


Abstract
Objectives: To investigate the incidence of parasitic infestations and inflammation accompanying parasitosis in a series of appendectomy cases.
Methods: Six-hundred-sixty patients who had undergone appendectomy in Bingöl State Hospital, Bingol, Turkey with the preliminary diagnosis of appendicitis between January 2012 and February 2015 were included in this retrospective study. They were retrospectively evaluated in terms of age, gender and pathological findings. Cases diagnosed with parasitic infestations were re-evaluated histopathologically for inflammatory response.
Results: The mean age was 19.6 years, and the male/female ratio was 1.8. When evaluated in terms of histopathological diagnoses, 573 (86.8%) were diagnosed as acute appendicitis, and parasitic infestation was identified in 12 (1.8%). Among cases with parasitic infestation, Enterobius vermicularis was identified in 9 (75%) and Taenia in 3 (25%) cases. Of cases with Enterobius vermicularis, 4 (44.4%) had lymphoid hyperplasia, 1 (11.1%) had normal-structured appendix vermiformis, and 4 (44.4%) had findings of acute appendicitis. All cases with taeniasis had an inflammatory response: acute appendicitis was identified in 2 (66%) and acute gangrenous appendicitis in 1 (33%) of them.
Conclusion: Parasitic infestations are among the probable causes in appendicitis etiology and should be kept in mind during differential diagnosis. However, whether every parasitic infestation leads to appendiceal inflammatory response is controversial.
Appendicitis is the most common cause of abdominal pain and one of the most common reasons for emergency gastrointestinal surgery.1-4 Appendicitis, which is generally seen in patients aged 10-30 years, is the most common cause of emergency abdominal surgery in children.5 Fecal stasis, fecaliths and lymphoid hyperplasia often take place in the etiology of appendicitis. Intestinal parasites, tumors, radiological studies in which barium is used, undigested vegetable residues and fruit seeds are also rarely identified in appendicitis etiology.4 Gastrointestinal system infections due to parasitic and protozoal infestations have various incidences throughout the world.2,4 Infection of the appendix itself by parasites is rare. The most common parasitic agents reported to be associated with appendicitis are Enterobius vermicularis, Schistosoma spp, Taenia spp and Ascaris lumbricoides.5,6 Studies involving large series of cases which have investigated the incidence of parasites in appendectomy specimens were reviewed, and this rate was determined to be 1.2%. Parasites have been reported to cause appendicitis by obstructing the lumen both without any acute inflammation and by creating an inflammatory reaction.4,7 However, the role of parasites in the pathogenesis of appendicitis has not been clearly identified yet.4,7 The aim of the current study was to determine the incidence of parasitic infections in the etiology of appendicitis and to investigate the relationship between parasitic infestations of the appendix and acute appendicitis.
Methods
A total of 660 patients who had undergone appendectomy in our hospital with the preliminary diagnosis of appendicitis between January 2012 and February 2015 were included in our study. We have no exclusion criteria for this study. The cases were retrospectively evaluated in terms of age, gender and pathological examination findings (Table 1). Cases were divided into 7 groups based on age. Distribution of cases according to age are summarized in Table 1. Within the rutin procedure in our hospital all specimens were fixated in 10% formalin and at least three samples were obtained, one longitudinally and 2 others transversely. The hematoxylin and eosin stained sections which belonged to cases diagnosed with parasitic infestation were re-examined by light microscopy for indications of parasitic infestation and inflammatory response.
Demographic and histopathological features of the cases (N=660).
The investigation protocol was in accordance with the Helsinki committee requirement and was approved by the institutional Ethical Committee of The General Secretary of Bingöl State Hospital.
