


Abstract
Objectives: To assess urine neutrophil gelatinase-associated lipocalin (uNGAL) level as a potential predictor of acute kidney injury (AKI), and both intensive care unit (ICU) and in-hospital mortality.
Methods: Patients presenting to our ICU with a systolic blood pressure (SBP) <90 mmHg or mean arterial pressure (MAP) <65 mmHg, and no prior kidney disease were followed prospectively. Baseline data were collected on patient demographics, admission diagnosis, APACHE II and SOFA scores, SBP, MAP, serum creatinine and cystatin C, and uNGAL. Patients were monitored throughout hospitalization, including daily uNGAL, serum creatinine and cystatin C, and continuous MAP. Bivariate analysis compared those dying in the ICU and in-hospital versus survivors; with hierarchical binary logistic regression used to identify predictors of mortality. Areas under receiver-operating-characteristic curves (AUC) were used to measure sensitivity and specificity at different uNGAL thresholds.
Results: Among 75 patients followed, 16 died in the ICU, and another 24 prior to hospital discharge. Mortality rates were greatest in trauma and sepsis patients. The ICU survivors differed from non-survivors in almost all clinical variables; but only 2 predicted ICU mortality on multivariate analysis: day one uNGAL (p=0.01) and 24-hour APACHE II score (p=0.07). Only the APACHE II score significantly predicted in-hospital mortality (p=0.003). The AUC for day one uNGAL was greater for ICU (AUC=0.85) than in-hospital mortality (AUC=0.74).
Conclusions: Day one uNGAL is a highly accurate predictor of ICU, but less so for in-hospital mortality.
Whether the result of severe illness or injury or recent surgery, patients who are critically ill have a very high rate of acute kidney injury (AKI),1-6 ranging from 5% to almost 90%, depending on the population studied.7,8 In one of the largest studies, Uchino et al5 analysed 29,269 patients admitted to critical care units at one of 54 hospitals in 23 countries between September 2000 and December 2001, and identified clinically-documented acute renal failure in 1738 (5.7%), among whom less than one third had previously-documented renal dysfunction. In another sizeable study in Japan, Isshiki et al9 ascertained that some major adverse kidney event had occurred in 102 (20.6%) of the 495 patients studied. Meanwhile, amongst 103 patients admitted to a single coronary care unit, Yang et al6 noted diagnosed acute renal failure in 49 (47.6%);6 while Camou et al10 detected AKI in 43 of 50 patients (86%) with sepsis admitted to a critical care unit. Outcomes in critically-ill patients who develop acute renal dysfunction are generally not good, with up to 60% dying prior to discharge,5 and chronic renal failure and the need for renal replacement therapy (RRT) are common outcomes among survivors.4,7-10
For several decades investigators have attempted to identify biomarkers that predict early AKI, so that aggressive kidney-sparing and life-saving treatment can be initiated earlier.11 Such biomarkers include tubular enzymes like alpha- and pi-glutathione S-transferase, N-acetyl-glucosaminidase, alkaline phosphatase, gamma-glutamyl transpeptidase, Ala-(Leu-Gly)-aminopeptidase, and fructose-1,6-biphosphatase); low-molecular weight urinary proteins like alpha1- and beta2-microglobulin, retinol-binding protein, adenosine deaminase-binding protein, and cystatin C; urinary interleukins/adhesion molecules; and markers of glomerular filtration like pro-atrial natriuretic peptide (1-98) and cystatin C; among others.11
Neutrophil gelatinase-associated lipocalin (NGAL) is a member of the lipocalin family of proteins that transport small hydrophobic molecules like steroids, retinoids, and lipids.12,13 Expressed by neutrophils and various epithelial cells, it has long been recognized as a marker of various disease states, beginning with its identification as an indicator of inflammation in patients with inflammatory bowel disease in 1996.14 For more than a decade, its use has grown to include the early detection of early AKI.15 Since then, it has been studied repeatedly to detect early AKI. This has included a variety of other clinical contexts,7 both in children and adults, like renal injury due to cancer,16,17 cancer chemotherapy,18-20 kidney surgery,21 kidney transplantation,22,23 cardiac surgery24-28 and systemic illness, especially sepsis.8,29-31 In an earlier paper, we assessed the role of urinary NGAL in the detection of AKI among critically-ill patients admitted to a large tertiary care intensive care unit (ICU) in Saudi Arabia. In this paper, given research documenting AKI as an independent predictor of mortality,32 we present out results assessing the value of urine levels of NGAL (uNGAL) for detecting both short-term and somewhat longer-term mortality in that same patient population.
