


Abstract
Objectives: To analyze the relationship between clinical features, hormonal receptor status, and survival in patients who were diagnosed with medullary breast cancer (MBC).
Methods: Demographic characteristics, histopathological features, and survival statuses of 201 patients diagnosed with MBC between 1995 and 2015 were retrospectively recorded. Survival analyses were conducted with uni- and multivariate cox regression analysis.
Results: Median follow-up time was 54 (4-272) months. Median patient age at the time of diagnosis was 47 years old (26-90). Of the patients, 91.5% were triple negative. Five-year recurrence free survival time (RFS) rate was 87.4% and overalll survival (OS) rate 95.7%. For RFS, progesterone receptor (PR) negativity, atypical histopathological evaluation, absence of lymphovascular invasion, smaller tumor, lower nodal involvement were found to be favourable prognostic factors by univariate analysis (p<0.05). The PR negativity and smaller tumor were found to be favourable factors by univariate analysis (p<0.05). However, none of these factors were determined as significant independent prognostic factors for OS (p>0.05).
Conclusion: Turkish MBC patients exhibited good prognosis, which was comparable with survival outcomes achieved in the literature. The PR negativity was related to a better RFS and OS rates.
Despite the fact that breast cancer is the most common malignant tumor in women, medullary breast carcinoma (MBC) is a very rare histological subtype of breast cancer. The incidence of MBC has been reported between 1% and 5%.1 The patients with MBC are generally younger than the patients of other types of breast cancer, and with a better survival rate. MBC may be confused, clinically and radiologically, with benign cases like fibroadenoma. Histologically, it presents large vesicular nuclei, distinctive nucleoli, wide-brimmed with prominent lymphocyte infiltration within and around the tumor sheets. It is called a typical MBC when fully reflecting these characteristics, and an atypical medullary breast carcinoma if it does not.1,2 According to gene expression profıle, the breast carcinoma may be evaluated in 4 different patterns as in luminal, Her/neu2 positive, basal-like tumors, and breast-like tumors. Medullary breast carcinoma is considered in the basal-like breast cancer group. Although this group has commonly poor prognosis, MBC has been reported to have a good prognosis. Medullary breast carcinoma cases are observed more frequently in younger age groups and the factors affecting its prognosis are still unknown.1-5 Identification of patients with poor prognosis is important to provide more effective treatment for MBC. The aim of the current study was to illustrate the status of hormonal receptors and their effect on the survival and clinical outcomes in patients with MBC.
Methods
A total of 201 patients, diagnosed with MBC between 1995 and 2015 at 12 medical oncology departments of Elazig, Istanbul (5 department), Ankara (2 department), Izmir, Trabzon, Bursa, Kayseri, and Zonguldak were prospectively recruited. The study was conducted in compliance with the rules and regulations proposed by the Ministry of Health in Turkish Republic and the Declaration of Helsinki. The study was approved by Firat University Ethics Committee, Elazig, Turkey. Cases with missing medical data were excluded from the study. Detailed medical data (including clinical notes, histology, and radiology reports) were collected to obtain information regarding the age at diagnosis, menopausal and hormonal status, primary tumor size, histologically tumor type and grade, degree of nodal involvement, perineural and vascular invasion of tumor, family history and type of surgery. Tumor oestrogen receptor (ER), progesterone receptor (PR) and Her/neu 2 status were evaluated using the immunohistochemical (IHC) method, fluorescence in situ hybridization (FISH) was conducted in the presence of score 2 for Her/neu 2. Positive interpretation was evaluated where more than 10% of tumor cells exhibited positive nuclear staining of any intensity.6 The positive of hormone receptor (HR) was assessed as both of ER and PR positive or ER positive or PR positive. The survival end points were recurrence-free survival time (RFS) and overall survival (OS) for the present study. Overall survival was defined from the date of diagnosis until the time of death or the date of the last visit. Recurrence due to MBC was evaluated as locoregional (the same and the other breast, chest wall, axillary and supraclavicular or infraclavicular lymph node), distant recurrence (bone, liver, lung, brain, other lymph nodes, and secondary tumors) or as MBC induced-death.7 Statistical analyses were evaluated using the Statistical Package for the Social Sciences (IBM corp. Armonk, NY, USA) version 22. Survival analysis and curves were estimated based on the Kaplan-Meier method. Multivariate and univariate analysis of prognostic factors related to survival were performed with the cox proportional hazards model. Results within 95% confidence interval (CI), and p<0.05 were considered as statistically significant.
