


Abstract
Objectives: To evaluate the influence of the ORM1 variants in codon 118 on the intra-operative remifentanil consumption under general anesthesia.
Methods: A prospective gene association study, performed at the Jordan University Jordan, Amman, Jordan from September 2013 to August 2014. It includes patients who underwent septoplasty surgery under general anesthesia. All patients received standard intravenous anesthesia. Anesthesia maintained with fixed dose of Sevoflurane and variable dose of Remifentanil to keep the systolic blood pressure between 90-100 mm Hg. The Remifentanil dose was calculated and correlated with ORM1 genotype variance.
Results: Genotype and clinical data were available for 123 cases. The A118A genotype was seen in 96 patients (78%), the A118G genotype was seen in 25 patients (20.3%), and only 2 patients had genotype G118G (1.6%). The G118G variant was removed from the statistical analysis due to small sample size. There was a significant effect of ORM1 genotype variant and the amount of remifentanil consumed. The A118A genotype received 0.173 ± 0.063 µg kg-1 min-1 and the A118G genotype received 0.316 ± 0.100 µg kg-1 min-1 (p<0.0001).
Conclusion: The ORM1 gene has a role in intra-operative remifentanil consumption in patients who underwent septoplasty surgery under general anesthesia. The A118G gene required higher dose of remifentanil compared with the A118A genotype.
The human mu1-opioid receptor (OPRM1) is the primary site of action for many endogenous opioid peptides, including β-endorphin and encephalin, as well as the major target for opioid analgesics.1 Polymorphisms in the OPRM1 gene may be associated with clinical variation on the patient’s response to opioids.2 A number of single nucleotide polymorphisms (SNPs) have been described for OPRM1, with the A118G mutation being the most common one. It is known to lead to a change in the gene product in the OPRM1, which is an A to G substitution in exon 1, which results in an amino acid exchange at position 40 from asparagine to aspartate.3,4 Opioids are used widely to control pain in the intra-operative and post operative period. Many opioid drugs used for this purpose, such as morphine, fentanyl, sufentanil, and remifentanil. Several recent studies focused on the effect of OPRM1 gene polymorphism and the opioid consumption either in the postoperative period, patients with chronic or cancer pain, or pain related to child birth. A recent systemic review and meta-analyses study investigated the effect of OPRM1 polymorphisms on the requirement of opioids in the postoperative period.5 Morphine and fentanyl were the most commonly studied opioid drugs, and the populations of these studies were mainly from Asian and Caucasian ethnic groups. The meta-analysis provided evidence that there is variation in the amount of opioid consumed in the postoperative period in correlation with OPRM1 A118G polymorphism and this variation depends on the type of opioid used, type of surgery, and the difference in ethnic group. In one study conducted on Chinese women,6 researchers assessed the association between SNPs in the OPRM1 gene and intraoperative remifentanil consumption in patients who had surgery under monitored anesthesia care (MAC). From our observation, we thought that there is variation in the amount of Remifentanil consumed intra-operatively in Jordanian patients, and this difference came from gene variance. Our hypothesis was that the A118G polymorphism contributes to the amount of intraoperative Remifentanil consumption. Confirmation of this correlation might help anesthesiologists in identifying sensitive and resistant patients to Remifentanil, especially in long surgeries that required hypotensive anesthesia. The primary outcome in our current study is to assess the correlation between intra-operative remifentanil consumption and the OPRM1 A118G polymorphism in Arab ethnic group patients who underwent surgery under complete general anesthesia.
Methods
Approval of this study was provided by the Scientific Committee of the Faculty of Medicine at the University of Jordan on the 8th of January 2014. An informed written consent from each patient involved in the study was obtained. The patients included in the study were scheduled to undergo elective septoplasty under general anesthesia at the Jordan University hospital, Amman, Jordan. Patients aged 18-60 years with American Society of Anesthesiologists (ASA) physical status I or II where included in the study. Exclusion criteria included any patients having hypertension or other cardiovascular disease, diabetic patients, patients who received blood, blood products or colloids fluid during surgery, patients who had kidney or liver disease, chronic pain patients, those taking pain drugs, or their weight is above 130 kg. The data collected for all patients underwent septoplasty surgery over one year, starting from the first of September 2013.
