemic control, and nutrient intake and its relation to diabetes in the Circassian and Chechen populations in Jordan.11-14 This study compares a combined diabetic Circassian/Chechen population with a diabetic Arab population living in Jordan in terms of clinical details, obesity, and glycemic and lipid lab parameters.
Socio-demographic characteristics were comparable between Arabs living with diabetes and Circassians/Chechens living with diabetes. These environment-determined similarities imply that differences found in other areas can be attributed to genetic differences between the studied ethnic groups. Hypertension is a common comorbidity among diabetes patients, and studies show a higher prevalence of hypertension in diabetics than in nondiabetics.15,16 Approximately 69.2% of the studied sample were diagnosed with hypertension and treated with antihypertensive medication. A study in the UK demonstrated a difference in hypertension among diabetes patients of different ethnic groups sharing the same environment;16 similarly, this study showed a significantly higher percentage of hypertension in Arabs with diabetes (75.5%) than in Circassians/Chechens with diabetes (55.5%). Self-reported dyslipidemia was also higher in Arabs (76.8%) than in Circassians/Chechens (35.5%).
High-fat diet and physical inactivity are established risk factors for development of DM.1,17 Exercise, on the other hand, is a protective factor against developing DM, and is an effective component in its management.18 Less than half of both groups were on a healthy low-fat diet. Circassians/Chechens living with diabetes exercise more than Arabs living with diabetes (74.5% of Circassians/Chechens with diabetes versus only 40.1% of Arabs with diabetes regularly exercise). These findings necessitate putting more emphasis on lifestyle modifications as an important component of DM management when treating DM in all studied ethnicities. More Circassians/Chechens were current or former smokers than Arabs.
Anthropometric indices are indicators of metabolic risk in general and DM risk in particular.19,20 Multiple studies had shown that indices that take the distribution of fat and central obesity into account (waist circumference and waist-to-height ratio) are better predictors of metabolic risk than indices that do not (weight and BMI).19,21,22 Anthropometric indices were examined and demonstrated a higher weight, waist circumference, and waist-to-height means in Arabs. Obesity, in particular, is a risk factor for development of DM, cardiovascular disease, and reduced life expectancy.1,23 It is increasing in prevalence in Middle-Eastern populations in general24 and the Jordanian population in particular.6,25 The studied sample showed that 60.6% of all participants were obese (defined as BMI ≥30 kg/m2), and 83.2% were centrally obese (defined as ≥102 cm WC in males or ≥88 cm WC in females). No differences were found in percentage of overweight or obese participants among the 2 ethnic groups. However, more Arabs were centrally obese (90%) than Circassians/Chechens (69.8%). Two glycemic laboratory parameters were analyzed, HbA1c and fasting blood sugar; Arabs with diabetes had higher means of both. It was also found that more Arabs (60.6%) had unsatisfactory glycemic control (HbA1c ≥7.0% as defined by the ADA) than Circassians/Chechens (38.2%). Previous studies carried out on Jordanian diabetic populations reported percentages consistent with the percentage found in participants of Arab ethnicity in our study but much higher than the percentage found in participants of Circassian/Chechen ethnicity.7,25,26 These results may indicate the presence of protective genetic factors in the Circassian/Chechen population in terms of glycemic control; factors that may have a role in the management of DM in that population in the future.
Dyslipidemia, as described earlier, is a common comorbidity of DM. It is still unclear if it is an independent risk factor for DM or just a confounding factor to obesity and glucose intolerance, however, it is an established risk factor for cardiovascular and ischemic heart disease, common causes of death in patients with diabetes.27 Of all participants, 88.8% were found to have at least one lipid abnormality and hence, dyslipidemia. Such a high percentage in both groups suggests a problem in the approach and management of dyslipidemia in Jordanian DM patients. Analysis of the components of dyslipidemia revealed that Circassians/Chechens had higher means of LDL, cholesterol, and triglycerides than Arabs. Circassians/Chechens also had a higher percentage of patients with elevated cholesterol (47.3%) and elevated triglycerides (60%) than Arabs cholesterol (20.3%) and triglycerides (42.6%).
This study had multiple points of strength. It analyzed 2 understudied diabetic ethnicities and compared them to a third; all living in the same environment and having similar environmental factors. Furthermore, multiple findings suggesting a different disease process among the studied ethnicities were found. Those differences can be used to guide DM public health programs that take them into account. One limitation of this study is the lack of multivariate analysis and that it did not utilize regression techniques.
In conclusion, this study compared genetically-isolated ethnic populations sharing the same environment in order to widen the understanding of any factors that contribute to the type 2 DM global epidemic. Multiple discrepancies between the 2 populations were found suggesting a role for genetic factors. New DM management recommendations and policies should be implemented when treating diabetic patients of those ethnicities particularly in areas of glycemic control, lipid control, and obesity. Moreover, further clinical and genetic studies aimed at these populations should be designed in the hope of discovering novel risk and protective factors in DM type 2 pathogenesis, glycemic control, obesity, and dyslipidemia in diabetic patients.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company. This study was funded by the Deanship of Research (RN: 20130242), Jordan University of Science and Technology, Irbid, Jordan.
- Received October 29, 2016.
- Accepted November 16, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.