


Abstract
Objectives: To examine the impairments, activity limitations, and participation restrictions in children with spastic unilateral and bilateral cerebral palsy (CP). We investigated the relationship between these factors according to the international classification of functioning, disability, and health (ICF) model.
Methods: This prospective cross sectional study included 60 children aged between 4-18 years with spastic CP (30 unilateral, 30 bilateral involvement) classified as Levels I and II on the gross motor function classification system. Children had been referred to the Pediatric Rehabilitation Unit in the Department of Physiotherapy and Rehabilitation, Hacettepe University, Ankara, Turkey between March 2014 and March 2015. The Physician Rating scale was used to assess body functions and structures. The Gillette Functional Assessment Questionnaire 22-item skill set, Pediatric Functional Independence Measure, and Pediatric Outcomes Data Collection Instrument were used to assess activity and participation levels.
Results: There was a significant positive correlation between impairments and activity limitations (r=0.558; p=0.000), as well as between activity limitations and participation restrictions (r=0.354, p=0.005).
Conclusion: These results show that activity limitations in children with unilateral and bilateral ambulatory CP may be related to their impairments and participation restrictions, although the sample size of our study is not large enough for generalizations. Overall, our study highlights the need for up-to-date, practical evaluation methods according to the ICF model.
Cerebral palsy (CP) is a non-progressive disorder caused by damage to cerebral structures during prenatal, natal, or postnatal periods. The lesion causes a group of disorders and activity limitations in movement and posture.1 Alongside the commonly used clinical classifications, the Surveillance of Cerebral Palsy in Europe classifies CP into 3 major groups: spastic, ataxic, and dyskinetic.2 Subtypes of spastic CP can be further classified as either unilateral or bilateral.2,3 Facilitation of ambulation in children with CP is crucial for maintaining activity and participation, and a main goal of treatment is thus to enable the restoration, maintenance, and improvement of ambulation.4 However, positioning of the pelvis, trunk, and lower extremities, while walking against gravity may not be typical in children with CP. For example, a child with spastic diplegia usually raises the upper limb high or overextends the upper body to compensate for the lack of antigravity. The anterior tilt of the pelvis can be excessive due to improper control of muscles that are attached to the pelvis. Forward tilting of the pelvis leads to limitation of movement of the hip or knee joints, such as adduction and flexion during walking. Overall, an impaired posture control mechanism is a major problem that can disturb the independent development of daily living activities in these children.5 According to the International Classification of Functioning Disability and Health (ICF) model prepared by the World Health Organization, body structure, activity, and participation are linked to personal and environmental factors. The ICF Child and Youth version (ICF-CY) is geared towards children and young adults. Its most important feature is that it is a classifier model instead of being hierarchical.6 For example, a person with limited functionality and activity might not encounter any problems in participation due to personal and environmental factors. The ICF model uses a standard classification that was established to evaluate previous studies and to direct new clinical studies.6 This classification consists of Section 1) body structure and functions, activity (completion of an action or a task by the person), and participation (participation in daily life), and Section 2) personal and environmental factors. These components interact with each other in a complex manner.7 Assessing the positive and negative correlations of function, activity, and participation together with the goal set, while also considering the child and parents’ expectations will enable versatile rehabilitation programs to be constructed to meet the objective.6,7 The purpose of this study was therefore, to examine impairments, activity limitations, and participation restrictions by CP subtypes (unilateral and bilateral), by classification systems, Gross Motor Function Classification System (GMFCS), and Manual Ability Classification System (MACS), and to determine their relationships according to the ICF model in children with spastic unilateral and bilateral ambulatory CP, and also to assess the relationship of these ICF constructs with each other.