Our specific objectives were 1) to determine and compare how well elevated uNGAL levels, at baseline and over the course of hospitalization, predict mortality, both in the ICU and afterwards prior to hospital discharge; 2) to determine if NGAL is a predictor of mortality independent of renal injury; and 3) to identify the threshold of uNGAL, in ng/mL that optimizes its diagnostic accuracy predicting death.
Methods
Because not all our patients were conscious at the time of admission, we were unable to obtain informed signed consent prior to the beginning of data collection, as per the Declaration of Helsinki. However, prior to any data collection, the protocol for this prospective cohort study had been approved by the institutional ethics review board of our hospital. Wherever possible, informed written consent was obtained from either the patient or their legal guardian.
For this study, we recruited a select cohort of patients consecutively admitted to the ICU at King Abdulaziz University Hospital in Jeddah, the second largest city in Saudi Arabia with a metropolitan area population of 3.5 million people, and the major referral center for all of Western Saudi Arabia. Eligibility criteria were age of at least 18 years, and either a systolic blood pressure less than 90 mm Hg or a mean arterial pressure (MAP) less than 65 mm Hg, thereby requiring the administration of at least one vasopressor, inotrope, or both. Patients were excluded if they had a serum creatinine >200 µµmol/L at presentation, had previously-documented end-stage renal disease (ESRD), were on dialysis, had documented obstructive uropathy, or were pregnant. Recruitment took place over a 13-month period from May 2012 to June 2013.
In addition to undergoing standard laboratory investigations, urine was collected and sent to measure uNGAL and serum cystatin C levels on the day of admission immediately upon arrival in the unit (time, t = 0), as well as at t = 6, 12, 24, and 36 hours, after which these levels were measured daily through day 4. Serum creatinine was measured by the hospital’s clinical laboratory at baseline, and then monitored as per standard ICU routine (namely, at least daily) throughout the ICU admission, as was urine output. Other variables that were measured to reflect the patient’s overall illness severity were the patient’s Acute Physiology and Chronic Health Evaluation, version 2 (APACHE II) and Sequential Organ Failure Assessment (SOFA) scores. As per standard ICU protocol, we also monitored each patient’s hemodynamic status, including MAP, any vasopressors and inotropic agents used, and their doses; fluid balance; need for mechanical ventilatory support; and need for RRT, including intermittent hemodialysis. Treatment was administered to protect the kidneys from further injury when the level of uNGAL was observed to start to increase, including attempts to optimize the patient’s MAP between 60 and 65 mm Hg to maintain adequate perfusion pressure, using judicious vasopressor doses to avoid vasoconstriction and worsening renal perfusion, avoiding nephrotoxic and contrast agents as much as possible, and initiating early continuous RRT within a few hours of AKI recognition if no response was apparent with optimized medical care. Both the KDIGO GL criteria and serum cystatin C level were used to define and stratify the severity of AKI. With the former, AKI is defined as an increase in sCr by ≥0.3 mg/dl within 48 hours or an increase in sCr to ≥ 1.5 times baseline within the first 7 days after transplantation. Furthermore, AKI is classified into 3 stages: Stage 1, sCr increase ≥0.3 mg/dl or an increase of 1.5-1.9 fold from baseline; Stage 2, sCr increase of 2-2.9 fold from baseline; Stage 3, sCr increase >3-fold from baseline, or an increase to ≥4.0 mg/dl, or the initiation of renal replacement therapy. With the latter, the following allocations were used, based on prior research results: cystatin C <100, normal; 100-499, mild injury; 500-999, moderate injury; ≥1000, severe injury.