Patients ate and drank nothing after midnight, the night before surgery. A standardized general anesthesia technique was used for all patients. Non invasive blood pressure (NIBP), electrocardiography, and saturation of peripheral oxygen (SpO2) were applied to all patients inside the operation room and base line readings were recorded. An intravenous cannula 18-gauge was inserted in the dorsum of hand. A blood sample was taken and sent to the genetic lab. After pre oxygenation, general anesthesia started with 1 µg kg-1 fentanyl, 2 mg kg-1 propafol and 0.6 mg kg-1 Rocoronium were given. After confirmation of endotracheal intubation, sevoflurane started with 2 volume % and a constant gas flow (2 L oxygen and 2 L air). Remifentanil with a concentration of 40 µg ml-1, started with initial dose of 0.1 µg kg-1 min-1. The surgeon injected in the patient nasal septum 2 ml of 2% lidocaine with epinephrine (1:100,000). The reverse Trendelenburg position (30° head up) was chosen for all patients. An automated NIBP reading was programmed to be taken every 2.5 minutes and the doses of remifentanil were adjusted so as to attain a systolic blood pressure (SBP) of 90-100 mm Hg. The SBP and heart rate (HR) readings were recorded every 5 minutes. At the end of the procedure, the primary anesthesiologist stopped the remifentanil infusion and chose another analgesic medication to cover the postoperative period. The total amount of remifentanil (in millimeters), total amount of intravenous fluid, and duration of surgery were recorded. The primary anesthesiologist had the right to stop the protocol if he feels there is any risk to the patient.
Sample collection
Blood samples were collected in EDTA tubes from venous blood. DNA extraction was performed using the Puregene Blood Core Kit A (Qiagen, Maryland, USA) according to the manufacturers protocol. DNA quantity and quality were assayed by a spectrophotometer (Biorad, USA). DNA was stored at -20C until use.