Methods
This prospective cross-sectional study was conducted with children aged between 4-18 years, who were referred to the Pediatric Rehabilitation Unit in the Department of Physiotherapy and Rehabilitation, Hacettepe University, Ankara, Turkey, between March 2014 and March 2015. Children had been diagnosed with spastic unilateral or bilateral CP, were at Level I or II of the GMFCS Expanded and Revised (GMFCS E&R), had not undergone any surgery on the lower extremities or received Botulinum Toxin treatment in the last 6 months, and had no behavioral problems were recruited. Only children with spastic type CP were selected, as this is the most common type of CP seen in the clinical settings. Unilateral spastic type refers to one side involvement of the body, while bilateral spastic CP may refer to the involvement of all extremities or lower extremities. In this study, bilateral CP cases only included children with lower extremity involvement CP. Children having other than the spastic type of CP and parents of children who did not volunteer to participate were excluded from the study.
Ethical approval was obtained from the Hacettepe University Non-interventional Clinical Researchs Ethics Board (GO 14/127). Informed consent was obtained from the families and informed assent from children older than 7 years of age. The study was performed in accordance to the Helsinki Declaration.
Demographic data, including name-surname, gender, diagnosis, clinical CP type, CP subtype, date and place of birth, height, weight, and contact data were recorded. Gross motor function classification was performed using the GMFCS E&R version translated into Turkish; evaluation was based on gross motor functions at 5 levels that range from unassisted walking with no hindrance to mandatory dependence on mobility devices. At Level I, children can generally walk without restrictions but tend to be limited in more advanced motor skills. At Level V, children are generally very limited in their ability to move around, even with the use of assistive technology. For each level, the GMFCS E&R defines gross motor functions for different age groups (<2, 2-4, 4-6, 6-12, 12-18 years), as motor functions vary with age.8 The GMFCS E&R includes an age band for youth 12 to 18 years of age and emphasizes the concepts inherent in the World Health Organization’s ICF. Turkish version of the GMFCS E&R was studied by El et al8 indicating excellent agreement with the overall weighted µ=0.86. High test-retest reliability was found intraclass correlation coefficien ([ICC]: 0.94 95% confidence interval) and the total agreement was 75% for test-retest reliability. The Turkish version of the E&R GMFCS was shown to be reliable and valid for assessment of Turkish CP children.8
Manual ability of children was classified according to the MACS. The validity and reliability study for the Turkish translation of MACS has been conducted by Akpınar et al.9 For the test-retest reliability, it ranged from 0.91-0.98. The inter-rater reliability of Turkish MACS was high, ranged from 0.89-0.96 among different professionals and parents. In the MACS, 5 levels are described. The scale is ordinal, with no intent that the distances between levels should be considered equal, or that children with CP are equally distributed across the 5 levels. Level I includes children with CP with, at most, minor limitations compared with typically developing children, which barely influence their performance of daily life tasks. Level V includes children unable to handle objects and with very limited ability to perform even simple actions.