Results
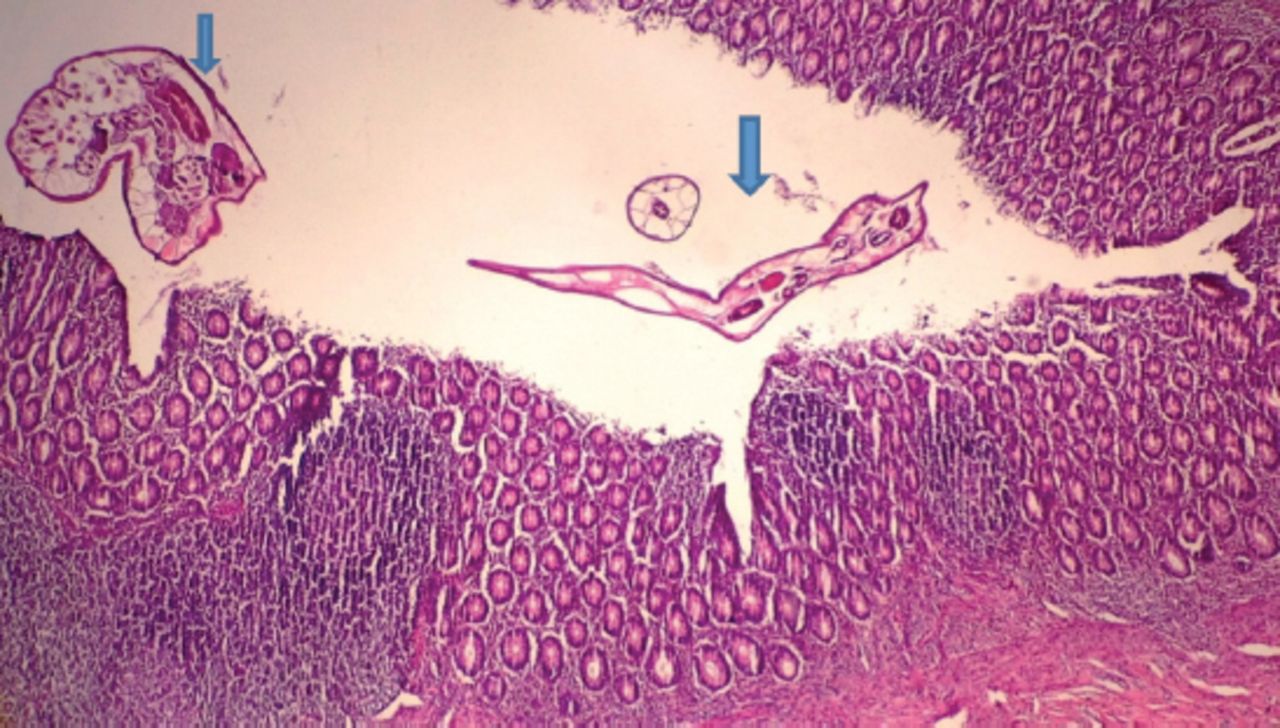
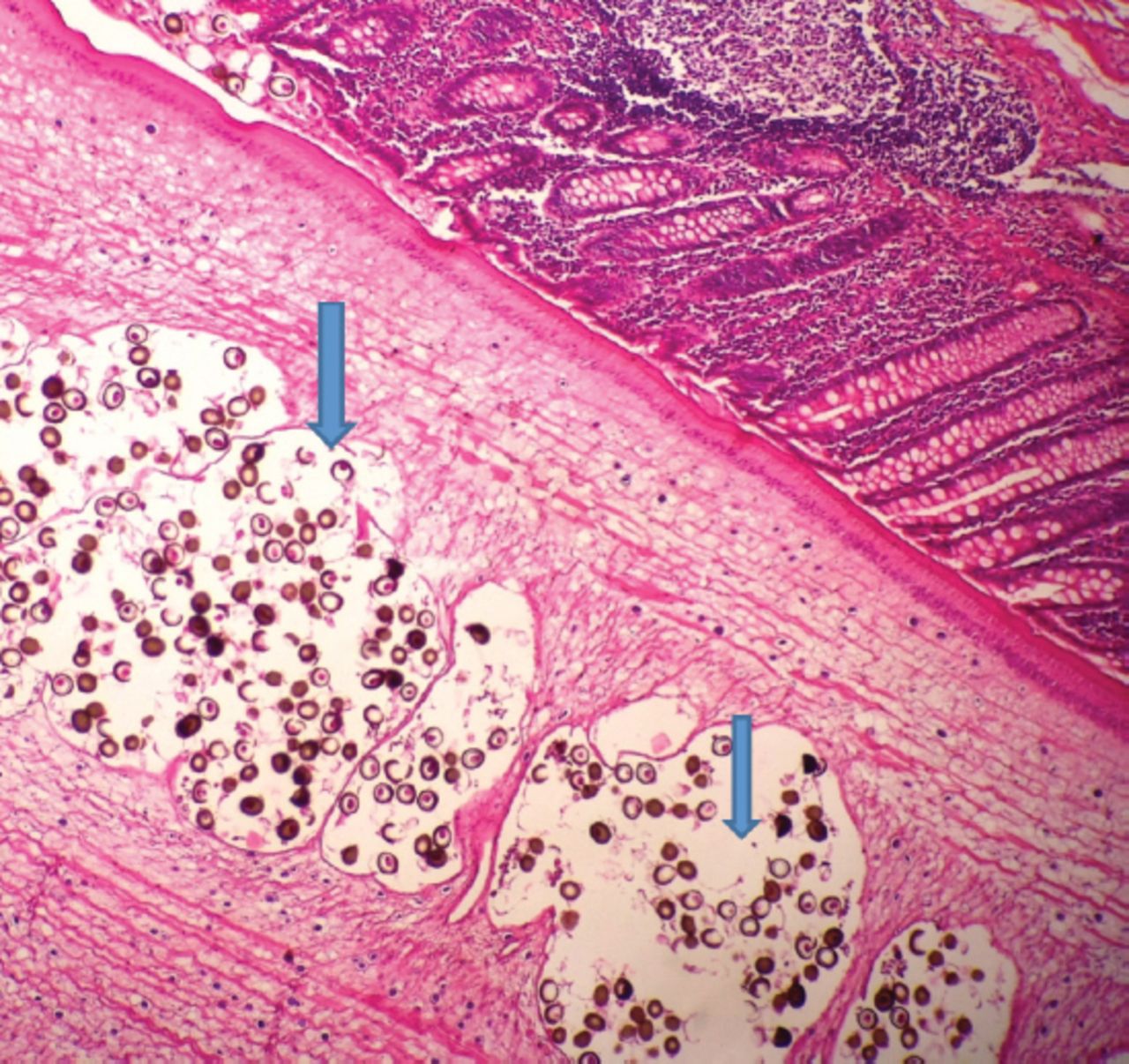
Of the 660 patients included in the study, 232 were female and 428 were male (male/female ratio: 1.8). When cases were analyzed in terms of age distribution, the highest number of cases was found in the 11–20 age range (43.8%). The smallest number of cases was in the >60 group. When our cases evaluated in terms of histopathological diagnoses, 573 cases (86.8%) were diagnosed as acute appendicitis, and parasitic infestation was present in only 12 (1.8%) cases. The mean age of patients with parasitic infestation was 14.8 years; 58% of them were female and 42% male. Among these cases (Table 2), 9 (75%) had Enterobius vermicularis (Figure 1) and 3 (25%) had Taenia (Figure 2). Of the cases with Enterobius vermicularis, 4 (44.4%) had lymphoid hyperplasia, one (11.1%) had normal-structured appendix vermiformis, and 4 (44.4%) had findings of acute appendicitis. All cases with taeniasis had an inflammatory response; acute appendicitis was identified in 2 (66%) and acute gangrenous appendicitis in one (33%). In all cases with parasitic infestation, either the parasite or its eggs were identified in the lumen of the appendix. No findings of intramural or intramucosal parasitosis were present.
Distribution of cases in which parasitic infestation was identified.

Structures consistent with lymphoid hyperplasia of the appendix and Enterobius vermicularis within the lumen (arrows) (40x, stained with hematoxylin and eosin)

Structures consistent with Taenia and its eggs within the lumen (arrows) (40x, stained with hematoxylin and eosin)
Discussion
Since Fitz first described the development of appendicitis due to acute inflammation in appendix vermiformis and proposed surgical excision in the majority of cases, numerous articles related to the etiology of appendicitis have been published.8,9 Fecal stasis, fecaliths and lymphoid hyperplasia often take place in the etiology of appendicitis. Other than these, intestinal parasites, tumors, radiological studies with barium and undigested vegetable residues and fruit seeds are also rarely identified in appendicitis etiology.4,10 Parasitic infestations can mask the clinical features of acute appendicitis. Radiological and laboratory findings are not helpful in preoperatively distinguishing acute appendicitis related to parasites.7 The incidence of acute appendicitis is 8.6% for males and 6.7% in females, reaching its peak in the second and third decades.3 Appendicitis is relatively more common in young males when compared to females; our study revealed similar results.3
Parasites can lead to appendicitis by obstructing the lumen or by causing secondary inflammation.10 In parasitosis, findings of acute inflammation may not be present in the appendiceal wall in histopathological examination of the appendix.7,11 Regarding the histopathological examination of appendectomies related to parasitic infestations, absence of histological findings of acute appendicitis was reported at rates of 25% in a study by Karatepe et al10 and 52.7% in a study by İlhan et al.11 In a study by Thanikachalam et al. conducted on 100 cases, parasitic infestation was found in 16 cases; in 13 out of these 16 cases (81%), findings of acute appendicitis were