Results
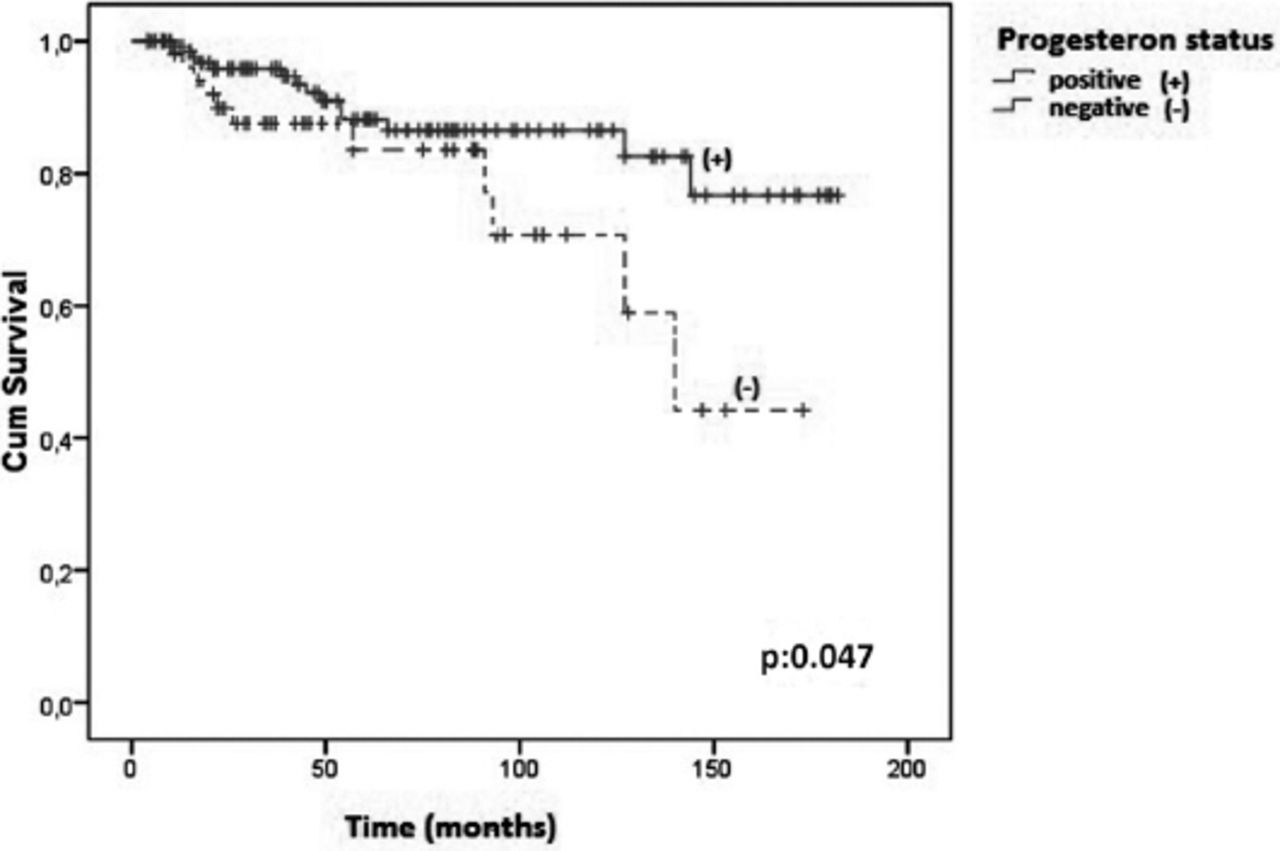
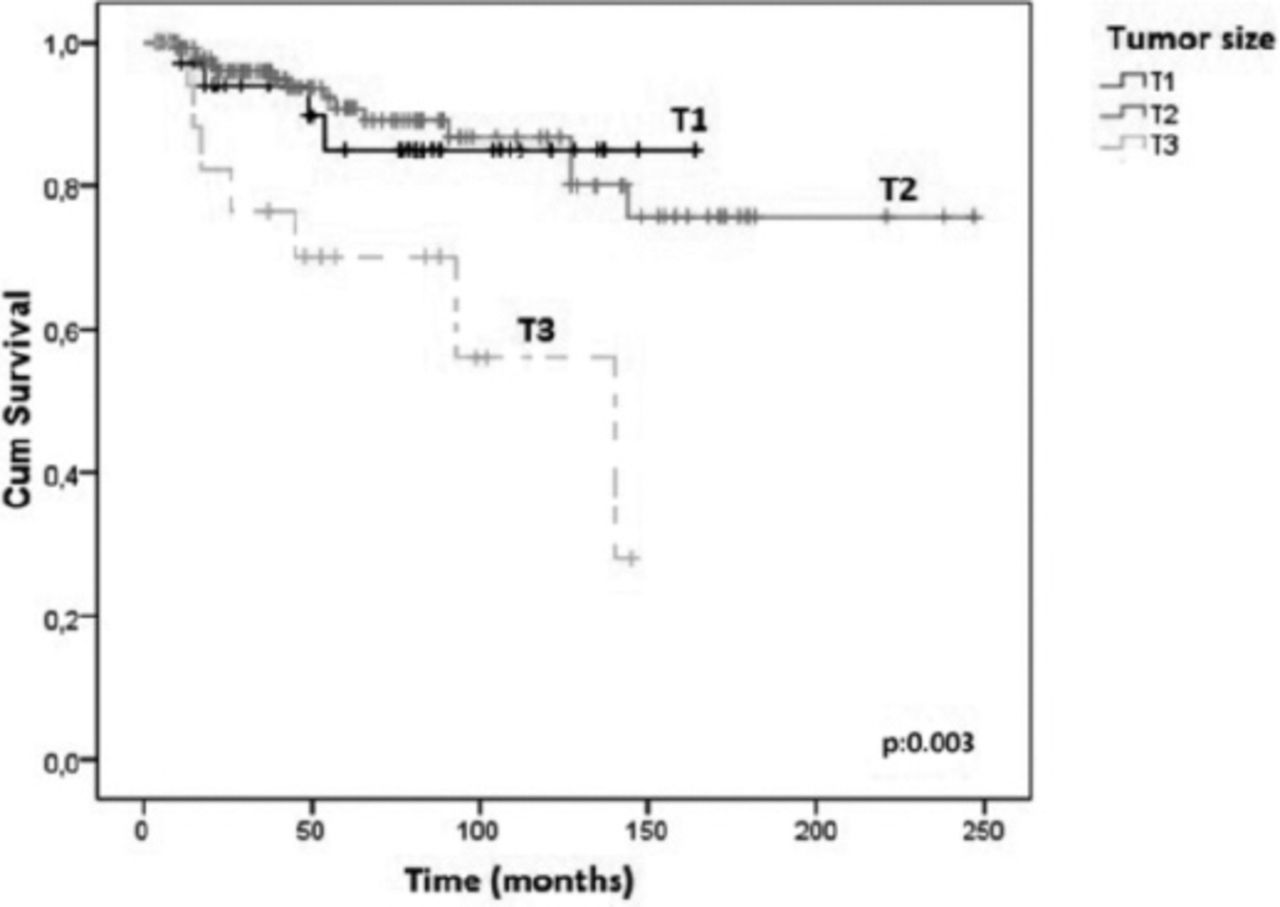
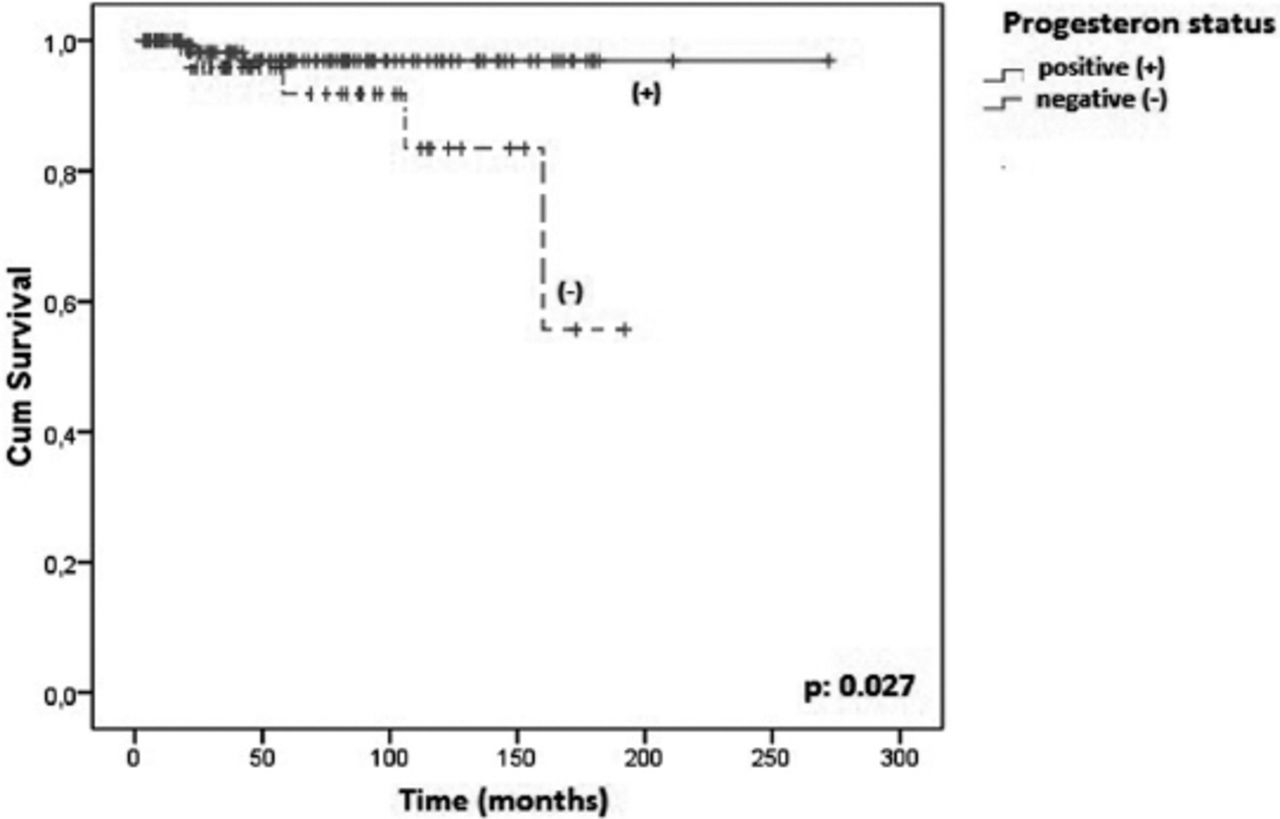
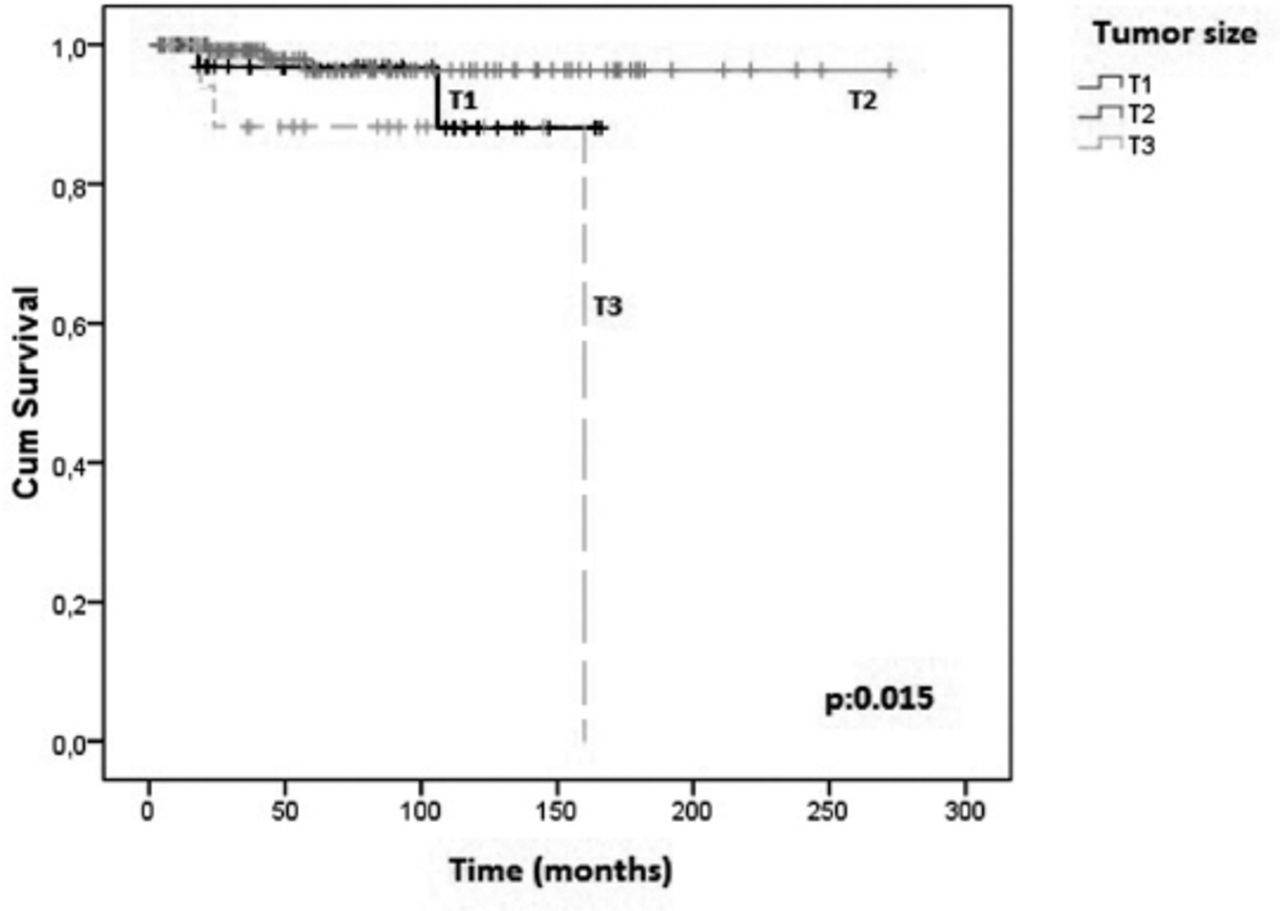
The median age of patients at the time of diagnosis was 47 years old (26-90). Median follow-up time was 54 months (4-272) among MBC patients. The general characteristics of the patients are shown in Tables 1 and 2. Twenty five of 201 MBC patients exhibited recurrence in median follow-up time. Median RFS and OS values were both not achieved. Mean RFS was 199.69 ± 8.96 (95% CI: 182.11-217.26) months, mean OS was 252.82 ± 7.45 (95% CI: 238.22-267.42) months. Five-year RFS rate was 87.4% and OS rate was 95.7%. Univariate analysis was used to estimate prognostic factors affecting the RFS (Table 1) and OS (Table 2). It was observed that PR negativity, small tumor size, atypical histopathological evaluation, absence of lymphovascular invasion and low degree of nodal involvement were favorable prognostic factors for RFS, (Figures 1 & 2) and (Table 1). The PR negativity and small tumor size were found to be significant favorable prognostic factors according to univariate analysis for OS (p<0.05), (Figures 3, 4, & Table 2). The PR status, tumor size, degree of nodal involvement, and evaluation of surgical margins were not determined as statistically significant independent predictors for both RFS and OS (p>0.05). Most of the patients with recurrences were observed to have distant metastases (66.6%). Three of these patients (11.15%) with recurrences had metachronous cancer.