Body structure and functions of the children during walking were evaluated using the Physician Rating scale (PRS), an observational gait analysis method where lower extremity joints are evaluated during walking by observations made from the sagittal plane.10 The PRS has high clinical applicability and consists of 3 evaluations: 1) Foot contact during gait (score of 0-4; 0: toe, 4: heel to toe), 2) recurvation of the knee (score of 0-2 scores; 0: recurvatum more than 5 degrees, 2: neutral, no recurvatum), and 3) the crouch angle (score of 0-3, 0: severe crouch, 3: none). It is possible to repeat the evaluation of relevant sections to determine the efficiency of the treatment. Scoring is between 0 (worst possible score) and 9 (best possible score) with separate scores for the left and right sides.10
The Gillette Functional Assessment Questionnaire (FAQ) 22-item skill set was utilized to evaluate activity levels. The FAQ 22-item skill set evaluates walking activities, such as walking while carrying an object and running, using a scoring system (very easy, a little difficult, very difficult, completely unable) to assess the ability to independently perform functional locomotor activities.11
The Functional Independence Measure for Children (WeeFIM) was used to assess activity and participation levels. The WeeFIM consists of 18 items divided into 6 sections (self-care, sphincter control, transfer, locomotion, communication, and social/cognitive skills). Each item is scored between 1 (low functional independence) and 7 (able to complete a task completely unaided, on time, and with confidence). The maximum attainable score of 126 signifies complete independence and the lowest possible score of 18 represents complete dependence.11 Activity and social participation was also evaluated using the Pediatrics Outcomes Data Collection Instrument (PODCI). The PODCI was developed by the American Academy of Orthopaedic Surgeons (AAOS) Outcomes Studies Committee. The validity and reliability of PODCI, which is a measure of activity and participation, was tested in relation to ICF in its native language.12 A validity and reliability study has also been conducted for the Turkish translation of PODCI in children with CP. Turkish PODCI study showed that the internal consistency was acceptable and test-retest reliability was quite high (Alpha=0.93, ICC=0.992). Findings of the validity of the scale indicated that it was highly sensitive in separating children with CP from healthy children (p<0.001). The scale could differ age groups, clinical types, and GMFCS groups only in the physical functioning domain (p<0.05). The correlations among subscales of 3 scales illustrated that the convergent validity was established while divergent validity was low. The Turkish version of PODCI is reliable and valid for assessing functional health