Patient mortality, both in the ICU and prior to hospital discharge, was recorded.
Data analysis
The primary goal of bivariate analysis was to compare patients who died in the ICU versus survivors, and patients who died in hospital versus those who survived long enough to be discharged. Variables of interest included patient demographic characteristics like age and gender; baseline clinical variables like their admission diagnosis (septic shock, cardiogenic shock, traumatic shock, severe post-operative hypotension, and other) and baseline MAP; 24-hour APACHE II (Acute Physiology and Chronic Health Evaluation - version 2) score; 24-hour SOFA score; baseline serum creatinine, cystatin C, and urinary NGAL levels; and maximum day 0 (first 24 hours) and day one (next 24 hours) urinary NGAL levels. Also computed from the serum creatinine levels was the 24-hour, 48-hour, and maximum percentage increase in creatinine over baseline, as per KDIGO guidelines.24 Since each analysis compared 2 subject groups, Student’s t tests were used for normally-distributed and Mann-Whitney U tests for non-normally-distributed continuous variables, with normality determined by calculating the Pearsonian coefficient of skewness, and Skp values between -1.96 and 1.96 considered indicative of a normal distribution. Meanwhile, Pearson x2 analysis was used for all nominal and ordinal variables. Because of multiple comparisons, for all bivariate analyses, a Bonferroni-adjusted p value of p=0.001 was used as the threshold for statistical significance, calculated as p=0.05 divided by (3 inter-group comparisons x 16 variables of interest; see Tables 1-3) = 0.05/48 = 0.001.33
Comparing ICU survivors versus non-survivors (N=75).
Comparing hospital survivors versus non-survivors (N=75).
Comparing patients dying in the ICU versus afterwards in the hospital.
The primary goal of multivariate analysis was to identify predictors of ICU and in-hospital mortality, adjusted for all other variables. Because we only had 75 subjects, but 10 independent variables for potential inclusion in models, stepwise (hierarchical) binary logistic regression was performed, the first model entering (through forward selection) patient age, gender, and ICU admission diagnosis into the model; the second model adding baseline APACHE II and SOFA scores to the residual step 1 model; the third model adding baseline serum creatinine, cystatin C, the maximum percentage increase in serum creatinine, and urinary NGAL levels; the fourth model, baseline, mean and minimum MAP; the fifth model baseline and day 0 and day one maximum and mean uNGAL levels; and the sixth and final model only those variables identified as potentially significant predictors (p≤0.10) across all 5 earlier models. Note that, when variables like baseline, mean, and minimum MAP or the 5 uNGAL measurements were added to a model for testing, that step’s model then was recreated using only the best of these newly added variables. When 2 such variables were found to be roughly equal, each was carried through separately to the final model. For each step, any variable with p<0.20 was retained for the next step. For the final model, p<0.10 was selected as the threshold for final variable retention.
To assess the accuracy of uNGAL for ICU and in-hospital mortality, receiver operating curves (ROC) were created using the best urinary NGAL-related predictor of both outcomes as the test statistic, and ICU mortality, and in-hospital mortality (yes/no) as binary status variables. From these, areas under the curve (AUC) were calculated to determine the value of the test variable as a predictor of ICU and in-hospital mortality, and then the optimum cutoff values of the test variable identified to optimize accuracy, defined as the best balance of sensitivity and specificity.
All tests were 2-tailed and performed using the Statistical Package for Social Sciences (SPSS) version 23.
