


Abstract
Objectives: To explore the atherosclerotic changes of the left anterior descending coronary artery (LADCA) in patients with early onset of rheumatoid arthritis (RA).
Methods: Transthoracic echocardiographic scans were performed on 15 early RA patients and 20 control subjects, free of rheumatological diseases, diabetes mellitus (DM), and cardiovascular disease (CVD). Out of 15 RA patients, 10 were matched for age and gender with control. Left anterior descending coronary artery wall thickness was compared between RA subjects and their matched control. Among early RA patients, correlation was assessed between LADCA wall thickness and the demographic features, RA activity features, and cardiovascular risk factors.
Results: Left anterior descending coronary artery wall thickness was significantly increased (p=0.001) in early RA compared to controls, as it was reported to be 0.61±0.04 mm (CI: 0.52-0.7); and 0.48±0.08 mm (CI: 0.44-0.51) respectively. Within early RA, LADCA wall thickness was related to the disease activity score (p=0.025, ß-coefficient 0.066, CI: 0.01-0.122) as well as to the patient global assessment of disease activity (PGADA) at RA onset (p=0.006, ß-coefficient 0.003, CI: 0.001-0.005), in a positive linear relationship. Left anterior descending coronary artery wall thickness was found to be thicker among RA patients with rheumatoid factor (RF) positive (p=0.015, CI: 0.53-0.66).
Conclusion: Early RA patients have increased coronary arteries atherosclerotic burden compared to healthy subjects matched for age, and gender. Rheumatoid factor positivity, high disease activity score and PGADA were found to be associated with coronary artery wall thickness.
Rheumatoid arthritis (RA) is a chronic inflammatory and destructive joint disease affecting around 1-3% of the general population and is associated with increased mortality and morbidity with cardiovascular disease (CVD) as an underlying leading cause.1 The role of inflammation has been well established in the formation, progression, and complication of atherosclerosis in RA.2 Ultrasound (US) testing has provided valuable insights into early atherogenesis by measuring carotid intima-media thickness,3,4 and endothelial dysfunction (ED), and these factors are the indicator of atherosclerosis at the earliest stage.5,6 It has been demonstrated that early and established RA patients have increased risk of sub-clinical vascular disease compared to their matched controls due to the high prevalence of carotid disease5,7 and ED.6,8 Atherosclerosis is considered to be a diffuse process, and it can be evaluated in other vessels such as the left anterior descending coronary artery (LADCA).9 Therefore, we investigated, whether the presence of generalized atherosclerotic changes are evident at early RA by studying LADCA wall thickness in RA patients presenting within 12 months of symptom onset.
Left anterior descending coronary artery and its proximal branches have been identified with 2-dimensional transthoracic echocardiography (TDTE) using short axis views.10-13 Left anterior descending coronary artery wall thickness was found to be significantly increased in coronary artery disease patients compared to healthy subjects. Furthermore, the high-resolution TDTE was found to be sensitive enough to detect these differences.14
Methods
Study participants
All 15 RA study participants including 7 female (47%), and 8 male (53%) met the ACR 1987 revised criteria for the classification of RA.15 All the patients had RA symptoms for less than 12 months. None of the patients were on non-steroidal anti-inflammatory drugs (NSAIDs). Twelve out of the 15 RA patients were on methotrexate only, 2 were on methotrexate and sulfasalazine, and one was on a combination of methotrexate, sulfasalazine, and hydroxychloroquine. None of the patients were on biological medications. Twenty healthy subjects were recruited from the community. The controls matched with 10 early RA patients (out of total 15) for age, gender, and cardiovascular risk factors. All the participants were free of CVD/cerebrovascular disease (CBD), and DM.
Study procedure
The study was approved by the Research Ethics Committee of the Ministry of Health and Prevention of United Arab Emirates. All subjects provided written informed consent. Participants histories related to cardiovascular risk factors, smoking, CVD/CBD, DM, hypertension, dyslipidemia, family history of vascular events in first degree relatives, and body mass index were recorded.
Rheumatoid arthritis disease activity measurements
The participants were examined for the presence of RA nodules, RF positivity and level, anti CCP positivity and level, Disease Activity Score based on 4 variable using erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), health assessment questionnaire score, PGADA (DAS 28 with 4 variable), joints pain, and number of tenders and swollen joints based on 28 joints count.
Lipid profile measurements
Laboratory parameters including low-density lipoprotein, high-density lipoprotein, triglycerides, and cholesterol level were measured for all the participants.
