


Abstract
Objectives: To evaluate the histopathological changes in the liver after oral antiviral therapy in patients with chronic hepatitis B.
Methods: A total of 79 HBeAg-negative and positive patients who had been on lamivudine, entecavir, or tenofovir disoproxil for at least 3 years prior to inclusion were enrolled between March 2015 and 2016, retrospectively. There were 23 patients on lamivudine, 21 patients on entecavir, and 35 on tenofovir. All patients underwent a follow-up liver biopsy. Biochemical, serological, virological and histopathological data were recorded in all patients and were compared after at least 3 years of treatment with oral antiviral agents.
Results: Histological activity index scores were reduced in patients who received lamivudine (p=0.011), entecavir (p=0.002), and tenofovir (p=0.001). Also, in contrast with a significant improvement in fibrosis scores in lamivudine (p=0.033) and tenofovir (p=0.001) groups no improvements were found in patients who received entecavir (p=0.090).
Conclusion: Long term treatment with oral antiviral agents was associated with biochemical, virological, serological, and histopathological improvements. Long-term use of anti-viral agents as well as continuous suppression of HBV DNA are prerequisites for histopathological improvement.
According to current estimates, there are approximately 350 to 400 million individuals with chronic hepatitis B virus (HBV) infection worldwide. Annually, almost 1 million deaths occur due to HBV-related diseases.1 The reported prevalence rate of HBV infection varies between 0.1% and 20%, and nearly 3 million individuals are estimated to have been infected with HBV in Turkey.2 Chronic hepatitis B (CHB) infection may have long-term consequences, with associated hepatic disorders.3 Of patients followed up with a diagnosis of chronic HBV infection, 15-45% developed cirrhosis, decompensated hepatic failure, or hepatocellular carcinoma (HCC).4 The results of randomized clinical studies have established the role of suppression of viral replication with antiviral agents in improving liver histology, in addition to preventing the development of fibrosis and complications in patients with CHB.5 The major goal of antiviral treatment is to achieve long-lasting suppression of HBV DNA to low or undetectable levels to prevent progression to hepatic failure or HCC, as well as reducing early deaths or the need for a liver transplantation.6,7
The present study investigated the responses of CHB patients to long-term oral antiviral therapy in terms of biochemical alanine aminotransferase (ALT), aspartate transaminase (AST), virological (HBV DNA levels), serological (HBeAg, antiHBe, HBsAg, and antiHBs), and histopathological (histological activity and fibrosis scores based on the modified Knodell system).
Biochemical, virological and serological parameters, in addition to oral antiviral agents administered, were recorded at the time of diagnosis and at least 3 years after treatment. The results of post-treatment repeated liver biopsies were also recorded and assessed.
Methods
This was a retrospective study of 79 patients with a diagnosis of CHB who were treated and followed up between March 2015 and March 2016 at outpatient units of the Department of Infectious Diseases and Clinical Microbiology and Gastroenterology. Data were obtained from an electronic database. Patients between 18 and 70 years receiving oral antiviral agents (lamivudine, entecavir, or tenofovir disproxil fumarate) for a minimum duration of 3 years due to CHB were included. Children, pregnant women, and patients with decompensated cirrhosis were excluded. The study was organized according to the principles of Helsinki Declaration.
Baseline biochemical parameters (AST, 0-35 U/L; ALT, 0-35 U/L), serological markers (HBeAg, antiHBe, HBsAg, and antiHBS), viral loads (HBV DNA, IU/mL), complete blood counts, prior liver biopsies, ongoing treatments, and treatment durations were recorded as pre-treatment values. To detect serological markers, the enzyme-linked immunosorbent assay (ELISA) tests (Abbott Diagnostics, Architect System, USA) were conducted in accordance with the manufacturer’s recommendations. For the detection of the hepatitis B viral load, a real-time PCR system (COBAS AmpliPrep, COBAS TaqMan HBV real-time PCR) was used in accordance with the manufacturer’s instructions. The same set of tests were repeated post-treatment, and the results were recorded. A repeat liver biopsy was performed. These results were used as post-treatment parameters and compared with the baseline findings. The initial and final liver biopsies were simultaneously assessed by the same pathologist in the same session. The study protocol was approved by the university’s ethics committee (approval no. 2015/90). Informed consent was obtained from each patient before inclusion in the study.