Results
Over the 13 months of recruitment, a total of 75 patients met eligibility criteria and were followed. Patients ranged in age from 18 to 89 years old (mean = 51.6) and were almost evenly split by gender (38 males, 37 females). The admission diagnosis for all 75 was, in itself, a major risk factor for AKI, with 34 (45.3%) admitted with septic shock; 20 (26.7%) with cardiogenic shock; 5 (6.7%) with traumatic shock; and 16 (21.3%) post-operative hypotension. The surgical procedures performed were neurological, cardiovascular, major abdominal, and gynecological, the number of cases ranging from 3 to 6 for each. Baseline MAP ranged from a low of 43 to a high of 69 (mean = 56.4). For the management of hypotension, 44 of 75 (58.7%) required one vasopressor, while 28 (37.3%) required more than one, and 46 (61.3%) were administered an inotrope. Baseline APACHE scores ranged from 10 to 47 (mean = 24.6), while SOFA scores ranged from 4 to 16 (mean = 9.8).
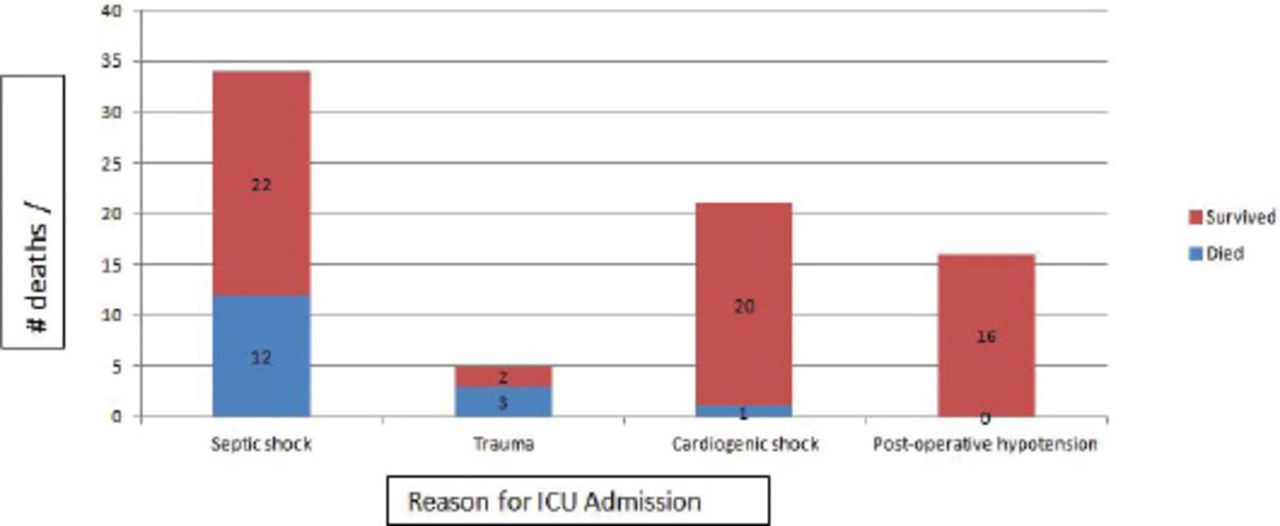
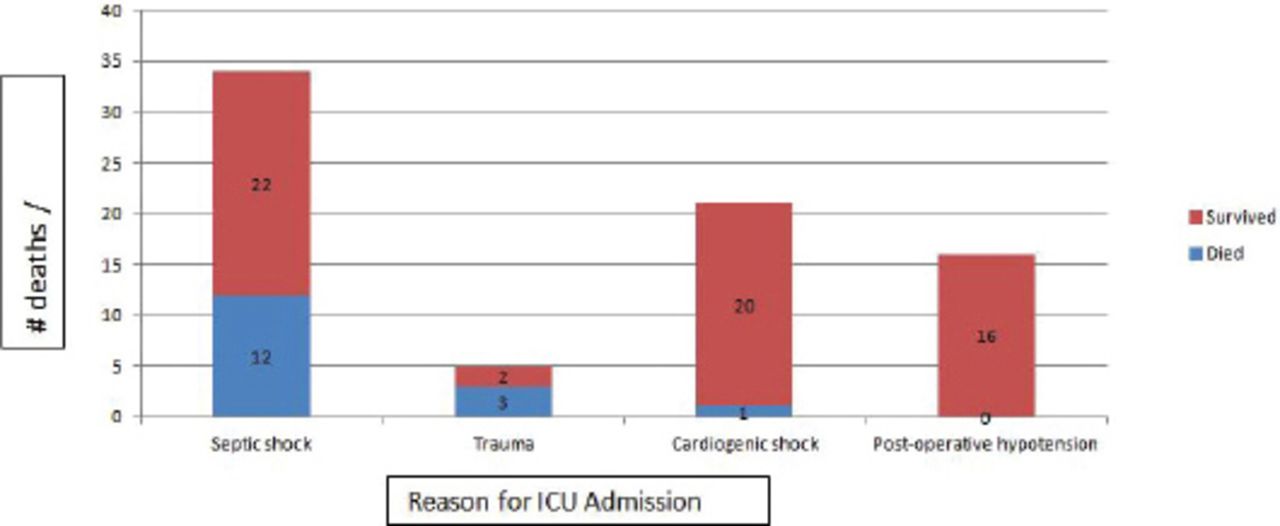