DNA amplification
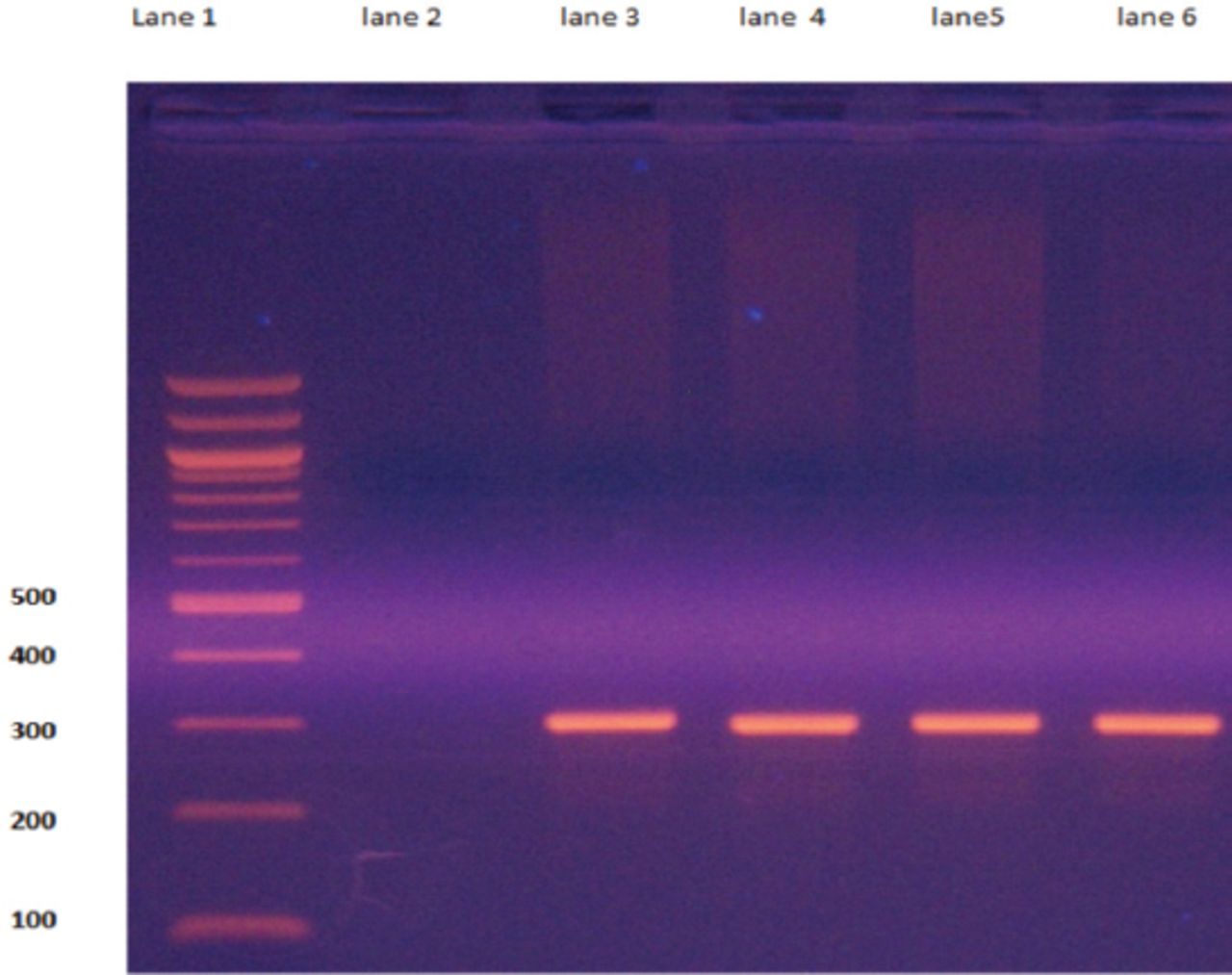
For A118G genotyping, the total volume of polymerase chain reaction (PCR) amplification was 25 µl, which contained 10-50 ng of DNA, 0.2 mM of each deoxynucleosidetriphosphates (dNTPs) (promega, USA), 5 µl buffer (100 mM Tris-HCl, 15 mM MgCl2, 500 mMKCl, pH 8.3), 0.1 mM of each primer, 1.5 mM of each MgCl2 and 1 U of Taq DNA polymerase (Promega, USA). The forward primer was 5’-GAAAAGTCTCGGTGCTCCTG -3’ and the reverse primer was 5’-GGAGTAGAGGGCCATGATCG-3’. The PCR amplification started with denaturation at 95°C for 5 min, followed by 35 cycles of denaturation (94°C, 30 sec), annealing (60°C, 1 min), and extension (72°C, 1 min). A final extension step was performed at 72°C for 7 min. The PCR product size was 293 bp (Figure 1).
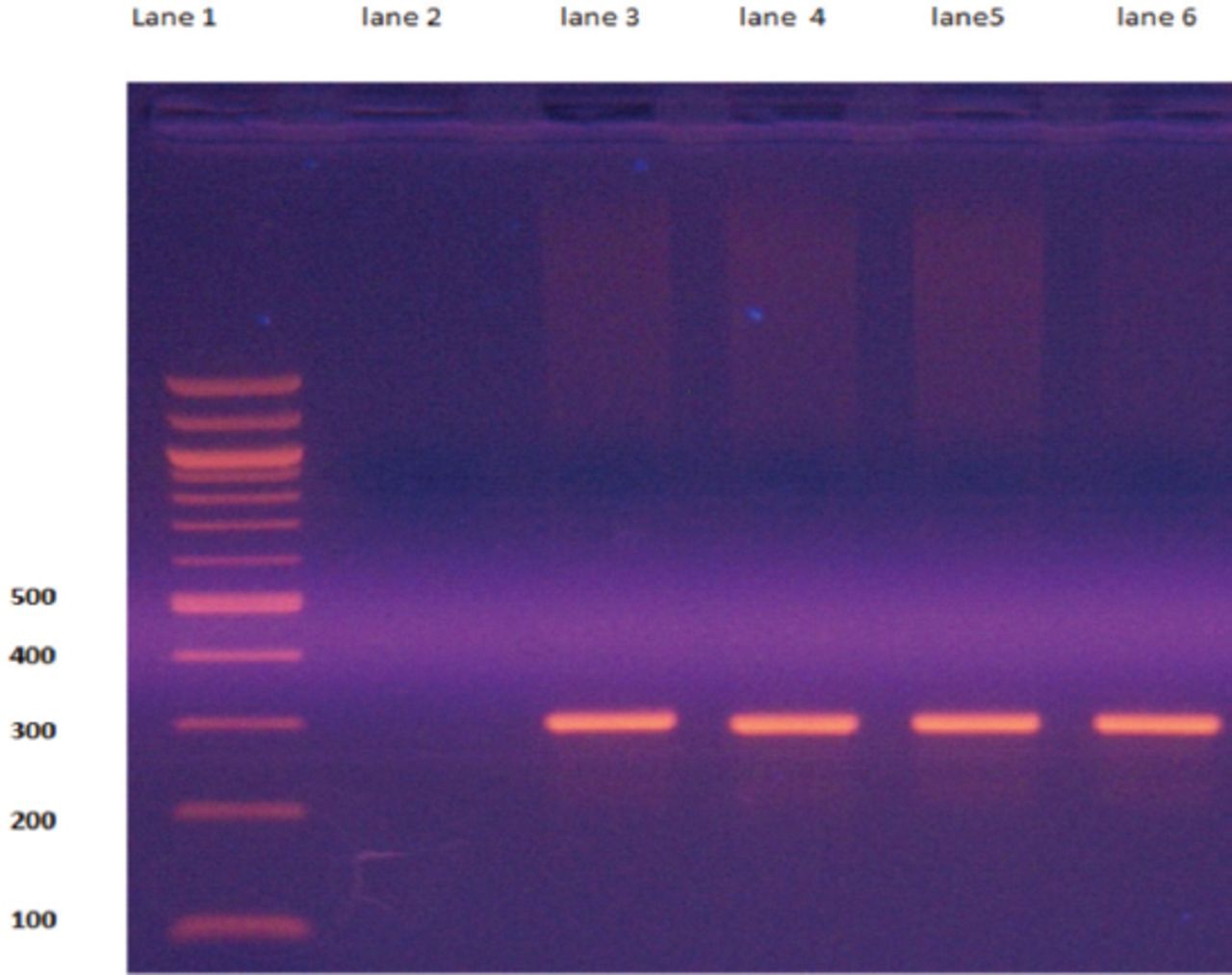
Representative polymerase chain reaction (PCR) products for A118G genotype. Lane1 is a 100 bp ladder, lane 2 shows non-template controls, while lanes 3 to 6 represent the PCR products (293 bp).
DNA Sequencing
A118G genotype was sent for DNA sequencing (Macrogen, South Korea). The PCR products were purified using the QIAquick PCR Purification kit (Qiagen, Germany).
Statistical analysis
For this study, all the statistical analysis of data was performed using the software package Statistical Analysis System version 9.4 (SAS Institute Inc., Cary, NC, USA). Descriptive statistics for the continuous variables are reported as mean ± standard deviation and categorical variables are summarized as frequencies and percentages. Continuous variables are compared by student’s t-test, while categorical variables are compared by Chi-square test. The level of statistical significance is set at p<0.05. The chi-square test was used to verify Hardy-Weinberg equilibrium.
