


Abstract
Nasal septal surgery is one of the most common otolaryngology procedures performed, with rare occurrences of major postoperative complications. Oronasal fistula is a rare complication of septal surgery, with only few cases being reported in the literature. It is commonly caused by a congenital cleft palate, cleft palate surgery, traumatic injuries, infections, or neoplasms; however, it does not usually occur post-septal surgery. Here, we report the case of a 55-year-old male who presented with a symptomatic oronasal fistula post-septoplasty. Unlike other reported cases, there were no features of underlying palatal pathologies, and no previous history of other nasal or oral procedures. We described a multilayer surgical closure technique that was utilized in this case, with no recurrence seen during a 6-month follow-up period. Additionally, we reviewed the other 3 reported cases of this complication, and discussed the possible etiology in this case.
Septal surgery is one of the most commonly performed otolaryngologic operations.1-3 It is primarily indicated to improve the nasal airway in patients presenting with nasal obstruction due to a deviated nasal septum.1-3 Various surgical techniques have been described in the literature, including submucosal resection (SMR), conventional septoplasty, and more recently, endoscopic septoplasty.1-3 The most common complications of septal surgeries include the persistence of nasal obstruction, bleeding, septal hematoma, and septal perforation.4 Rare complications include saddle nose deformities, cerebrospinal fluid rhinorrhea, and ocular complications;4 however, an oronasal fistula is one of the rarest complications of septal surgery.5 It is most commonly caused by a congenital cleft palate, cleft palate surgery, traumatic injuries, infections, or neoplasms.5 The main complaints associated with an oronasal fistula and necessitating early surgical repair are nasal regurgitation and hypernasality.6 Here, we present the case of an oronasal fistula as a complication of septal surgery, without any previous underlying palatal pathology. The aim of presenting this rare complication was to highlight the possible causes and available surgical approaches, and to increase awareness among the general otolaryngology community.
Case Report
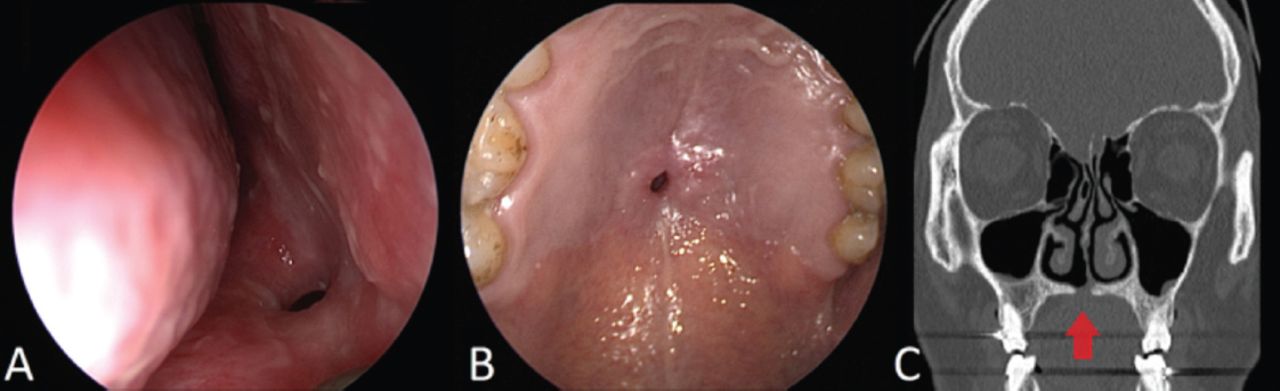
A 55-year-old gentleman presented with a history of nasal regurgitation and hyper-nasality post-septoplasty. The original surgery was carried out in another institute under general anesthesia 2 months prior to his presentation to our clinic. The fistula was unnoticed intra-operatively, and the patient’s symptoms began on the third postoperative day, after which he underwent multiple failed attempts at closure under local anesthesia at the other institution. He denied having any other nasal or oral procedures in the past, and had not been treated for any infections in the same area. The in-office examination revealed a 3-mm oronasal fistula starting just off the midline on the right side of the hard palate, and ending in the right nasal floor adjacent to the mid-septum (Figures 1A-1B). There were no signs of a submucosal cleft palate, cleft palate, high arched palate, cleft lip, ulceration, or any current or reported previous infections in the area. A noncontrasted CT scan of the paranasal sinuses was performed, and showed a bony defect in the hard palate corresponding to the site of the oronasal fistula, as seen on the clinical examination, and an absence of the majority of the vomer bone posteriorly (Figure 1C).