Statistical analysis
The normal distribution fitness of the numerical data was tested by the Shapiro-Wilk test. An ANOVA test was conducted for comparison of the variables that fit a normal distribution in the 3 treatment groups (lamividune, entecavir, and tenofovir groups). Wilcoxon’s test was performed to compare non-normally distributed variables at 2 different time points in the groups. The Kruskal-Wallis test and Dunn’s multiple comparison test were used for comparisons of ANOVA normal non-parametric variables for comparisons of variables with a normal distribution in the 3 independent groups. Relationships between categorical variables were tested by the Chi square test and McNeamar test. The Statistical Package for the Social Sciences (IBM SPSS Statistics, NY, USA), version 22.0 was used in the analyses. A value of p<0.05 was considered significant. Median values were used in the evaluation of the obtained data. The results of the liver biopsies were compared both pre- and post-treatment by calculating the median and mean value ± standard deviation (SD).
Results
In total, 79 patients with a diagnosis of CHB who were taking oral antiviral agents for a minimum duration of 3 years and who were followed up at our unit were included. There were 51 males (64.4%) and 28 (35.4%) females. The duration of oral antiviral therapy was 3 years in 10 patients, 4 years in 15 patients, and 5 years in 54 patients. The mean age was 40.92 ± 10.90 years. The treatments included lamivudine in 23 (29.1%) cases, entecavir in 21 (26.6%) cases, and tenofovir in 54 (44.3%) cases. Prior to treatment, all patients were HBsAg(+) and antiHBs(-). Thirty-five patients (44.3%) were HBeAg(+), 44 patients (55.7%) were HBeAg(-), 42 patients (53.2%) were antiHBe(+), and 37 patients (46.8%) were antiHBe(-). Two patients were both HBeAg and antiHBe(-). The median pre-treatment HBV DNA was 7.9×106 (8.9×104 - 11×107), the median ALT was 61 (36-96) IU/ml), the median histological activity index (HAI) was 5 (4-6), and the median fibrosis score was 3 (2-4).
A comparison of pre- and post-treatment HBeAg positivity in the 3 groups showed no significant changes based on McNemar’s test (lamividune [p=0.250], entecavir [p=0.125], and tenofovir [p=0.453] groups). This is most probably due to the small sample sizes leading to low test power and it is a limitation of the study. Patients who were HBeAg(-) in the lamivudine and entecavir groups prior to treatment were also HBeAg(-) in their final follow-up assessments. Two patients in the tenofovir group were HBeAg(+).
Pre-treatment, the study groups were comparable in terms of HAI scores (p=0.807). Upon completion of treatment, there were no significant differences in the HAI scores of the 3 groups (p=0.228). Prior to treatment, the median HAI in 23 patients in the lamivudine group was 5 (4-6), and the median post-treatment HAI was 3 (2-5). In the lamivudine group, the mean HAI pre- and post-treatment score has a statistically significant difference (p=0.011) (Table 1). Among the 21 entecavir patients, the median HAI before treatment was 4 (3.5-6.5) and after 2 (2-3). There was a significant difference between the pre- and post- treatment HAI in the entecavir group (p=0.002) (Table 1). Among the 35 patients in the tenofovir group, the pre-treatment median HAI score was 4 (4-7) and post- was 2 (2-4). The difference between the pre- and post- treatment HAI scores in these patients was statistically significant (p=0.001) (Table 1).
Comparison of pre-treatment and post-treatment HAI in lamivudine, entecavir and tenofovir groups.
The 3 treatment groups were statistically comparable with regard to pre-treatment fibrosis scores (p=0.215), whereas post-treatment fibrosis scores showed significant differences (p=0.009). There was a significant difference in fibrosis scores post-treatment between the lamivudine and tenofovir groups (p=0.005); lamivudine and entecavir groups (p=0.010) but no significant difference in these scores between the tenofovir and entecavir groups (p=0.957).
Among the 23 patients in the lamivudine group, the median fibrosis score before treatment was 3 (2-4) and after was 3 (2-3). The pre-treatment and post-treatment fibrosis scores in this group were significantly different (p=0.033) (Table 2). In 21 patients who received entecavir, the pre-treatment fibrosis scores were 3 (2-3) and post- were 2 (2-3). The difference in the pre-treatment and post-treatment fibrosis scores in the entecavir group was not significant (p=0.09) (Table 2). The median fibrosis scores before treatment among the 35 patients in the tenofovir group were 3 (2-3) and after was 2 (2-2). There was a significant difference between the pre- and post-treatment fibrosis scores among the tenofovir patients (p=0.001) (Table 2).