present.5 In a study by Zakaria et al,2 parasitic infestation was observed in 88 of 1600 appendectomy specimens, and findings of appendicitis were present in 54 of the 88 cases (61%). In cases with no evidence of inflammation in the appendiceal wall, lymphoid hyperplasia, luminal obstruction or hypersensitivity reaction occurring in the appendiceal wall have been suggested to be associated with the onset of symptoms.7 However, some publications have mentioned that findings of inflammation might have occurred with settlement of the parasite into the appendiceal wall, or the parasite might have been incidentally discovered within the lumen of an inflamed appendix during surgery.7,10
Enterobius vermicularis is the most commonly identified parasitic agent in the gastrointestinal system4,12 While Enterobius vermicularis infestation has a higher prevalence in developing and tropical countries, it has been identified at rates of 4-28% in pediatric populations around the world.2 The relationship of appendicitis with this parasite, which is most frequently located in the ileum and cecum, was first shown in 1988.13 Enterobius vermicularis is also the most commonly identified parasite within the appendix.4,11 In various studies, Enterobius vermicularis has been identified within the appendix with incidences between 0.5% and 3.8%.2,4,12 In the literature, the rate of inflammation occurring in appendixes in which Enterobius vermicularis was identified varies widely. In a study by Yabanoğlu et al of 1452 cases, parasitic infestation was identified in 17 (1.17%) of the cases, and Enterobius vermicularis was observed in 15 (88%) of these. In 80% of the samples with Enterobius vermicularis, normal appendiceal tissue was present.4 In the study by Zakaria et al in which they included 51815 appendectomy cases published in the literature between 1957 and 2002, 2308 cases were determined to have Enterobius vermicularis infestation, and findings of inflammation were found in only 12% of them.2 In our series, while acute appendicitis occurred in 44.4% of the cases in which Enterobius vermicularis was observed, 55.6% of cases exhibited normal appendix vermiformis and lymphoid hyperplasia. These findings suggest that Enterobius vermicularis might have been incidentally identified in the appendix rather than being a causal factor for appendicitis. After ingestion of meat infected with larvae of Taenia, also known as tapeworm, the larvae cling to the wall of the small intestine using suckers on the head, or scolex, and the infection is initiated. The parasite passes through the intestinal wall, enters the venules, and then moves into the systemic circulation.14 Although Taenia is known to reach organs such as the liver, lungs, brain and eyes by systemic circulation, the manner by which it enters the appendix is not clear.15,16 The diagnosis of taeniasis is made by identification of the parasite itself or its eggs. Taenia eggs are spherical and 30-40 µm in diameter.14 The eggs of Taenia solium and Taenia saginata are similar in appearance. Thus, to distinguish the species of eggs histopathologically is very difficult.16 Taenia infestation of the appendix is rare.3,14,16 In a study in which 1600 appendectomy specimens were investigated,24 (1.5%) had parasitic infestation, and in