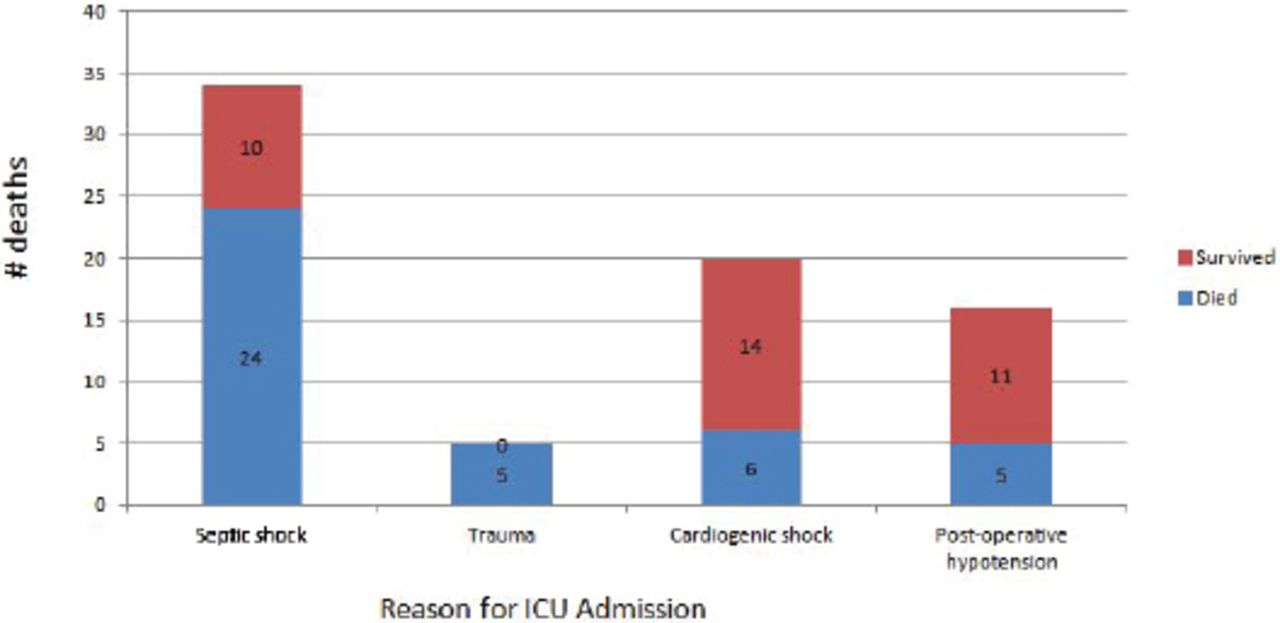
Table 1 summarizes outcomes across the sample, in terms of death and renal injury. Note that renal function was only assessed over the course of the hospital stay, so we present no data here on long-term outcome. In our subject sample, there was a very strong association between the level of injury, as indicated by the cystatin C level and the KDIGO GL criteria (x2 = 47.9, p<0.001). In total, 16 of the 75 patients (21.3%) died during their ICU stay and 40 (an additional 24) prior to discharge from hospital. Twelve of the 34 patients admitted for sepsis died in the ICU, versus 3 of 5 admitted for trauma, one of 20 admitted for cardiogenic shock, and zero of 16 post-operative hypotension patients (x2=15.92, p=0.001; Figure 1). Accounting for the 40 who died prior to hospital discharge (16 in the ICU and 24 afterwards) were 24 of the 34 patients admitted with sepsis, all 5 admitted for trauma, 6 of 20 admitted with cardiogenic shock, and 5 of 16 admitted for post-operative shock (x2 = 15.95, p=0.001; Figure 2).