and HRQL of children with CP.13 The PODCI has been translated into Turkish for use as a pediatric data collection tool and includes 2 different questionnaires for children and adolescents; a pediatric questionnaire that is completed by the caregiver, and an adolescent questionnaire that is completed separately by both the child and the caregiver. There are 5 major subsections that evaluate upper extremity functions, physical function and sports, transfer and basic mobility, pain, and happiness/satisfaction.13 Most items are scored on a scale of 1 (indicating the most positive response namely, “The activity is easy for the child”; “The child is very happy”; “The child never required help from another person”). Raw scores for each scale are converted to a standard score based on the mean of items that make up that scale. All items in a scale are first recalibrated so they are in the same metric, with a range of values from 0-5 for each item. Next the scores for all items comprising a scale are averaged over the number of items answered. The mean of the rescaled values is then multiplied by a constant so that each scale has a final range of values between 0-100. All standardized scores (range 0-100) are calculated in the worksheets, such as higher scores represent less disability and better functioning. A patient scoring above 50 on a particular scale is above the general population’s average, while a patient scoring below 50 on a scale is below the general, healthy population’s average. To compute the individual normative score requires knowledge of the general population mean (standardized) score and corresponding standard deviations.13 We used the Turkish version of the PODCI, which has been found to have a good validity and reliability for assessing activity limitation and social participation restrictions in children with CP.13
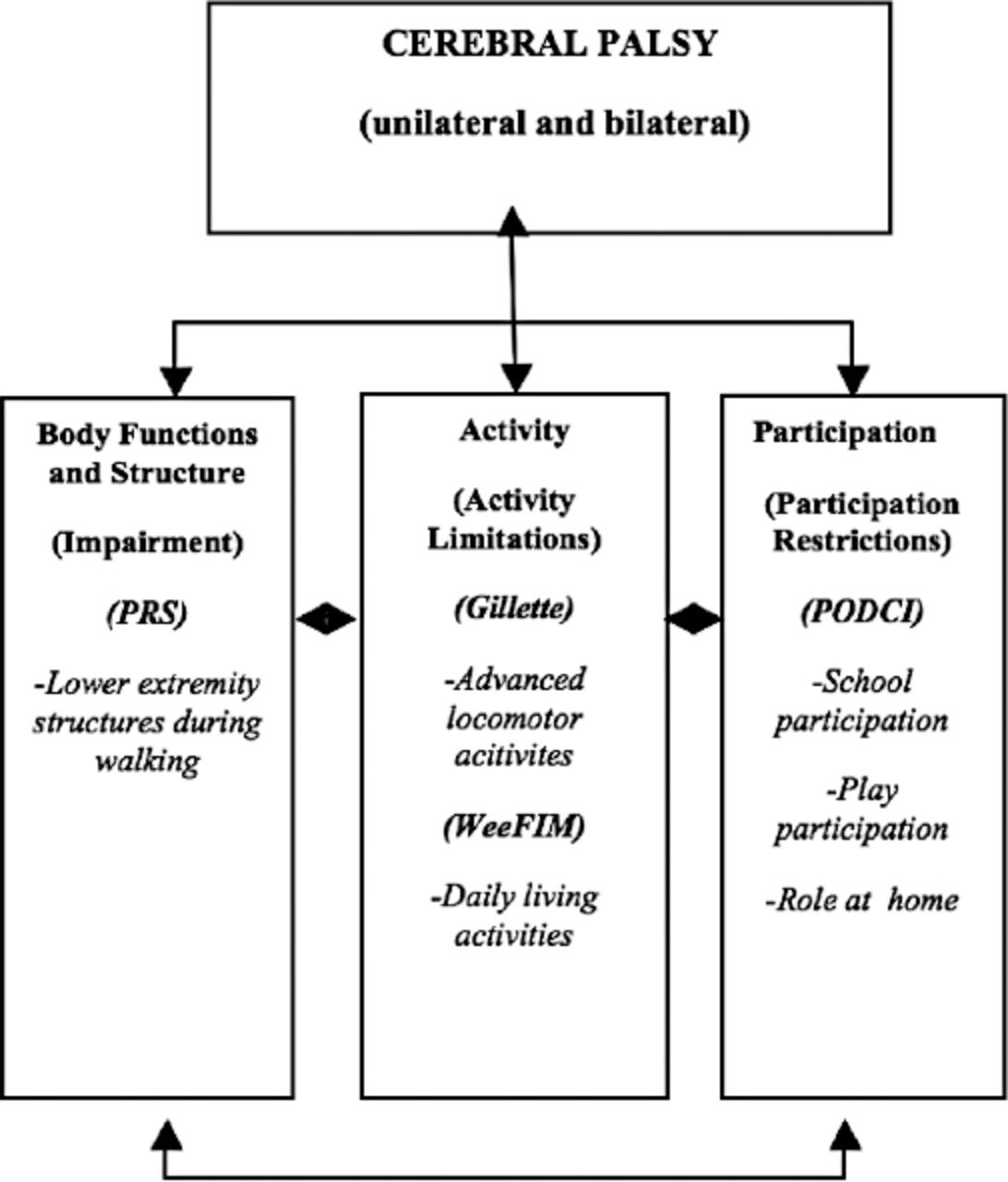
The relationship between the assessment methods and the ICF model is shown in Figure 1. The Statistical Package for Social Sciences version 18 (SPSS Inc., Chicago, IL, USA) was used for statistical analyses. In accordance with non-parametric methods, we used the Mann-Whitney U test for 2 independent groups and the Kruskal-Wallis H test for 3 or more independent groups when comparing measurement scores. Spearman’s correlation test was used to determine the degree, relationship, and significance of outcome measures, as the data were not normally distributed. Statistical significance was set at p=0.05.

Outcome measures linking international classification of functioning, disability, and health Model. PRS - Physician Rating Scale, Gillette - Gillette Functional Assessment Questionnaire 22-item skill set, WeeFIM - Functional Independence Measure for Children, PODCI - Pediatrics Outcomes Data Collection Instrument
Results
The extremity distribution was unilateral in 30 (50%) and bilateral in 30 (50%) participants. There were 39 (65%) males and 21 (35%) females, with a mean age of 9.5 ± 3.4 years. The GMFCS motor functional classification was level I in 33 (55%) and level II in 27 (45%) participants. The manual ability level of children was 31 (51.7%) for level I, 20 (33.3%) for level II, and 9 (15%) for level III.