only one of these was taeniasis observed.17 In the literature, the incidence of taeniasis within the appendix is reported to be between 0.01 and 0.31.2,6,11,18 In a study by Eğilmez et al19 of 847 cases, parasitic infestation was identified in 83 (9.8%) of the cases, and taeniasis was observed in 38 (45,8%) of these. In 55% of the samples with taeniasis, normal appendiceal tissue was present.19 In our series, taeniasis was present in 0.5% of the cases, all of which showed an inflammatory response in the appendix. In the literature, the rates of parasitosis occurring in normal appendix tissue were determined to be 41% and appendicitis 59%, in patients undergoing appendectomy; no significant difference was found between these 2 rates (Table 1). Evaluation of our results together with data from the literature suggests that parasites might not be the primary cause in appendicitis etiology.
Study limitation
The number of cases is not large enough. Furthermore, we had limited urban/village diversity within our population. This could have limited the differences between the urban and non urban populations.
Parasitic infestations are among the probable causes in the etiology of appendicitis and should be kept in mind during differential diagnosis. However, whether every parasitic infestation leads to an inflammatory response in the appendix is controversial.11,20 Review of the literature shows that the rates of inflammatory response and normal-structured appendix accompanying parasitic infestation are similar (Table 3). Parasitic infestations may still be a minor cause of acute appendicitis, but the number of cases is not large enough to establish a significant relationship. In order to avoid the surgical side effects associated with negative laparotomy, patients complaining of abdominal pain should be examined for intestinal parasites. Patients whose medical history as well as clinical and laboratory findings are positive should then be evaluated more carefully. If parasitosis is identified in the histopathological examination, anti-parasitic treatment is indicated following appendectomy.
Student Corner
We invite students from a variety of medical disciplines to submit original contributions based on their supervised research.
The Student Corner of Saudi Med J aims to help students explore research opportunities and network with other peers and mentors in the same field.
Submission Guidelines
Submitted Abstracts should include the following:
Title should be descriptive
Author’s names and affiliation(specify college level/year, academic degree of Senior Author)
Abstract must be structured and not more than 300 words
The following are the typical headings:
Objectives (background, why the study was done, specific aims)
Methods (setting, date of study, design, subjects, intervention and analysis)
Results (findings, data and statistical tests) and
Conclusion (general interpretation of results)
General Information on Abstract Submission
Submitted Abstracts should be co-authored by a Senior Supervisor
Abstracts will be reviewed by Student’s Corner Section Editor
There is no fee to submit an Abstract
Ethical Approval should be provided
Non-indexed materials
- Received October 18, 2016.
- Accepted November 7, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.