Causes of death in the ICU.

Causes of in-hospital death.
Table 2 summarizes the bivariate comparison between ICU survivors (n=59) and non-survivors (n = 16). Note that there was no statistically significant inter-group difference in either mean age or gender distribution. However, even at the conservative Bonferroni-adjusted threshold of p≤0.001, the 2 groups were statistically different in nearly every clinical variable of interest, including their 24-hour APACHE II and SOFA scores; baseline, maximum, minimum and mean MAP; baseline serum creatinine; the maximum percentage increase of creatinine over baseline; maximum uNGAL levels over the first and second 24 hours in the ICU, and the first 48 hours combined; and the presence of either AKI or severe AKI. The only clinical variables that were not different between the 2 groups were the baseline serum cystatin C level and mean improvement (increase) in MAP over the first 72 hours.
Table 3 summarizes the bivariate comparison between hospital survivors (n=35) and non-survivors (n=40). Again, there was no significant difference in gender distribution; and, though there was almost a 9-year difference in age (46.7 versus 55.8 years), this difference failed to meet the a priori Bonferroni-adjusted threshold for significance. Also failing to meet the Bonferroni-adjusted threshold were the presence of AKI and development of severe AKI (both p=0.003). Neither improvement in MAP over the first 72 ICU hours nor baseline cystatin C level even approached statistical significance. All other clinical variables were different at a p≤0.001 level.
On multivariate analysis, the maximum level of uNGAL recorded on the first ICU day (p=0.035) and the maximum percentage increase of creatinine over baseline (p=0.032) were the only variables that remained in a binary logistic model predicting mortality in the ICU, while the APACHE II score was the only remaining predictor in the model predicting in-hospital death. The AUC of day one uNGAL was 0.85 (0.75, 0.95, p<0.001) for ICU death, indicating that it was a good indicator of future ICU mortality, with sensitivity of 93% and specificity of 58% at the uNGAL normalcy threshold of 150ng/mL; 87% and 64% at 200ng/mL; 80% and 81% at 500ng/mL; and 67% and 88% at an uNGAL threshold of 1000ng/mL. For in-hospital death, the AUC was 0.74 (0.63, 0.86, p<0.001), suggesting that day one uNGAL was only a fair predictor of future ICU mortality. Sensitivity and specificity were 68% and 65% at 150ng/mL; 61% and 71% at 200ng/mL; 50% and 88% at 500ng/mL; and 40% and 94% at a day one uNGAL level ≥1000 ng/mL. Areas under the curve for the maximum percentage increase of creatinine over baseline were 0.85 (0.74, 0.97, p<0.001) for ICU death and 0.70 (0.58, 0.82, p=0.003) for in-hospital death.