We hypothesize that the frequency of G alleles to be 20% in our patients based on previous studies that were conducted in Caucasian populations.7,8 Using the prevalence rate of 20%; and with 95% confidence interval to control the error of estimation to within a 7% error margin and for type I rate of 5%, the calculated sample size we needed was 125. Taking into consideration that patients might be excluded from the study, we enrolled in the study 147 patients.
Results
From the first of September 2013 to the 31st of August 2014, the total number of septoplasty surgeries performed at the Jordan University hospital were 147 cases, and 17 cases were excluded from the study either because they did not fulfill the inclusion criteria (2 patients) or they refused to be enrolled in the study (15 patients). There were 130 patients enrolled in our study who signed the consent form. Seven cases were removed from the statistical analysis due to incomplete data, and 123 cases were involved in the statistical analyses. The minimum age of those patients was 18 year and the maximum was 46 year. The total intravenous fluid range was 250-750 ml. The duration of surgery was between 25-70 minutes. The minimum body mass index (BMI) was 17.1 and the maximum was 40.5.
We divided the patients into 3 groups according to genotype results. The A118A genotype was seen in 96 patients (78%), the A118G genotype in 25 patients (20.3%), and only 2 patients had the genotype G118G (1.6%). The G118G gene was presented in 2 cases only and due to very small sample size in this group; we excluded G118G from the statistical analysis. The analysis was completed for the genotypes A118A and A118G, and 121 cases were included in the statistical analysis.