Total participant scores for the body structure and function on the PRS differed significantly between unilateral and bilateral CP groups (U=141.000, Z=-4.600; p=0.000), whereby participants with bilateral CP had a poorer body structure and function than in the unilateral group. Total participant scores on the PRS also differed significantly between motor functional levels, GMFCS levels I and II (U=69.000, Z=-5.633, p=0.000) with significantly higher total PRS scores in level I. PRS scores also significantly differed between the manual ability, MACS groups (X2=6.984, df=2, p=0.030). Bonferroni-corrected dual comparisons indicated that the level III had significantly higher scores than the level I group. For the FAQ 22-item skill test, unilateral CP cases had significantly higher scores than in bilateral CP cases (U=267.500, Z=-2.702, p=0.007), and the GMFCS I group had significantly higher scores than in the GMFCS II group (U=144.000, Z=-4.487, p=0.000). There was no difference between the FAQ 22-item skill test scores when compared by MACS results (X2=5.507, df=2, p>0.05).
Total WeeFIM scores were significantly lower in the GMFCS II group than in the GMFCS I group (U=232.500, Z=-3.174, p=0.002), and there was also a significant difference between the total WeeFIM scores by MACS group (X2=11.971, df=2, p=0.003). Results of the Bonferroni-corrected dual comparison test indicated that the level II and level III had significantly lower scores than in the level I of MACS.
The PODCI participation scores were significantly higher in the GMFCS I group than in the GMFCS II group (U=256.500, Z=-2.811, p=0.005). No difference in the PODCI scores with relation to MACS level was detected (X2=5.516, df=2, p>0.05). All the impairments, activity limitations, and participation restrictions according to functional levels of children with CP are presented in Table 1.
Impairments, activity limitations, and participation restrictions according to functional levels of children with cerebral palsy (CP).
Total PRS and FAQ 22-item skill test scores showed a significant moderate, positive correlation (r=0.558; p=0.000). The FAQ 22- item skill test scores and total WeeFIM scores had a significant moderate, positive correlation (r=0.537, p=0.000). The FAQ 22-item skill test scores and total PODCI scores also had a significant moderate, positive correlation (r=0.604, p=0.000). A significant moderate, positive correlation was also found between the total of WeeFIM and PODCI scores (r=0.354, p=0.005) (Table 2). No significant correlation was found between total PRS, WeeFIM, and PODCI scores (p>0.05).
Relationship between impairments, activity limitations, and participation restrictions.
Discussion
The purpose of this study was to examine the impairments, activity limitations, and participation restrictions in 60 children with spastic unilateral and bilateral CP, using evaluation parameters that are in accordance with the ICF model. In our opinion, such studies enable medical staff, academics, and even individuals with CP and their relatives to utilize a common language and develop strategies according to the ICF models. Body structure, activity, and participation was evaluated by measuring lower extremity structure during gait function, gross motor skills/mobility/functional skills, and social roles for integration at home, school, and the society in general. Previous studies have shown that increasing the child’s participation is one of the most important goals of treatment.14-16 However, evaluation of activity and participation in clinical settings may provide an unrealistic image of capabilities in daily life, as this setting is isolated from environmental and personal factors.14-16 More recently, an emphasis has therefore been placed on the importance of targeting performance qualifiers in daily life to increase participation, rather than capacity qualifiers in clinical settings.4,5,11-16 This study, thus, only used scales that assess performance qualifiers.
The children with unilateral and bilateral CP included in this study were similar in terms of age, gender, height, and weight. Those diagnosed with unilateral CP had higher motor functional classification and GMFCS levels, and lower MACS levels than those diagnosed with bilateral CP. This replicates findings that motor function classification, GMFCS levels were higher in unilateral CP in a study conducted with 639 subjects.14 Similarly, Damiano et al15 found that patients with unilateral CP had better lower extremity functions and gait, while patients with bilateral CP had better upper extremity functions. In GMFCS Level II, the group with unilateral CP walked faster (p=0.017), scored 6.6 points higher on Dimension E of the Gross Motor Function Measure (p=0.017), 6.7 points lower on Upper Extremity subscale of the Pediatric Outcomes Data Collection Instrument, and 9.1 points lower on WeeFIM self-care (p=0.002). Kerr et al16 found unilateral cases to have significantly more developed gross motor functions in comparison with bilateral cases. Similarly, we found that children with bilateral CP, in whom lower extremities are more affected, had better upper limb functional abilities, while those with unilateral CP, in which only one side is affected, had better gross motor skills.