Univariate analyses for recurrence-free survival (RFS).
Univariate analyses for overall survival (OS).
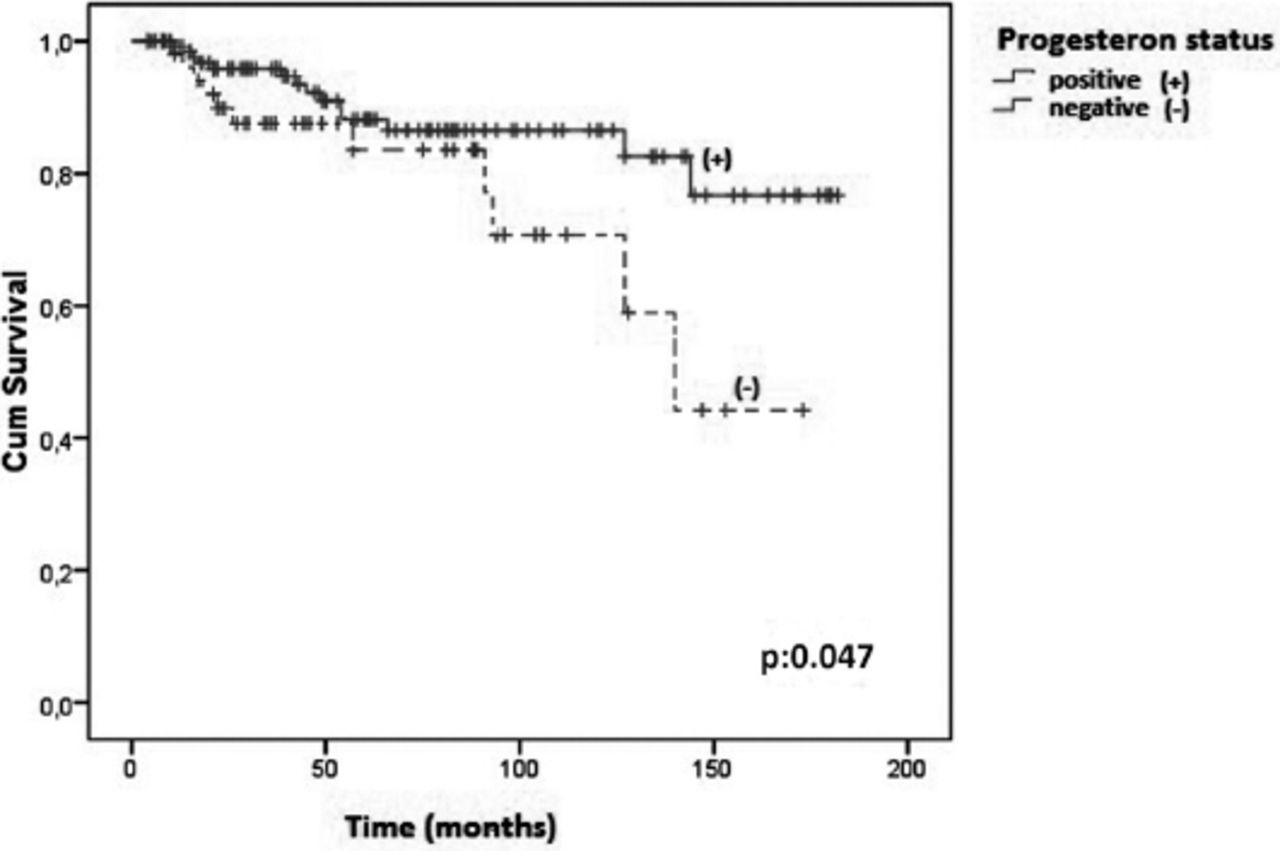
Relapse–free survival graphic according to progesterone receptor status.