Comparison of pre-treatment and post-treatment fibrosis scores among lamivudine, entecavir and tenofovir patients.
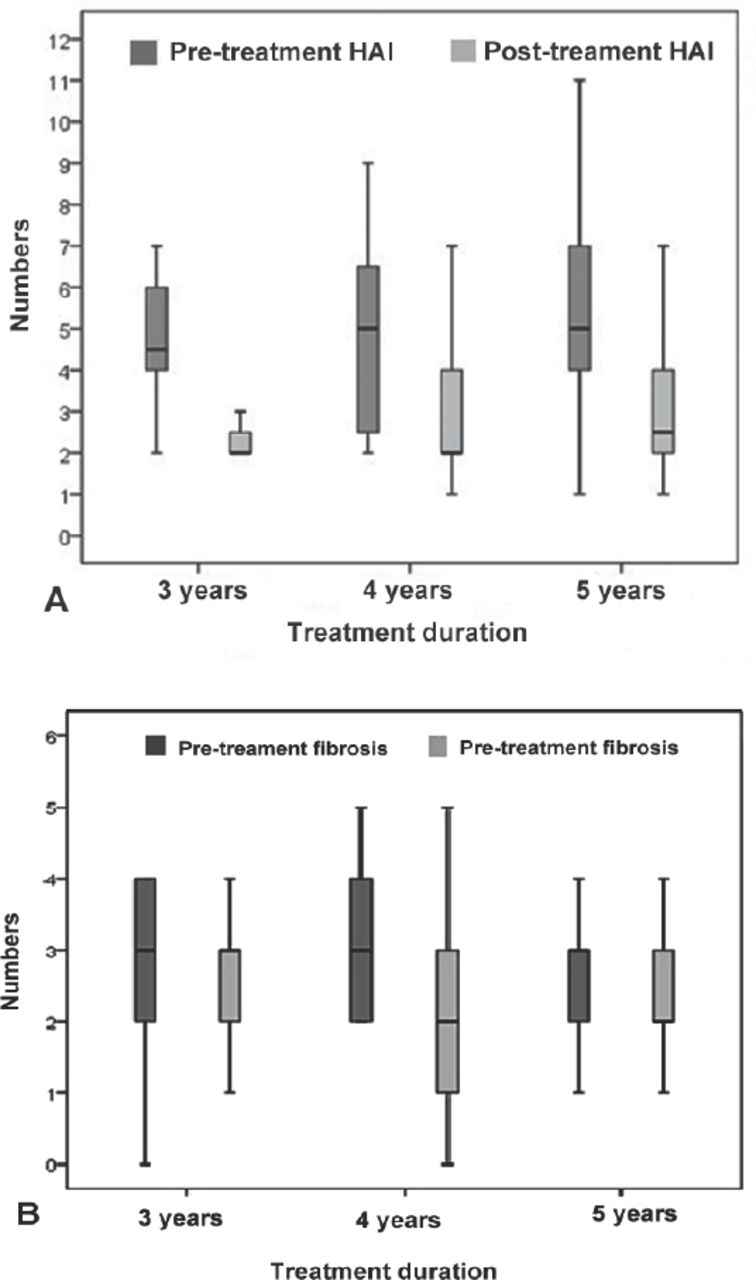
The patients in the 3 groups were stratified according to the duration of treatment (namely, treatment for 3, 4, or 5 years) (Table 3 and Figures 1A & 1B).
A correlation analysis between the duration of treatment and the values of HAI and fibrosis (pre, post, and improvement in scores).