Left anterior descending coronary artery wall thickness measurements
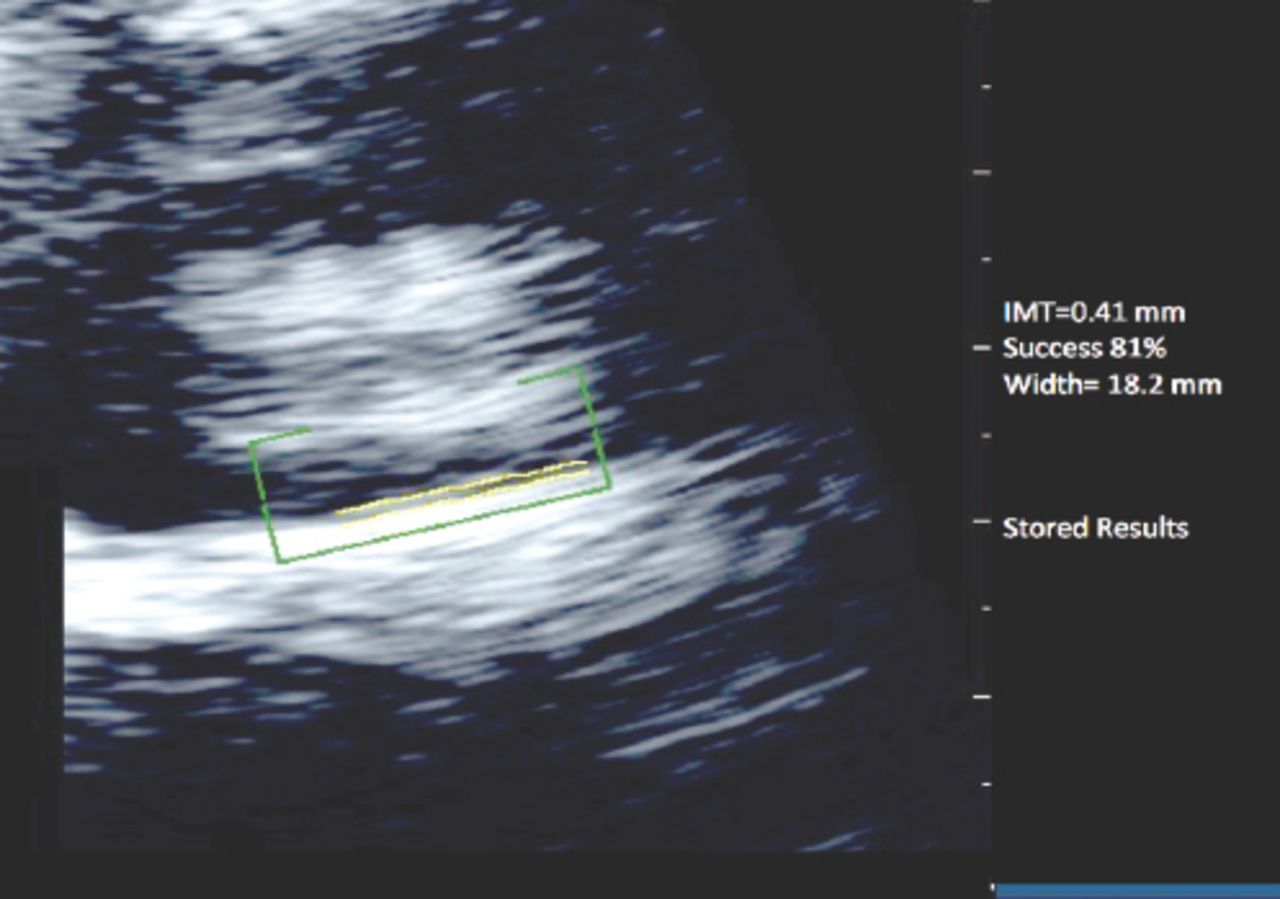
Left anterior descending coronary artery wall thickness was measured soon after the confirmed diagnosis of RA with no more than 12 months of symptoms onset. The transthoracic images were obtained using the Philips iE33 (Andover, MA). A single operator carried out all transthoracic echocardiographic measurements. Patients were examined in the dorsal decubitus position. Transthoracic echocardiographic images were obtained with the 3MHz phased array transducer. The left anterior descending coronary artery was viewed in the parasternal short axis plane. Coronary arteries appeared as linear tubular structure. The wall thickness was measured off-line by expert echocardiographers (Figure 1). The LADCA wall thickness measurements were obtained from the outer edge to the inner edge of the line representing the vascular wall. The reader was blinded to any clinical data and was free to choose any frames that he believed well visualized the LADCA wall. All measurements were obtained on 3 frames, and the results were averaged. Clear images were obtained in all the study participants. There were no significant inter (p=0.89) or intra-observer (p=0.30) variability in LADCA wall thickness readings.

Coronary arteries appeared as linear tubular structure. The wall thickness was measured off-line.