Oronasal fistula during the endoscopic examination of the A) right nasal cavity and B) examination of the oral cavity. C) Coronal CT scan of the paranasal sinuses showing a bony defect in the hard palate connecting the right nasal cavity to the oral cavity (arrow).
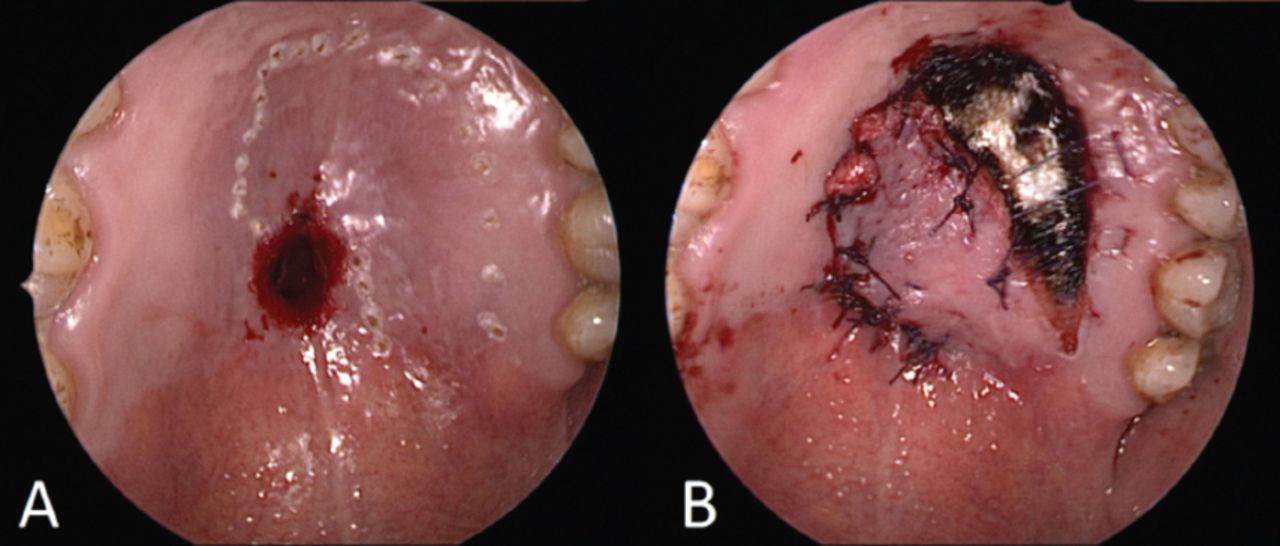
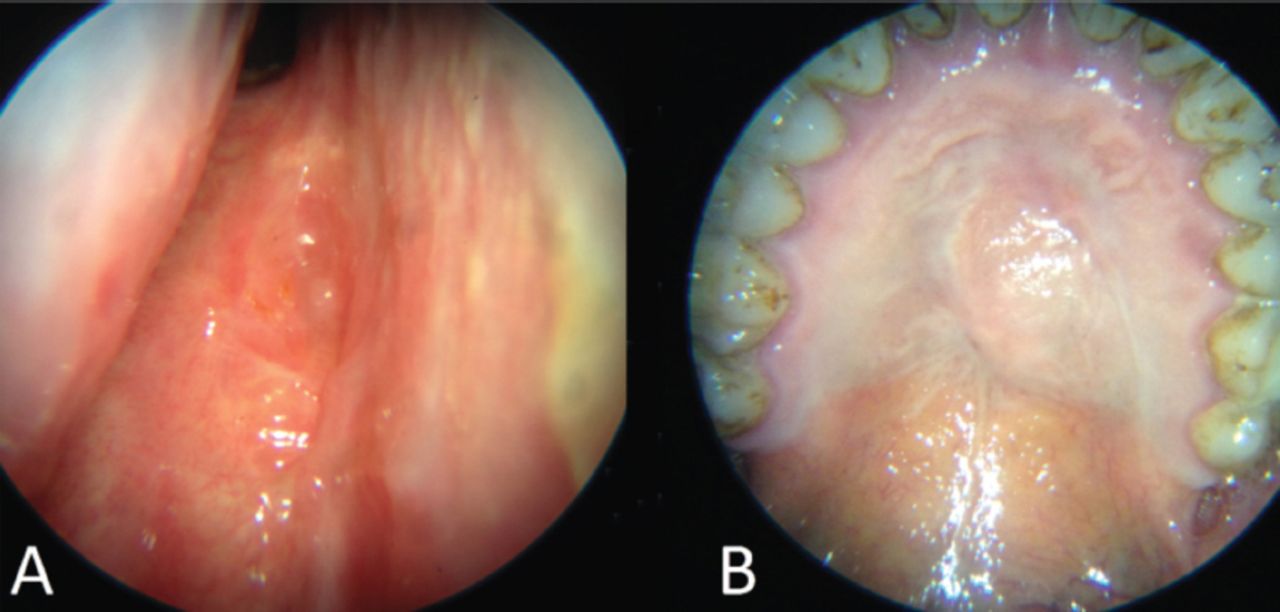
He underwent a surgical repair of the oronasal fistula using multilayer reconstruction under a general anesthetic. Initially, the fistula tract was resected transorally and transnasally utilizing nasal endoscopy. Then, a palatal mucoperiosteal flap was raised on the left based on the greater palatine vessels. Irradiated fascia lata Tutoplast® (RTI Surgical, Inc., USA) was placed as the first layer covering the fistula on the oral side, and the mucoperiosteal flap was rotated and advanced as the second layer. The flap was sutured to the surrounding mucosa with absorbable