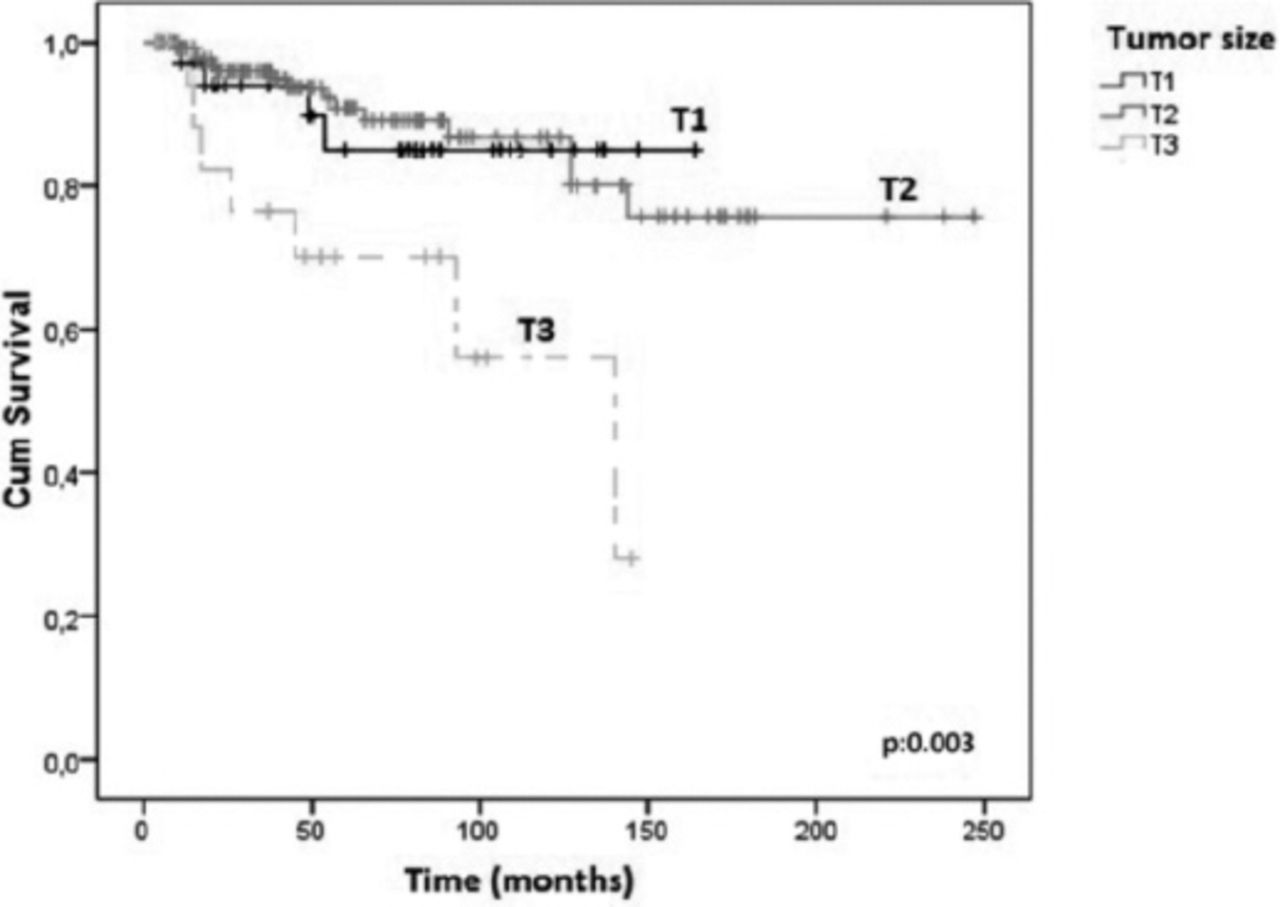
Relapse–free survival graphic according to tumor size.

Overall survival graphic according to progesterone receptor status.
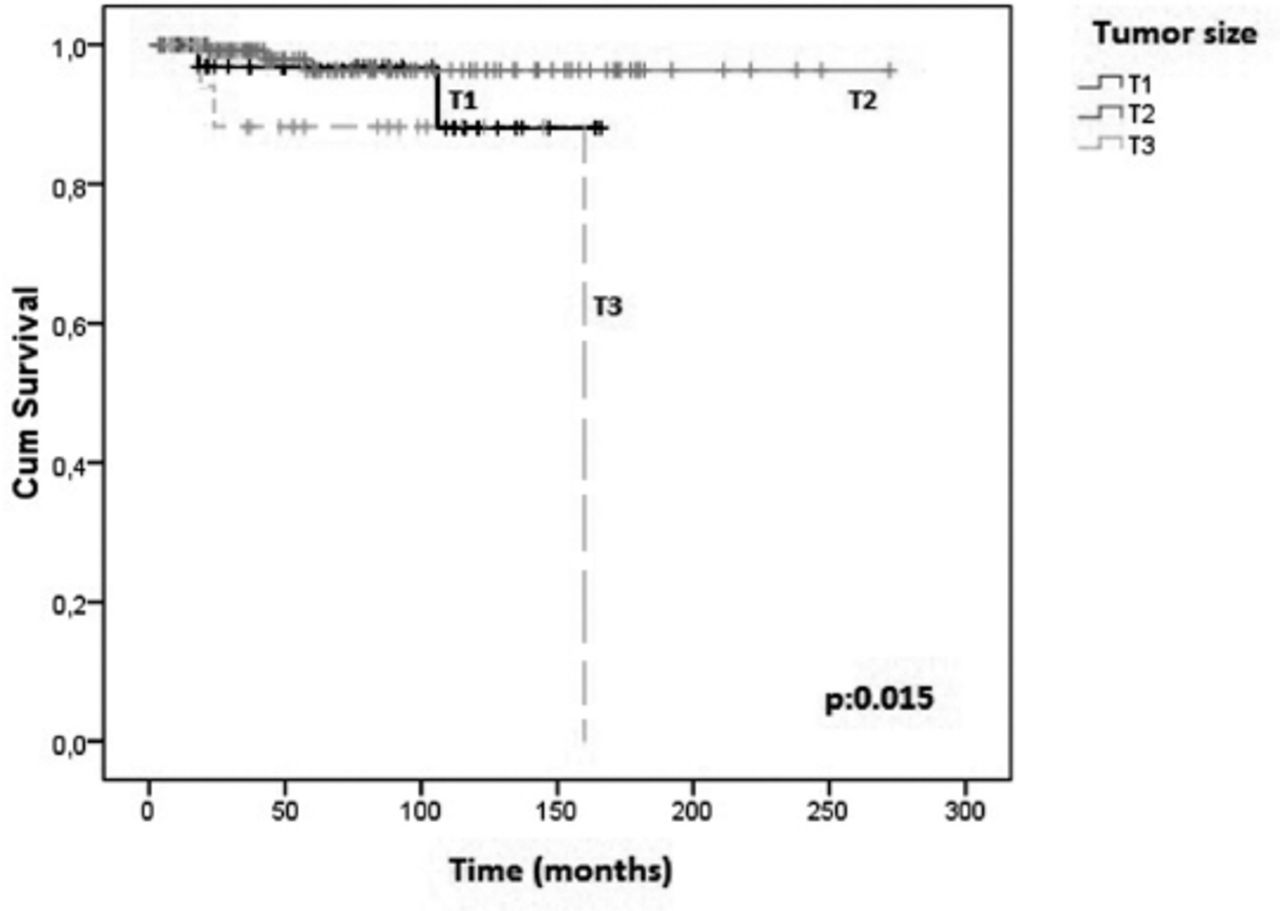
Overall survival graphic according to tumor size.
Discussion
Breast cancer is one of the most prevalent cancers among women, but histological subtypes of breast cancer and especially MBC are seen rarely and1 also known for their favorable prognosis.4 The features of MBC such as histomorphologic structure and prognosis were discussed in some studies.8-12 In the present study, we described prognostic factors of recurrence and survival time in patients who were diagnosed with MBC. Women under 40 years of age are usually defined as young individuals and those under 35 are defined as very young in the literature.13,14 The patients with MBC are generally younger than other patients who had different types of breast cancer and patients who had breast cancer at earlier ages were associated with BRCA1-2 mutations.1,2 Median age of patients was 47 years old and the rate of younger patients (<35) was 10.4% in our study, similar to the findings of Park et al,9 which reported that median age of patients was 44 years old, and the rate of younger patients was 13.5%. Based on our results, the low incidence of MBC among very young women was consistent with the findings in the literature.1,2,7 According to previous studies, T2 tumors were identified as the most common and T1 tumors were determined as the least common type in the present study.7-11 Similar to previously mentioned studies, the lymph node