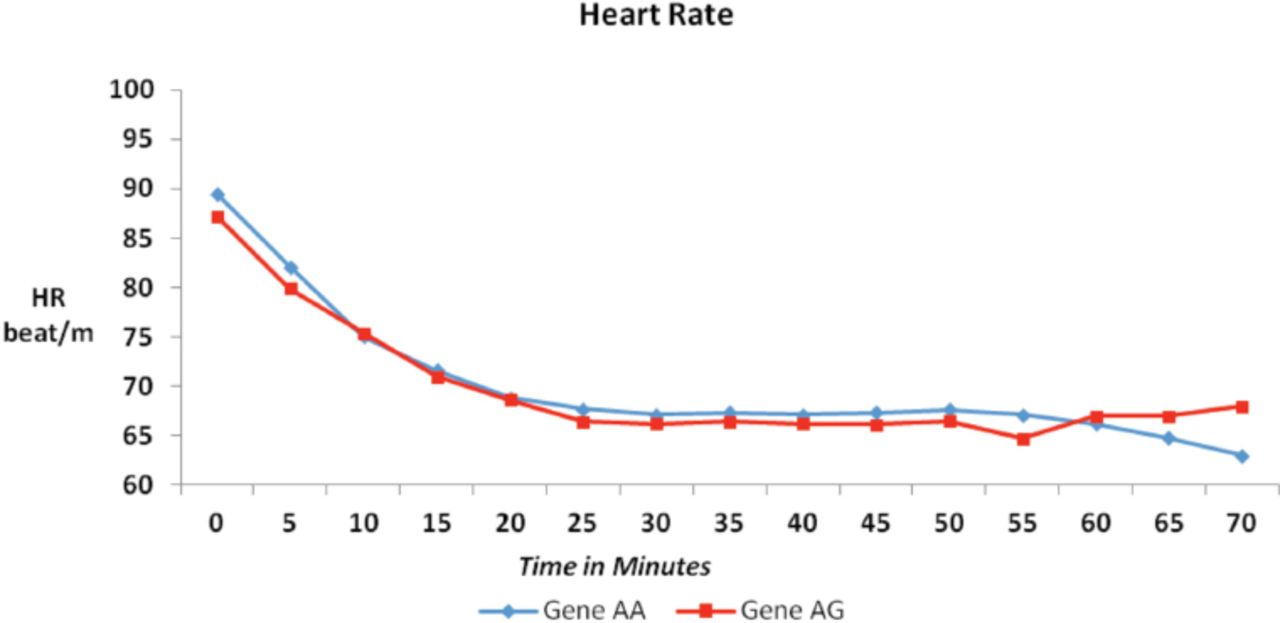
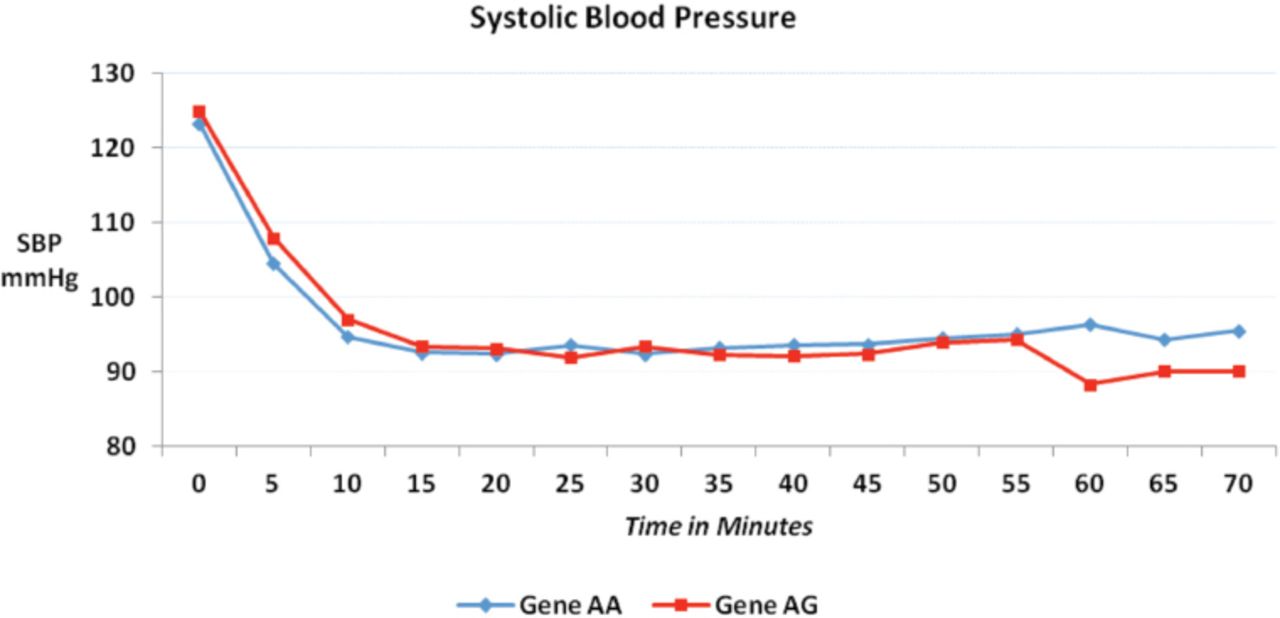
The patients’ gender, ASA status, age, total intravenous fluid, duration of surgery, basal HR, and basal SBP were comparable between the 2 groups (A118A and A118G). The p-value was not significant >0.05 (Table 1). The BMI was significant between the 2 groups (p=0.027). The SBP and HR during surgery from the basal HR until 70 minutes were comparable between the 2 groups. The p-value was not significant at any time as shown in Figures 2 & 3. The mean value of SBP in the 2 groups was between 90-100 mm Hg after 10 minutes from taking the base line reading until the end of the procedure, as shown in Figure 3.
Patients characteristics and demographic data of codon 118 genotypes.

Heart rate (HR) variation over 70 minutes (m) after induction of general anesthesia for the codon 118 genotype.

Systolic blood pressure (SBP) variation over 70 minutes after induction of general anesthesia for the codon 118 genotype.
The amount of remifentanil used during surgery was calculated in µg kg-1 min-1. The dose of remifentanil in group A118A was 0.173 ± 0.063 (Mean ± standard deviation [SD]) µg kg-1 min-1. And the dose in group A118G was 0.316 ± 0.100 (Mean ± SD) µg kg-1 min-1. The p-value was highly significant <0.0001 (Table 2). It is worth mentioning that the dose of remifentanil used in the 2 patients in group G118G was 0.286 and 0.311 µg kg-1 min-1.
Remifentanil dose consumption of codon 118 genotype.
Our results were in Hardy-Weinberg equilibrium, there was no statistical significant between the observed and expected genotype frequencies, p-value was 0.8. the A alleles frequency was 217 (88.2%) and the G alleles was 29 (11.8%) as shown in Table 3.