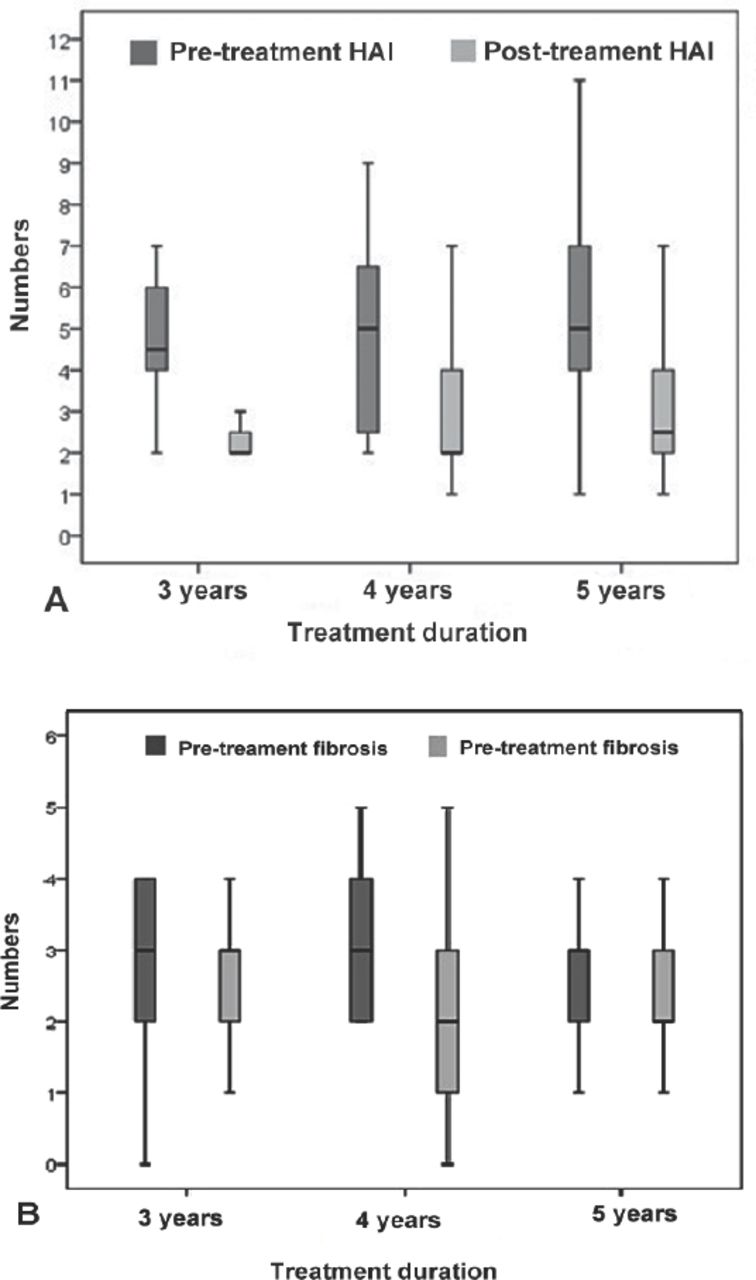
Median analysis: A) pre-treatment and post-treatment histological activity index according to treatment duration B) pre-treatment and post-treatment fibrosis scores according to treatment duration.
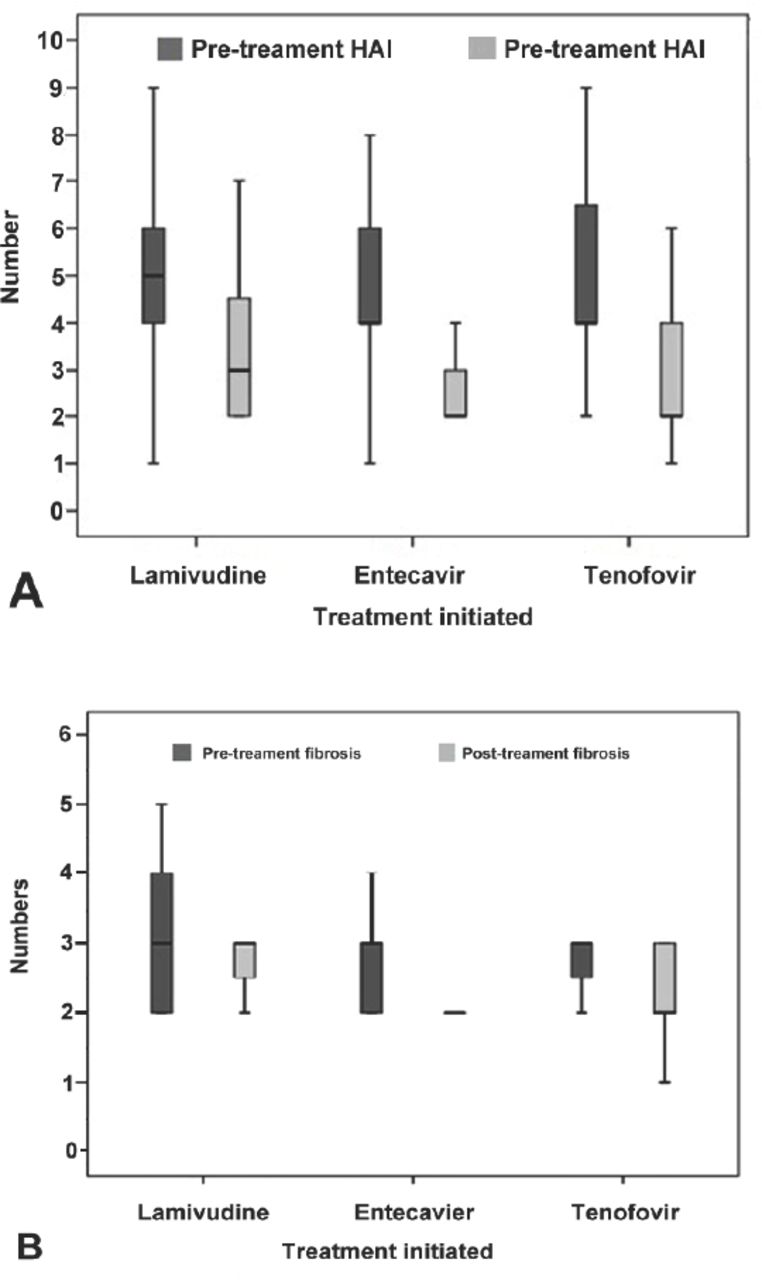
Figures 2A & 2B show the median pre-treatment and post-treatment HAI scores and the fibrosis values according to the treatment administered. Among the study groups, a liver biopsy was performed 3, 4, and 5 years after treatment commencement in 10, 15, and 54 of 79 patients, respectively. The fibrosis scores of 5/10 (50%), 10/15 (66.6%), and 30/54 (55.5%) patients improved by ≥1 point, respectively. Among these patients with a ≥1 point increase in the fibrosis score were 2/10 (20%), 0/15 (0%), and 5/54 (9.2%), respectively. The respective figures for patients with no change in their fibrosis scores were 3/10 (30%), 5/15 (33.3%), and 19/54 (35.1%). Among the patients who underwent a biopsy after 3, 4, and 5 years, 6/10 (60%), 9/15 (60%), and 31/54 (57.4%) patients, respectively, showed a ≥2 point improvement in HAI scores. The number of patients with no change or a decrease of <2 points in HAI scores was 4/10 (40%), 4/15 (26.6%), and 17/54 (31.4%), respectively, whereas the corresponding figures for patients with increasing (>2 points) HAI scores were 0/10 (0%), 2/15 (13.3%), and 6/54 (11.1%).

Median analysis: A) pre-treatment and post-treatment histological activity index (HAI) according to the treatment initiated B) pre-treatment and post-treatment fibrosis scores according to the treatment initiated.
Figures 3A & 3B show the changes in HAI and fibrosis scores according to the duration of treatment in patients receiving oral antiviral agents.

Graphic representation of the distribution of histological activity index (HAI) A) and fibrosis scores B) based on liver biopsy at baseline and after 3, 4, and 5 years of treatment with lamividune, entecavir or tenofovir