Since both ICU and in-hospital mortality were especially high in both patients with sepsis (12/34 and 24/34) and those admitted for trauma (3/5 and 5/5), we wanted to perform further analysis to assess the AUC and optimum threshold for sensitivity and specificity for both these groups. However, given that there were only 5 trauma patients, this latter analysis was not carried out. Among the 34 presenting to the ICU with sepsis, the AUC for ICU death was 0.90 (95% CI = 0.78, 1.00, p<0.001); and the optimum accuracy (combining a sensitivity of 91.7% and specificity of 81.2%) was achieved at the uNGAL threshold of 1000ng/mL. Meanwhile, for in-hospital mortality, the AUC was 0.85 (0.64, 1.00), and the optimum accuracy (sensitivity 90.5%, specificity 85.7%) was achieved at the uNGAL threshold of 300ng/ml. At uNGAL thresholds of 500 ng/ml and 1000ng/ml, sensitivity and specificity were 85.7% and 85.7% and 61.9% and 85.7%.
Discussion
For reasons that are not entirely understood, AKI appears to be increasing in incidence, especially in critically ill patients.8,34 Most common in patients with sepsis,8,35,36 AKI also appears to be an independent predictor of mortality.32 In our sample, which included patients with septic, traumatic, and cardiogenic shock, as well as with post-operative shock, the mortality rate prior to hospital discharge among those with documented AKI was an alarming 81%, with 50% of those with AKI dying during their initial ICU stay.
Urine levels of NGAL have been examined by numerous investigators, including ourselves, as an indicator of renal injury, both in animal models,37,38 and in humans,7,9,23,25,28,39,40 A much smaller number of studies have examined the role of NGAL as a predictor of mortality. Haase et al7 performed a meta-analysis of 19 studies performed between 2005 and 2009, inclusive, to assess the role of NGAL predicting early AKI; but only 7 of these studies provided usable data on mortality. Using thresholds ranging from 80 ng/mL to 570 ng/mL, sensitivity rates for mortality spanned from 43-100%, while specificity ranged from 38.7-100%. The overall AUC across the 7 studies was 0.71, suggesting that NGAL was, at best, a fair predictor of mortality. More recently, Hong et al41 calculated an AUC of 0.80 in 470 patients with sepsis followed for up to 28 days. Meanwhile, Lipinski et al42 discovered that admission and day one urine levels of NGAL were highly predictive of mortality from pancreatitis, with AUC values of 0.98 and 0.92. However, Yang et al43 found that, though both urine and plasma levels of NGAL obtained during the first 12 hours post admission predicted early AKI and mortality in patients with massive burns, they did not predict long-term mortality. Meanwhile, Wang et al44 discovered plasma NGAL to be an independent predictor of mortality in 143 patients with sepsis during their ICU stay; however, the AUC was only 0.63, suggesting that it was, at best, a weak predictor. Similarly, Nisula et al40 found urinary NGAL to be a weak prognosticator for 90-day mortality in 1052 critically-ill patients in Finland, with an AUC of just 0.63; this contrasted against a much convincing AUC of 0.84 predicting renal replacement therapy. Moledina et al45 identified no association between plasma NGAL levels and 3-year mortality in cardiac surgery patients. The literature trend thereby appears to be that NGAL is a better predictor of short-term than long-term mortality.
Our data are consistent with all this in that, in our study sample, uNGAL was a good predictor of mortality while patients remained in the ICU, with an AUC of 0.85; however, it was only a fair predictor of longer term, post-ICU but pre-hospital discharge mortality (AUC = 0.74). On multivariate analysis; in fact, the maximum level of NGAL measured in urine over the first 24 hours in the ICU was the best predictor of ICU mortality, the only other significant predictor being the global systemic illness severity scale, APACHE II. Urinary NGAL dropped out of the model predicting mortality throughout the hospital stay; leaving the APACHE II score alone. Further evidence that uNGAL is a better marker of early than later mortality is our finding that, when we compared the 16 patients who died in the ICU and the 24 who died later in hospital, the 3 measures of uNGAL, maximum level on ICU day one, maximum level on ICU day 2, and maximum level over those first 2 days combined, were among the abbreviated list of just 5 variables in the final regression model that statistically distinguished these 2 groups at the p≤0.001 level, the remaining 2 variables being the 24-hour APACHE II and SOFA scores.