Genotype and allele frequency association.
Discussion
Most of the studies performed on the human mu-opioid receptor gene and opioid requirement were conducted in the post-operative time. The mood and anxiety of the patients, emotional states, and attitudes of patients toward pain before surgery might alter opioid requirements in the post-operative time.9 To avoid the effect of those factors we designed our study to calculate the amount of narcotic used in the intra-operative time for patients who underwent septoplasty surgery under general anesthesia. The Liu et al6 study was the only study done in the intraoperative time and they used remifentanil as a narcotics agent. In this study, anesthesia was performed under MAC and maintained by the intravenous infusion of remifentanil during hysteroscopy surgery. In their study they assessed the intra-operative pain using the visual analogue score (VAS), gave fixed weight adjusted dose (µg kg-1 min-1), and gave a bolus dose of 0.25 µg kg-1 to keep VAS below 3. Our study was build on the Liu et al6 study, and the main difference was that our study was conducted under complete general anesthesia and the only factor that decided the dose of remifentanil was the value of SBP affected by severity of pain that comes from surgical stimulation. Sympathetic stimulation caused by painful surgical stimuli leads to increase secretion of catecholamines from the adrenal medulla and release of norepinephrine from presynaptic nerve terminals. The increase in sympathetic activity results in the well recognized hemodynamic effect of tachycardia and hypertension.10 During anesthesia we counteracted this raising of blood pressure by giving opioids medications to control the pain that results from surgical stimulation.