The motor functional classification GMFCS levels showed as statistically significant according to extremity distribution in children with CP in our study. We chose to only investigate unilateral and bilateral spastic types, as they are the most common type of CP and it allows us to investigate ambulatory differences of ICF parameters (the ability to walk unassisted is rare in quadriparetic and triparetic subjects). However, future studies may wish to include larger sample sizes and different CP types. For example, Gorter et al14 examined the functional level and motor impairment in various types of CP in 639 subjects aged 1-13 years: 500 spastic, 39 dyskinetic, 16 ataxic, 26 hypotonic, and 58 mixed type CP. Five hundred of these subjects were suffering from the spastic clinical type. As Gorter et al14 mentioned, the ability to walk unassisted is rare in quadriparetic and triparetic subjects. In addition, the unilateral and bilateral spastic type is the most common type of CP in the clinical setting. Ambulatory children of both type was selected to clarifying and comparing the differences and similarities, as well as investigating the relations of ICF parameters in between each other. We therefore included only ambulatory, unilateral, and bilateral subjects in the present study. But further studies may include larger sample sizes, such as Gorter et al14 to a better comparison of the datas. However, we excluded CP types other than the spastic CP from our study.
There are a variety of gait disorders in children suffering from CP, although these disorders present similar findings, making atypical classification is quite difficult. Gait patterns observed in unilateral and bilateral CP have been summarized by Rodda et al.17 However, the validity and reliability of gait classifications have been challenged by Dobson et al,18 who systematically reviewed 18 studies. The authors concluded that gait in the CP was mostly evaluated from the sagittal plane, while no classification included all deviations of gait in these children. In an investigation of 14 different gait disorders, Wren et al19 found that crouch and equinus were commonly seen in both bilateral and unilateral CP; 47% of unilateral and 74% of bilateral subjects walked in crouch, while 64% of unilateral and 58% of bilateral subjects walked in equinus. The recurvation rate was below 15% in both unilateral and bilateral subjects. Similarly, we found the crouch position in 50% of unilateral and 86% of bilateral CP cases. The higher crouch ratio in children with bilateral CP in our study compared with the Wren et al’s19 study, could be because what they called ‘elevated hip flexion disorder’ was classified as slight crouch in our study. Recurvation was present in 17% unilateral and in 12% bilateral CP in our study (and below 15% in both unilateral and bilateral subjects in Wren et al’s19 study). The first foot contact was made at the heels in 47% of the unilateral cases, decreasing to 5% in bilaterally involved children in our study. Fifty percent of bilateral CP cases made flat foot contact. We therefore, believe that flat foot contact might be associated with increased crouch rates in bilateral CP.
Maathius et al20 investigated the validity and reliability of PRS in 24 subjects with spastic CP consisting of 15 bilateral and 9 unilateral cases and found perfect intra observer reliability. We found that children with unilateral CP had significantly higher PRS scores than bilateral subjects. This may be related to limb topography; when only unilateral limbs are involved, subjects also have better GMFCS values with advanced gross motor abilities. Indeed, children in the motor functional classification of GMFCS I group had a significantly higher PRS scores than children in the GMFCS II group. A negative correlation was also found between PRS and MACS, which outlines the impairment during walking. Our study was conducted on bilaterally ambulatory children with CP, who do not have or have mild upper extremity involvement. Therefore a distribution between bilateral CP with mild upper extremity involvement with manual ability classification, MACS I and II levels, and unilateral CP with MACS I, II, and III levels were compared.