Discussion
Elevated HBV DNA is a known risk factor for the progression of liver disease.8,9 The objective of CHB treatment is to achieve long-lasting suppression of viral replication to reduce the risk of progression and to prevent complications, such as liver failure, death, cirrhosis, or HCC.1 Previous research demonstrated that long-term lamivudine treatment reduced hepatic decompensation and the incidence of HCC.10 Two studies in Taiwan reported similar findings.11,12 Although the use of pegylated interferon in CHB is limited to 1 year, oral antiviral agents can be administered for longer term treatment. Based on literature data, the general recommendation with regard to treatment duration is to continue oral antiviral therapy for at least 6 months after HBeAg seroconversion.1,13,14 In HBeAg(-) CHB patients, there is no clear evidence at present for the optimun duration of oral antiviral treatment. However, in HBeAg(+) and (-) patients, the aim is long-term viral suppression.13,15
This retrospective study compared biochemical, virological, serological, and histopathological results in CHB patients receiving long-term treatment with lamividune, entecavir, or tenofovir. The results showed that continued suppression of HBV DNA in patients receiving long-term oral antiviral treatment may lead to ALT normalization and a histopathological improvement. Hepatitis B virus DNA of <20 IU/ml was detected in 60%, 60%, and 83.3% of patients who received lamivudine, entecavir, and tenofovir treatment for 3, 4 and 5 years, respectively. These results demonstrate that long-term oral antiviral treatment can achieve high rates of HBV DNA suppression. The proportion of patients with ALT normalization in the lamivudine, entecavir, and tenofovir treatment groups was 60%, 73.3%, and 72.2%, respectively.