We standardized the general anesthesia for all patients; it was conducted under general anesthesia with endotracheal intubation, using standard dose of drugs for induction and maintenance of anesthesia. The only variable was the dose of remifentanil that was given in a weight adjusted dose to keep the SBP between 90 and 100 mm Hg, which was also a surgeon demand. Remifentanil is short acting, easy to be titrated to control blood pressure and it decreases HR. It is a fast acting mu-opioid receptor agonist that is metabolized rapidly, making it a good choice to control blood pressure during surgery. Remifentanil is used widely in hypotensive anesthesia for nasal surgery, it provides low blood pressure and low HR, which is reflected in surgical field and decreased blood loss during surgery.11 In hypotensive anesthesia, the most satisfactory technique is a combination treatment of remifentanil with either propofol or an inhalation agent (isoflurane, desflurane, or sevoflurane) at clinical concentration.12 We used fixed concentration of sevoflurane (2 volume %) to maintain anesthesia and adjusted the remifentanil dose to control the SBP. In our study, the SBP was well controlled in all patients and the mean value of SBP and HR were comparable between the 2 gene groups (A118A, A118G) from the start of anesthesia until the end of surgery (Figures 2 & 3).
The BMI was 25.7 ± 4.5 in group A118A and 23.5 ± 3.8 in group A118G, and the p-value was significant (p=0.027). This variation in the BMI between the 2 groups did not affect our results; we gave remifentanil in weight adjusted dose.
Despite evidence of enormous differences in pain sensitivity and analgesia across ethnic groups,13-15 previous studies were performed with limited ethnic diversity. Hwang et al,5 analyzed 18 studies, where all populations analyzed in these studies were either Caucasian or Asian. The meta-analysis provided evidence that the OPRM1 A118G polymorphism in OPRM1 was associated with postoperative pain response in patients who were Asian but not Caucasians, used morphine, or received viscus surgery. Such variation in results among different ethnic groups, may confirm that data derived from genetic studies must always be considered with respect to ethnic background. Large interindividual differences exist in pain sensitivity and analgesic response, can be explained by genetic variations. Chau et al,16 found that patients with AA genotype required less postoperative morphine dose than patients with genotype AG or AA. Also, Liu et al,6 found that patients carrying one or 2 copies of the minor allele (G allele) required significantly more intraoperative remifentanil than in patients without the minor allele (p=0.001). We performed our study on Jordanian patients (Arab ethnic group) and our findings coincide with Liu et al,6 where the remifentanil consumed in the intra-operative time to maintain a SBP between 90-100 mm Hg was higher in AG gene compared with AA gene. The mean required dose of remifentanil for patients with AG gene was 0.316 µg kg-1 min-1, and for the patients with AA gene it was 0.173 µg kg-1 min-1 (p<0.0001).
The genotype frequency was variable between different studies. The GG mutant homozygous was seen more in Asians compared with Caucasians.6 The lowest frequency of the GG genotype was seen in a Pennsylvanian population (1%).17 The highest frequency was seen in a Taiwan population (22.5%).13 In our study, the frequency was only 1.6% (2 patients only). Such variations in the frequency between ethnic groups might explain the differences in opioid requirements in different populations.
Study limitations
We used a fentanyl with weight adjusted dose (1 µg kg-1) in induction of anesthesia; this opioid drug might have variable effect on the patient’s hemodynamic parameters. It was preferable to use remifentanil to facilitate induction beside maintenance of anesthesia. Another limitation of our study is that the fasting time was variable. While all patients started fasting at midnight on the day before surgery, the time of surgery was variable. Even though the sample size of the patients was 130 patients, the GG gene was seen in 2 patients only, a bigger sample size might produce more GG gene patients so that we can include those patients in statistical analysis.
In conclusion, the genetic variation of the mu-opioid receptors was associated with a different drug dose of intravenous, intra-operative remifentanil infusion. Jordanian patients who underwent septoplasty surgery under general anesthesia required more remifentanil dose in the A118G gene group in comparison with patients with homozygous for the A allele involving nucleotide 118 of OPRM1.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company. This study was funded by the Deanship of Scientific Research, The University of Jordan, Amman, Jordan. The study was completed during sabbatical leave at King Faisal Specialist Hospital and Research Center, Riyadh, Kingdom of Saudi Arabia.
- Received September 27, 2016.
- Accepted November 2, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.