At some level, given that NGAL is believed to be a marker of acute inflammation, released by neutrophils and endothelial cells as part of the acute inflammatory response.14,46 Among its known functions, it is known to bind to formyl peptides released by bacteria,14 so that it might be especially expected in patients with bacterial sepsis, as was the admitting diagnosis in 34 of the 75 patients in our patient cohort. This conjecture is further supported by our own data that showed that day one maximum uNGAL levels were appreciably higher in our patients with the more systemic inflammation generally associated with major trauma or sepsis (1032.5 and 898.8) than in those with the more localized inflammation usually attributed to cardiogenic or post-operative shock (358.2 and 99.1). It also was an especially accurate predictor of ICU mortality among our septic patients, with AUC rising from 0.85 among all patients to 0.90 just among those with sepsis.
Another interesting finding of our study was that, though both the APACHE II and the SOFA global illness severity scores were significantly different in ICU survivors versus non-survivors, and in hospital survivors versus non-survivors, on multivariate analysis, the APACHE II appeared to be superior at predicting both ICU and in-hospital mortality. Most prior studies assessing these 2 items in various critically-ill patients had found them to be relatively comparable;47-49 however, this was generally on bivariate rather than multivariate analysis, so that a true comparison, adjusted for other potential confounders, was never made. Speculating on the reason behind this apparent superiority of the APACHE in our subject sample is beyond the scope of this paper. However, it might relate to the measurement and rating of 12 components of systemic illness with the APACHE II scale versus just the 6 with the SOFA.50,51
Study limitations
Among them are the relatively small patient population, which prohibited much sub-group analysis; for example, although we had enough patients with sepsis (n=34) to calculate the AUC of uNGAL for mortality in patients with sepsis, we had only 5 patients with major trauma, the other patient sub-population with significant ICU mortality; among the 36 with either cardiogenic or post-operative shock, only one patient died in the ICU. We do note, however, that maximum levels of uNGAL were much higher among patients with sepsis or post-trauma than in either of the other 2 groups. We also were somewhat inconsistent in the number of daily measurements of NGAL that we did from patient to patient, though it generally was measured 3 times, and all patients were measured at least twice on ICU days one and 2. Some might also call into question our decision to assess urine alone rather than both urine and plasma levels of NGAL; we made this decision because the former has tended to outperform the latter as a predictor of AKI. Finally, there were numerous other variables that we might have assessed as predictors of mortality, like baseline electrolytes, arterial pH, respiratory status, and neurological status, among others. On the other hand, many of these variables are encompassed by the APACHE score, the SOFA score, or both.
These weaknesses considered, our study has definite strengths, such as, we did measure NGAL multiple times each day. Other strengths, we feel our study has, are our serial measurement of mean arterial pressure and that we assessed different levels of renal injury, which was either not carried out or not reported for several earlier studies. Ours is also the only such study reporting data collected in Saudi Arabia.
Others, including our own study group, have demonstrated that urine levels of NGAL are of value as predictors and indicators of renal outcomes, especially AKI. In this study, we found not only that uNGAL predicts death, but that it and the maximum percentage increase in serum creatinine over baseline were the best predictors of ICU mortality among all the variables we studied, including global systemic disease severity measures like the APACHE II and SOFA scales assessing global systemic illness. It has the advantage over the maximum percentage creatinine increase (derived from the KDIGO guidelines criteria) of being available on day one of hospitalization, instead of having to wait a minimum of 48 hours to observe the 48-hour percentage increase in creatinine. In addition, given that earlier detection of risk tends to portend more favorable outcomes, this might be a clinically meaningful advantage. It also appears to be even more sensitive and specific in patients admitted for septic shock. We, therefore, add our results to the accumulating mountain of data supporting the use of NGAL as a marker of critical illness outcomes.
In conclusion, in our study, the maximum urine level of NGAL measured over the first 24 hours of an ICU stay was a highly-accurate predictor of mortality in the ICU, especially among patients with septic shock; but it was less of a predictor of mortality once patients were discharged from the ICU.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 13, 2016.
- Accepted March 23, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}