sutures, followed by the application of BioGlue® (CryoLife, Inc., USA) over the flap to further support and seal the reconstruction (Figure 2). The nasal surface of the fistula was also reconstructed using a free mucosal graft harvested from the left nasal cavity floor, after removing the mucosa surrounding the fistula site on the nasal aspect. The intraoperative endoscopic examination of the surrounding area revealed the absence of a large portion of the bony vomer, with intact mucosa. The nasal reconstruction was also held in place with BioGlue® and absorbable packing. During the 6-month postoperative follow-up period, this patient’s symptoms resolved, with no evidence of recurrence upon examination (Figure 3).
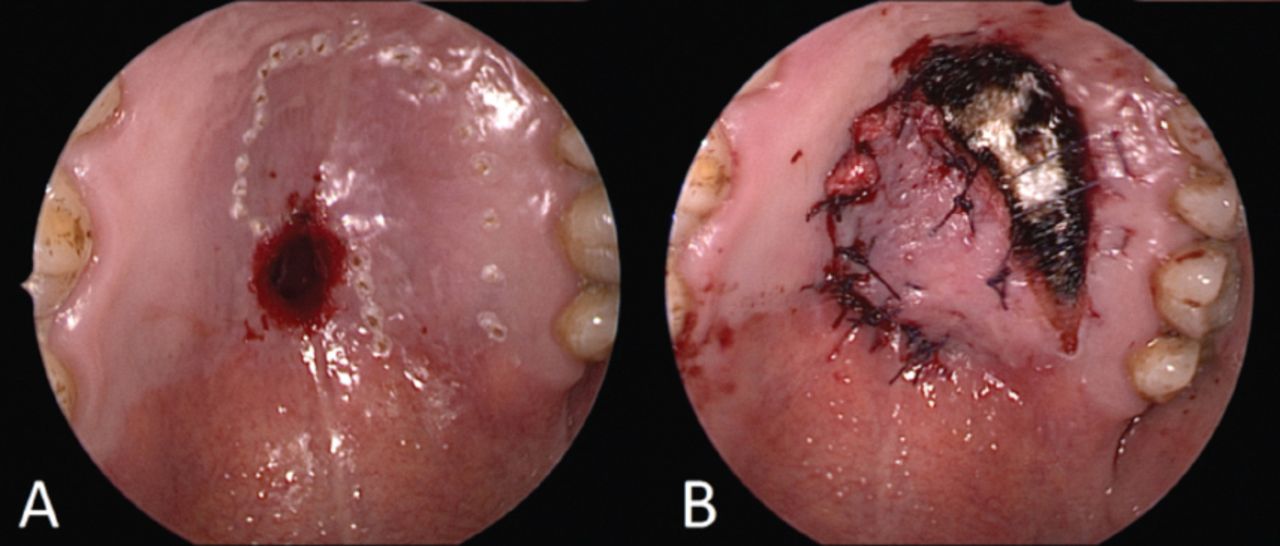
Photography showing A) Cautery marking of the rotational mucoperiosteal flap based on the greater palatine vessels. B) Mucoperiosteal flap sutured in place.