A virological response (HBV DNA <20 IU/ml) was found in 21 of 35 (60%) HBeAg(+) patients and 39 of 44 (88.6%) HBeAg(-) patients. Overall, 60 of 79 (75.9%) patients had a virological response. Virological response rates 3, 4, and 5 years post-treatment were 60%, 60%, 83.3%, respectively, in the entire study group; 66.6%, 66.6%, and 81.8%, respectively, in the lamivudine group; 100%, 60%, and 93.3%, respectively, in the entecavir group; and 33%, 50%, and 78.5%, respectively, in the tenofovir group. The differences observed may be due to the small sample size. A previous study involving 204 patients reported a virological response rate of 87.5% after 5 years of entecavir treatment in compensated cirrhotic patients, whereas the corresponding figure in decompensated cirrhotic patients was 92.5% (p=0.077).16 In another study of HBeAg(+) CHB patients, 2 years of entecavir use resulted in a virological response rate of 80%, whereas the virological response rate for 2 years of lamivudine use was 39% (p<0.001).17 In another study, among HBeAg(-) CHB patients, the virological response rate after 2 years of entecavir or lamivudine treatment was 94% and 77%, respectively (p<0.001).18 Furthermore, 5 years of entecavir treatment led to a virological response rate of 97% in HBeAg(+) patients and 99% in HBeAg(-) patients.19 A phase III study in France reported a response rate of 94% after 5 years of entecavir treatment.20 In the same study, the virological response rate in 238 HBeAg(+) patients was 97%, whereas it was 99% in 347 HBeAg(-) patients.
In the present study, ALT normalization was found in 21 of 35 (60%) HBeAg(+) and 35 of 44 (79.5%) HBeAg(-) patients. Alanine transaminase normalization after 3, 4, or 5 years of treatment occurred in 60%, 73.3%, and 72.2% of the patients, respectively. The observed rates of ALT normalization in the lamivudine, entecavir, and tenofovir groups were 82.6%, 57.1%, and 71.4%, respectively, with an overall rate of 70.8%. In a similar phase III trial of patients who received oral antiviral treatment for 5 years, ALT normalization rates in 125 patients who received lamivudine were 69%, and they were 80% in 146 patients who received entecavir.20 In the same study, 238 and 347 of 585 patients who received tenofovir were HBeAg(+) and HBeAg(-), respectively. Of these, 73% of HBeAg(+) patients and 85% of HBeAg(-) patiets showed a biochemical response.20 In the current study, the highest biochemical response rates were found in the lamivudine groups, whereas patients in the tenofovir group exhibited the lowest biochemical response rates. This observation may be related to the small number of participants included. In a previous study, 3 years of entecavir treatment in 69 patients resulted in a response rate of 86%.5 In another study, 2 years of lamivudine (n=145) or entecavir treatment (n=193) resulted in biochemical response rates of 82% and 96%, respectively (p<0.05).16 In a Japanese study of patients who received entecavir, 52 of 59 (88%) patients who were treated for 96 weeks and 128 of 142 (90.1%) patients who were treated for 120 to 148 weeks had ALT normalization.8 In a study conducted in France, tenofovir treatment was associated with responses in 124 of 169 (73%) HBeAg(+) patients and in 236 of 277 (85%) HBeAg(-) patients.19 In another double-blind phase III study involving HBeAg(-) CHB patients, 222 of 313 (71%) patients who were treated with lamivudine and 253 of 325 (78%) patients who were treated with entecavir had ALT normalization.21 HBeAg loss was observed in 3 of 3 (100%) HBeAg(+) patients in the lamivudine group, 4 of 13 (30.7%) HBeAg(+) patients in the tenofovir group, and 5 of 19 (26.3%) HBeAg(+) patients in the tenofovir group. The respective HBeAg seroconversion rates were 100%, 23%, and 10.5%. It is probably due to the small sample sizes and a limitation of this study. Some previous reports found higher rates of HBeAg seroconversion with long-term oral antiviral treatment. Among 164 HBeAg(+) patients who received tenofovir for 5 years, 81 patients (49%) had HBeAg loss, and 66 (40%) had HBeAg seroconversion.19 In another study, 3 years of entecavir use was associated with HBeAg loss in 22 of 40 (55%) patients and with HBeAg seroconversion in 13 of 40 (33%) patients.5 In another study, 10 of 49 (20%) patients achieved seroconversion after 2 years of entecavir treatment, whereas treatment duration exceeding 2 y resulted in seroconversion in 32 of 121 (26.4%) cases.8 Furthermore, in a study of 58 patients, the authors reported seroconversion rates of 22% (n=13), 29% (n=17), and 40% (n=23) at the end of 1, 2, and 3 years, respectively.22