involvement was not observed in the majority of our patients. Most of the patients (65.7%) had no lymph node involvement, while 22.9% of the patients with N1, 8.5% with N2, and 3% with N3 breast tumors were observed. In our study, we determined that this was reflected positively on the RFS in patients’ absence of lymph nodes, similar to the literature.8,9,15
Hormonal receptors, such as ER, PR, Her/neu-2 are predictive prognostic factors, and cornerstone of the treatment of patients with breast cancer. It is known that MBC was observed with the lowest frequency of ER, PR, Her/neu-2 expression based on previous studies.1,16 The ratio of high grade (grade 3) tumor was 71.1% in our study. The presence of LVI and high grade tumors, which were detected among featured more aggressive tumors, were identified in a large portion of our patients. It was observed that the presence of LVI was determined as an unfavorable prognostic factor for RFS. It was determined predominantly as a high grade tumor similar to other studies.1,17,18 Furthermore, 66.3% of patients in terms of HR, 72.7% of patients in terms of PR status, 79.8% of patients in terms of Her/neu-2 were evaluated as negative, similar to other studies.19,20 In this case, it was considered that these patients could benefit less from hormone suppression therapy.
Although our study showed that more tumors were identified as HR negative (90.47%) and triple negative (61.9%) in the group of patients aged <35 years old, Cao et al.21 reported that, among patients aged <40 years old, 50% were in the HR negative group and 44% were in the triple negative group.