Six-month postoperative appearance of both sides of the reconstruction [A) nasal side and B) palatal side] showing the disappearance of the oronasal fistula.
Discussion
An oronasal fistula is a pathological defect that connects the nasal and oral cavities.6 It is considered to be one of the rarest complications of septal surgery. Upon reviewing the literature, only 3 cases of this complication have been previously reported. Thompson et al5 described the case of an oronasal fistula in a patient who underwent septal surgery complicated by a fungal infection. Four months postoperatively, the patient showed signs of swelling and ulceration at the midline of the hard palate, which progressed within 8 months to a complete palatal perforation.5 A biopsy from the ulcerative edges confirmed the presence of candida albicans.5 A repeated biopsy after 3 months of oral antifungal therapy was negative for fungus. The patient then underwent a successful surgical repair of the defect with an oral mucosal flap.5 Ersoy et al7 presented a case with a palatal fistula of the hard palate immediately after septal surgery in a patient with an undiagnosed submucosal cleft palate. The fistula was repaired successfully using 2 vascular layers composed of a nasal mucosal flap for the nasal layer, and a rotational mucoperiosteal flap from the oral cavity for the oral layer, with no recurrence.7 Gökdemir et al8 reported the third case of a palatal perforation immediately after septal surgery in a patient with a high arched palate, which was repaired using mucoperiosteal flaps to cover the nasal and oral parts of the defect.
In contrast to the other case reports, no underlying palatal abnormality or pathology was present in our case. We presume that this unusual complication was the result of a vigorous resection of the maxillary and palatine crests of the nasal septum, with the possible use of an osteotome angled inferiorly. We also believe that this was overlooked intra-operatively due to the narrow and bloody surgical field of view posteriorly in a routine septoplasty. This could have been prevented with use of rigid nasal endoscopy to optimize the visualization in that area.
Various techniques have been described to repair a palatal fistula, depending on its site and location.9 To decrease the risk of recurrence, the closure is most commonly performed with 2 vascularized mucosal layers, with the nasal layer being closed by a nasal mucosal flap and the oral layer being closed by mucoperiosteal transposition flap.9 Murrell et al10 described a 3-layer closure of oronasal fistulas consisting of a septal mucosal flap, bone or cartilage graft, and palatal mucosal flap, with no recurrence after one year of follow-up. We utilized a similar surgical technique with 3 layers for the closure of the defect. It consisted of a free nasal mucosal graft, an irradiated fascia lata allograft (Tutoplast®), and a rotational mucoperiosteal flap from the oral cavity adjacent to the fistula. Our results showed good healing with no recurrence of the fistula or symptoms after a 6-month follow up period.
In conclusion, an oronasal fistula is an unusual complication of septal surgery. Care should be taken preoperatively to identify those patients at risk, including patients with a high arched palate or a submucosal cleft palate. Any resection of the deviated bony maxillary and palatine crests in high risk patients during septal surgery should be attempted under direct vision, with great care. Endoscopic visualization may help in preventing such a complication during septoplasty, especially when dealing with posterior deviations of the nasal septum. Early identification and surgical repair are important to reduce the negative impact of an oronasal fistula on the patient’s quality of life. Moreover, a 3-layer repair can be utilized for the closure of an oronasal fistula, with a low recurrence rate.
Clinical Practice Guidelines
Clinical Practice Guidelines must include a short abstract. There should be an Introduction section addressing the objective in producing the guideline, what the guideline is about and who will benefit from the guideline. It should describe the population, conditions, health care setting and clinical management/diagnostic test. Authors should adequately describe the methods used to collect and analyze evidence, recommendations and validation. If it is adapted, authors should include the source, how, and why it is adapted? The guidelines should include not more than 50 references, 2-4 illustrations/tables, and an algorithm.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 8, 2016.
- Accepted November 16, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.