Numerous studies have demonstrated that children with CP have much lower activity levels than their peers. For instance, children with CP have been found to have significantly lower participation levels in school activities.21 No mention was made of the activity and participation differences among motor functional classification levels, GMFCS groups. Bjornson et al22,23 reported that children with CP had lower walking activity than healthy children. Longmuir et al24 found that the gross motor function, GMFCS group classification was significantly associated with walking activity. Cerebral palsy in children and young adults has also been associated with a sedentary lifestyle. Bjornson et al25 found that not only did children with CP have lower activity levels compared with healthy peers, but also that the activity level was related to the GMFCS group classification; daily walking activity and variability decreased as functional walking level (GMFCS level) decreased. Bagley et al26 investigated all 22 items of the FAQ 22-item skill test in children aged 4-18 years, and found that 13 were precise enough to differentiate between motor functional classification GMFCS groups I and II. However, they did differentiate between different types of CP. We also found a significant relationship between the FAQ 22-item skill test functional locomotor questionnaire and the GMFCS group value. This is because motor functional classification GMFCS is a measure of motor function in children with CP and the Gillette questionnaire directly outlines the mobility aspect of activity and participation. In addition, the FAQ 22-item skill test results were significantly different in unilateral and bilateral CP cases. We think that this difference was due to higher activity levels in the unilateral CP subjects.
We used the WeeFIM to evaluate activity and participation due to its compatibility with the ICF-CY. Our study showed a positive correlation between impairment, activity limitation, and participation of the ICF model. This replicates findings of Ko et al,27 who also investigated the correlation between activity and participation measures using the ICF-CY and the WeeFIM evaluation scale. Interestingly, the authors found activity and participation to be related to muscle strength and thickness, as well as other physical factors. Their results of ICF-CY evaluation for body function, activity, learning and application of knowledge, communication, and environmental factors showed a decline (p<0.05). Significant differences in the thickness of muscle was observed according to the GMFCS level, thickness of knee extensor and ankle extensor of cerebral palsy (p<0.05), and clauses of self-care, activity, mobility, ambulation, communication, and social acknowledgement (p<0.05). Study results showed negative correlation in the thickness of muscle, muscle strength, major motor function, daily activity and participation; the score of ICF-CY was shown to decline due to the high score for differences in the thickness of muscle, muscle strength, WeeFIM, and GMFM. The thickness and muscle strength of lower extremities affect main functions of the body and improvement of muscle strength of lower extremities may have positive effects on social standards, such as activity and participation of cerebral palsy.
Our study indicated positive correlation between impairment, activity limitation and participation of ICF model similar to Ko et al’s27 study. Song et al28 investigated the relationship between daily activities and physical and cognitive function in 68 children with CP. The WeeFIM scores were found to differ significantly according to the type of CP, whereby unilateral CP cases had significantly higher WeeFIM total scores than those with bilateral CP. However, we did not find such difference in the present study. This may be because all the children in our study were in GMFCS levels I or II and were ambulatory children. Song et al28 found no relationship between WeeFIM and physical function but the GMFCS groups of the children were not disclosed.
Manual ability of children was measured using the MACS. The MACS levels have previously been associated with function, activity, and participation,29 and our present findings support this; we found a significant relationship between the MACS level and activity-participation values (WeeFIM scale). We believe this is derived from self-care items, such as “eating” and “lower body dressing” for which the upper extremity is used, and “stair ascent/descent” of the WeeFIM scale, especially considering that GMFCS II children use handrails and that hand functions are directly involved with the locomotion items and lower mobility module.
Activity and social participation was also evaluated using the PODCI. Although the PODCI scale is suitable for detecting differences in physical functions and has been developed for children aged 2-18 years, a study by McCarthy et al30 suggests that it does not seem to be suitable for evaluating children aged 2-5 years. For example, the “too young for activity” option is classified as missing information. Children in the present study were aged 4-18 years, and we believe that the PODCI scores constituted a healthy data set. For reasons of consistency, all the children in our study were given the PODCI parent form to complete, even those over 11 years old. While Oeffinger et al,31 reported a significant difference between the PODCI adolescent and child forms, we had all subjects complete parent forms to establish a common ground and allow for an unbiased analysis. The PODCI parent forms have also been used in some other studies to differentiate between parents and children.32 Parents and adolescents agreed more on functioning (ICC=0.488-0.748) than health-related quality of life (ICC=0.242-0.568; PODCI).