In the present study, we found that PR expression rate was low (27.3%). This ratio was identified as high expression,21 although some of the cases were identified as low expression similar to our findings.18,20 Although studies including PR status associated with MBC are rare in the literature, Cao et al.21 determined that positivity of PR present an unfavorable risk factor on RFS patients with MBC. Rakha et al.22 reported that tumors with ER negative/PR positive status had more aggressive clinical outcomes than tumors with ER positive/PR negative status (p<0.01 for RFS, p<0.03 for OS) in all breast cancers. It has been demonstrated in recent studies that PR negative patients have no responder to complete response after neo-adjuvant chemotherapy in patients with local advanced breast cancer.23 We have determined that especially atypical histopathological patterns were significantly independent predictors of RFS (p<0.05). Similarly, Rakha et al24 obtained better survival rates in patients with the typical character of MBC when compared with patients who had atypical character, but they found that the difference was not statistically significant. In contrast, 4 of our 25 patients presented an atypical recurrence and a longer RFS. Typically, MBC is known to have prominent lymphocyte infiltration within and around the tumor sheets contrary to atypical MBC, which has less lymphocyte infiltration within tumor sheets. While lymphocyte infiltration in tumor tissue of typical MBC is denser, less lymphocyte infiltration is observed in atypical MBC.2,16,22,24 Although these features seem to be simple distinguishing factors of both types of MBC, pathologists sometimes fail to subtype MBC. Recently, a new terminology including both typical and atypical MBC, medullary-like carcinoma was emphasized.25 The recovery of some cancers spontaneously are more associated with cell-mediated immune response. Some researchers showed that some tumors such as melanoma can recover spontaneously with a high number of lymphocyte infiltration in tumor tissue. However, there are conflict results regarding its effects on the immune system of cancer pathogenesis in the literature.26,27 In our study, patients with atypical MBC present significant superior rates of RFS, which is not previously reported in the literature. We thought it was due to less tumor growth and angiogenesis with fewer lymphocytes, and mononuclear infiltration in atypical MBC. In the literature, it was shown that inflammatory cells may affect tumor growth with the release of angiogenetic and proteolytic enzymes and cofactors.28-30 Therefore, patients with typical MBC had poor prognosis in our outcomes similarly to Rakha et al24 outcomes. We demonstrated that negativity of PR and small size tumors had a statistically favorable prognostic effect on RFS and OS in MBC patients. The results of our study were similar to other studies in the literature.9,18,20 When we posed the question on why PR negative tumors had a longer survival effect, we found in the literature that triple negative tumors, especially PR negative tumors in MBC, were associated with BRCA1 mutation carriers. BRCA1 mutations were found in 12-13% of patients with a positive history of breast cancer in first degree relatives, those who were diagnosed less than 35 years of age and patients with breast cancer in synchronous or metachronous contralateral breast. Occurrence of breast cancer in BRCA1 mutation carriers also tend to lack PR and Her2/neu receptors, with heterogeneous tumor structures and has poor prognoses than cancers linked to BRCA2 mutation. According to some studies, BRCA1 mutation carriers were more likely to have ER-negative breast cancers.28,31,32 We found that PR negative rates were high (72.7%), and we observed that this situation does not represent a poor prognostic factor. Hence, we considered that the cancer of our patients was not associated with BRCA1 mutation.
Our study has several limitations. First, since this is a multicentre study, pathology samples were evaluated by different pathologists. Because of this issue, subtyping of MBC histopathology could have prevented an optimal diagnosis. It would have been preferable to have all samples be assessed by only one pathologist within certain norms Ridolfi’s17 or Pederson’s.33 Second, we did not conduct any further genetic evaluation in this study. If we could have carried out analysis for BRCA1-2, p-53 mutation, we would be able to discuss more accurate and more objective results regarding the clinical differences between BRCA1 and non-BRCA1 associated with tumors in MBC patients.
In conclusion, the patients with MBC were mostly diagnosed in early stages in Turkey. Although pathological characteristics (such as HR negativity, triple negative, high grade tumor) were determined as less favorable, patients with MBC have longer survival rates in our country. It is detected that good prognosis was observed in PR negative and small tumor size groups among patients with MBC. There may be a relationship between the PR negative tumor and BRCA1 mutation analysis. There is probably lower incidence of BRCA1 mutation in our region, because BRCA1 mutation probability is higher in PR negative MBC. Further studies are needed which would also include BRCA1-2 mutational analysis.
References
* References should be primary source and numbered in the order in which they appear in the text. At the end of the article the full list of references should follow the Vancouver style.
* Unpublished data and personal communications should be cited only in the text, not as a formal reference.
* The author is responsible for the accuracy and completeness of references and for their correct textual citation.
* When a citation is referred to in the text by name, the accompanying reference must be from the original source.
* Upon acceptance of a paper all authors must be able to provide the full paper for each reference cited upon request at any time up to publication.
* Only 1-2 up to date references should be used for each particular point in the text.
Sample references are available from: http://www.nlm.nih.gov/bsd/uniform_requirements.html
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received September 2, 2016.
- Accepted November 9, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.