In the present study, in the entire study group (namely, patients treated with any of the oral agents lamivudine, entecavir, or tenofovir), the HAI scores of 60%, 60%, and 57.4% of the population who had a biopsy after 3, 4, and 5 years post-treatment, respectively, improved by ≥2 points. An increase in HAI scores occurred in 0%, 13.3%, and 11.1%, respectively. Among all patients who had a biopsy after 3, 4, or 5 years post-treatment, the fibrosis scores of 50%, 66.6%, and 55.5%, respectively, showed an improvement of ≥1 point (Table 3). An increase in fibrosis scores was found in 20%, 0%, and 9.2%, respectively. When the patients were classified into 3 subgroups based on the treatment they received (namely, lamivudine, entecavir, or tenofovir), all 3 groups showed a statistically significant improvement in HAI scores (p=0.011, p=0.001 and p=0.002). On the other hand, statistically significant improvements in fibrosis scores were found in the lamivudine- and tenofovir-treated patients (p=0.033 and p=0.001, respectively), whereas there were no significant changes in the fibrosis scores among the entecavir recipients (p=0.090). Considering the median level, there was a decrease in the levels of fibrosis in the patients receiving entecavir. This finding may explain the higher rate of HBeAg positivity (13/21) in this group. Previous research reported that long-term oral antiviral therapy provided significant improvements in both fibrosis and HAI scores. A study of the effect of treatment with different oral antiviral agents on liver histopathology reported an improvement in HAI scores in 56% of 63 patients who received lamivudine for 3 years, 96% of 57 patients who received entecavir for 6 years, and 89% of 124 HBeAg(+) patients and 87% of 224 HBeAg(-) patients who received tenofovir for 5 years.20 In cirrhotic patients who were treated with tenofovir for 5 years, 87% (304/348) exhibited an improvement in HAI scores.19 In the same study, 51% (176/348) of patients had improved fibrosis scores (p<0.001). The study reported that patients who had a fibrosis score ≥4 at study entry comprised 38% of the study population and that this figure declined to 12% at the end of 5 years (p<0.001). Of the overall population, 28% had a fibrosis score ≥5 at study entry, and this figure declined to 8% at the end of 5 years (p<0.001). In a Chinese study of 38 cirrhotic patients who received entecavir for 5 years, 89.5% of patients showed an improvement in both HAI and fibrosis scores (p<0.001).16 In a phase III study, the authors reported an improvement in HAI and fibrosis scores in 73% and 32% of patients, respectively, after entecavir use.5 In the same study, among a subgroup of 57 patients who were treated with entecavir for at least 3 years, long-term treatment was associated with an improvement in HAI scores in 55 (96%) patients, whereas 50 of 57 (88%) patients had improved fibrosis scores. In another study of 19 patients treated with entecavir for 3 years, 100% and 63% of patients exhibited an improvement in HAI and fibrosis scores, respectively.23
The small number of patients and heterogeneous nature of the study group were limitations of the present study. Nevertheless, long-term use of oral antiviral agents was associated with biochemical, virological, and histopathological improvements. Patients need to be convinced of long-term treatment with oral antiviral agents. Given the positive impact of histopathological improvements in a patient’s prognosis, long-term use of oral antiviral agents to achieve continued suppression of HBV DNA seems warranted. However, multicenter studies are needed to confirm.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 29, 2018.
- Accepted August 22, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.