There are findings that suggest that the GMFCS is a valid tool for estimating the participation of the child. In a study by Beckung and Hagberg,33 a relationship was found between the motor functional classification levels of the GMFCS and participation (consisting of mobility, education, and social relation parameters); participation, and especially its mobility aspect, was highly compatible with the GMFCS group. Although participation and the GMFCS group were found to be related, no comparison was made between participation and extremity distribution. We also found that participation (measured by the PODCI and WeeFIM) was related with the GMFCS group, whereby the GMFCS I children (a better functional level) had significantly higher participation levels than the GMFCS II group. Fauconnier et al34 evaluated social roles associated with participation in the daily life of children with CP and assessed major areas, such as self-care, school, and communication. While participation in daily life activities was associated with the assigned GMFCS group, it was not associated with extremity distribution. Similarly, we did not find any relationship between the children’s extremity distribution and participation
Our results indicate a significant relationship between activity and participation. Although it is difficult to distinctly separate measures that evaluate activity and participation, the Gillette (which relies heavily on activity), WeeFIM (which evaluates activity and participation), and PODCI (which relies more on participation) seem to have a moderate correlation. Sullivan et al32 investigated the relationship of functional data collection tools in children with CP who could walk, and found that the PODCI parent form scores and WeeFIM scores had a weak correlation. It is not necessarily surprising that these 3 measures do not have a strong correlation; the Gillette emphasizes the mobility aspect of activity and participation, the PODCI emphasizes health-related quality of life, and the WeeFIM emphasizes the self-care, mobility, and cognition aspects. Indeed, this is outlined in a systematic review by Harvey et al,35 which outlines 8 activity limitation evaluation methods used in 29 studies on children with CP. The fact that PODCI and WeeFIM evaluate activity and participation in different aspects results in the 2 complementing each other. These nuances should be taken into account when choosing a test battery.
Limitations
One limitation of our study is the need for advanced studies in which the relationship between walking functions, activity, and participation can be detected in patients with not only spastic CP, but also quadriparetic, dyskinetic, and ataxic CP types. In addition, the GMFCS groups III, IV, and V, which have more severe CP involvement, need to be evaluated with regards to their activity and participation levels and compared with subjects with milder CP involvement. Future studies should also replicate our findings using a larger sample size.
Contributions
Our data demonstrate that unilateral and bilateral involvement leads to differences in walking function, and activity and participation levels. The walking functions of patients with unilateral and bilateral ambulatory spastic CP affect the activity level, which in turn influences the participation level. These factors are therefore closely related. These differences can also depend on the body part that is more heavily involved, and future studies should recognize the fact that extremity distribution has an important effect on CP type. Within the framework of ICF, this study highlights the potential definition of treatment goals in long-term physiotherapy and rehabilitation programs by reporting the similarities and differences in function, activity, and participation levels.
We found that children with unilateral CP have better developed lower extremity body structure, gross motor levels, and activity levels during walking than children with bilateral CP. Unilateral CP patients also showed higher lower extremity participation parameters than those with bilateral CP. Bilateral CP patients had higher upper extremity participation parameters than those with unilateral CP.
In conclusion, these results show that activity limitations in children with unilateral and bilateral ambulatory CP may be related to their impairments and participation restrictions although the sample size of our study is not large enough for generalizations. Overall, our study highlights the need for up-to-date, practical evaluation methods that enable physiotherapists to evaluate body structure and function, and activity and participation levels in children with CP in accordance with the ICF model.
Saudi Medical Journal Online features
*Instructions to Authors
*Uniform Requirements
*STARD
*Free access to the Journal’s Current issue
*Future Contents
*Advertising and Subscription Information
All Subscribers have access to full text articles in HTML and
PDF format. Abstracts and Editorials are available to all
Online Guests free of charge.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received August 2, 2016.
- Accepted November 7, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}