Statistical analysis
Continuous variables were tested for normality of distribution. Transformations were applied for non-normally distributed variables. Differences between the LADCA wall thickness in RA patients and the matched control group were analyzed by 2-sample (independent) Student’s t-test. Association of LADCA wall thickness with age, continuous CV variables, and disease activity variables were evaluated using linear regression analysis. The 2-sided probability values of p<0.05 were considered statistically significant. For all the analysis, Stata 10/SE statistical software (Stata Corp, Texas, USA) was used.
Results
Clinical features
Fifteen RA patients and 20 control subjects with matched 10 RA participants were included in the study. Demographic details, RA characteristics, and laboratory values of 15 RA patients at first presentation are shown in Table 1. None of the RA patients or the control participants had previous CVD/CBD or DM. There were no significant differences in the history of ever smoking, current smoking, hypertension, hyperlipidemia, or family history of CVD/CBD between the 2 groups. Systolic and diastolic blood pressure, level of cholesterol, triglyceride, HDL, LDL, and cholesterol levels between control participants and RA patients, revealed no significant difference (results not shown). Among RA patients, the mean age at the time of diagnosis was 54 (26-78 years), with no significant difference in age between males (57 ± 13.6 years) and females (51 ± 16 years). The mean duration of RA symptoms at the time of scanning was 2 ± 4 (range 1-12) months.
Demographic details, RA characteristics, and laboratory values of 15 RA patients at first presentation.
Left anterior descending artery wall thickness in RA patients and their matched controls
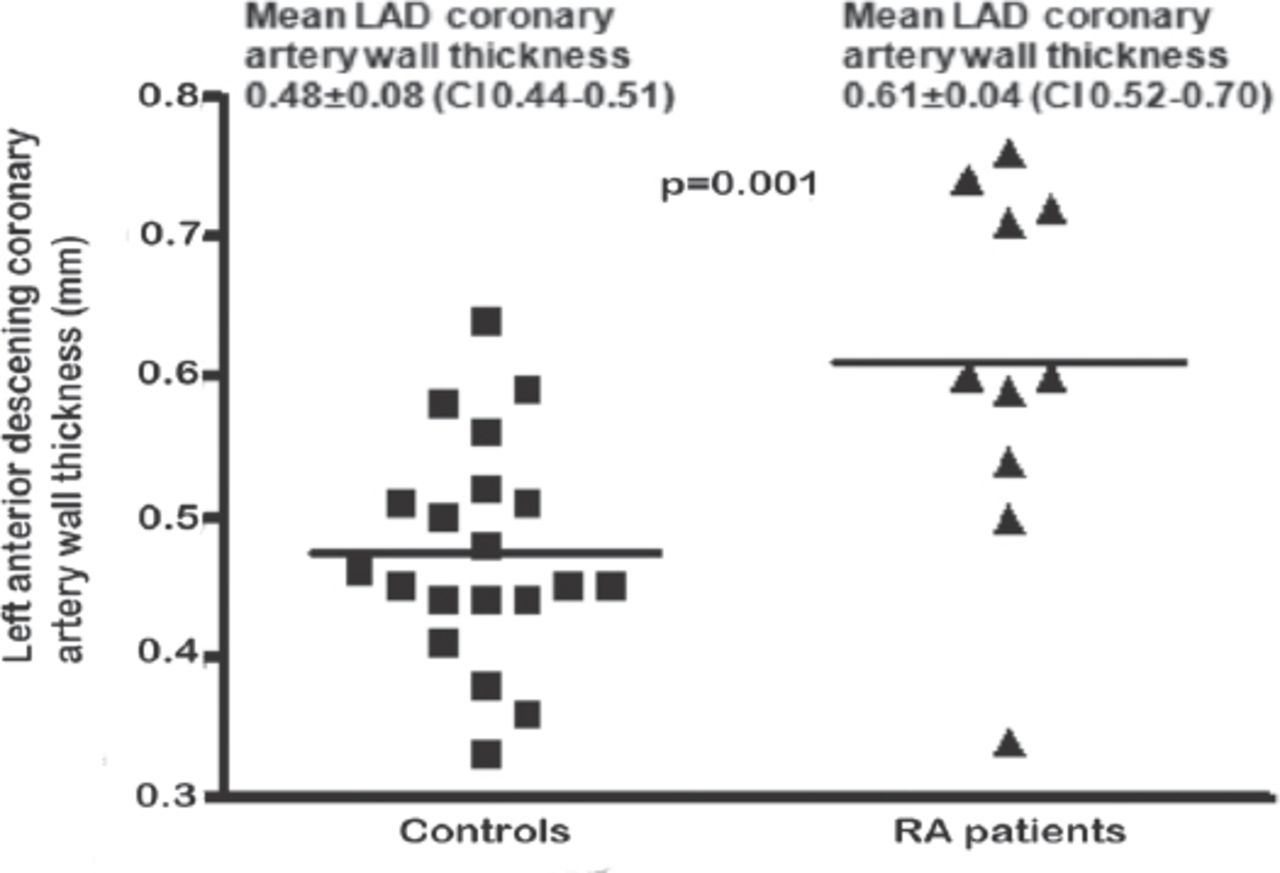
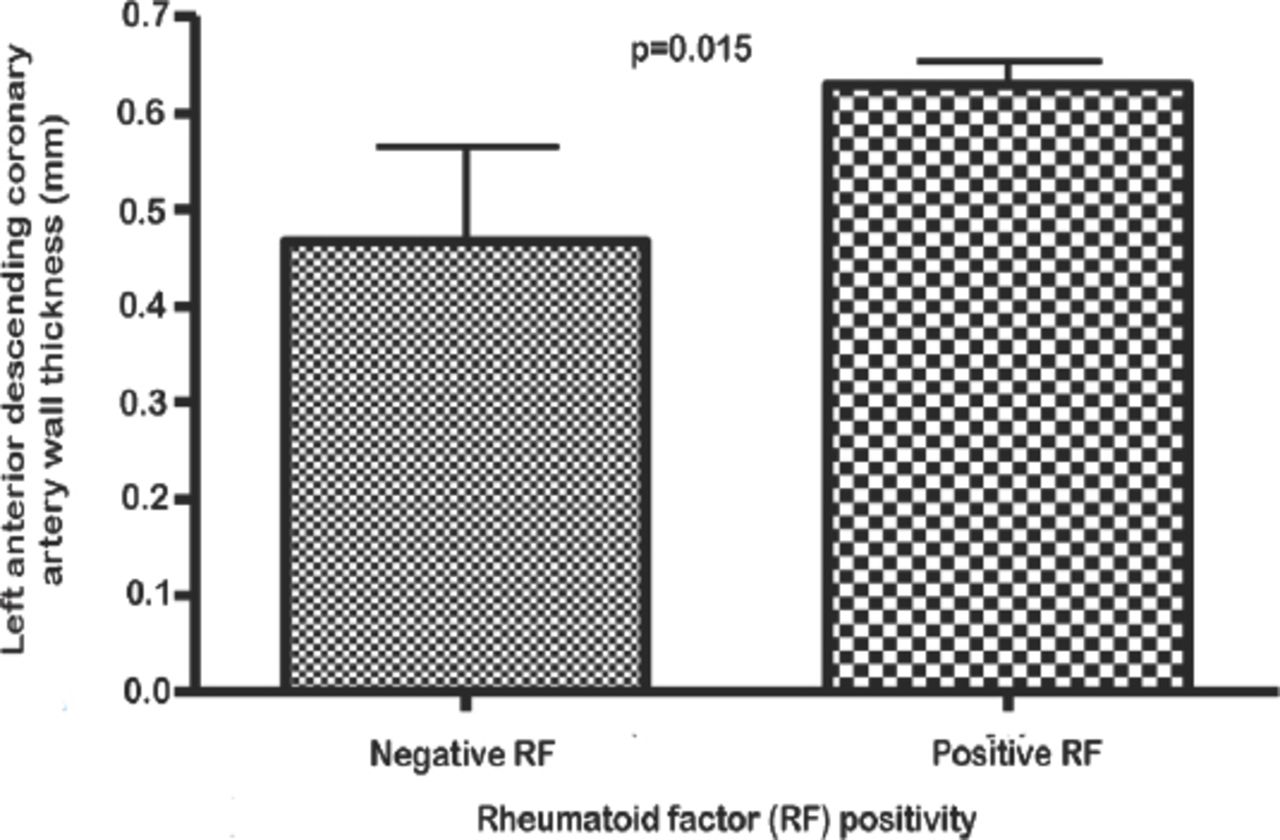
The LADCA wall thickness was measured in all early RA patients and control subjects. Despite the fact, that the cardiovascular risk factors did not differ significantly between RA patients and control group, however, the LADCA wall thickness was significantly increased (p=0.001) in patients with early RA (0.61 ± 0.04 mm, CI: 0.52-0.70), than among their matched controls (0.48 ± 0.08 mm, CI: 0.44-0.51), (Figure 2). Within the 15 early RA patients, univariate modeling revealed that LADCA wall thickness was related to Disease Activity Score (p=0.025, ß-coefficient 0.066, CI: 0.010 - 0.122) and to the PGADA at RA onset (p=0.006, ß-coefficient 0.003, CI: 0.001 - 0.005), in positive linear relationship. LADCA wall thickness was higher among RA patients with positive RF (p=0.015, CI: 0.53 - 0.66), (Figure 3).
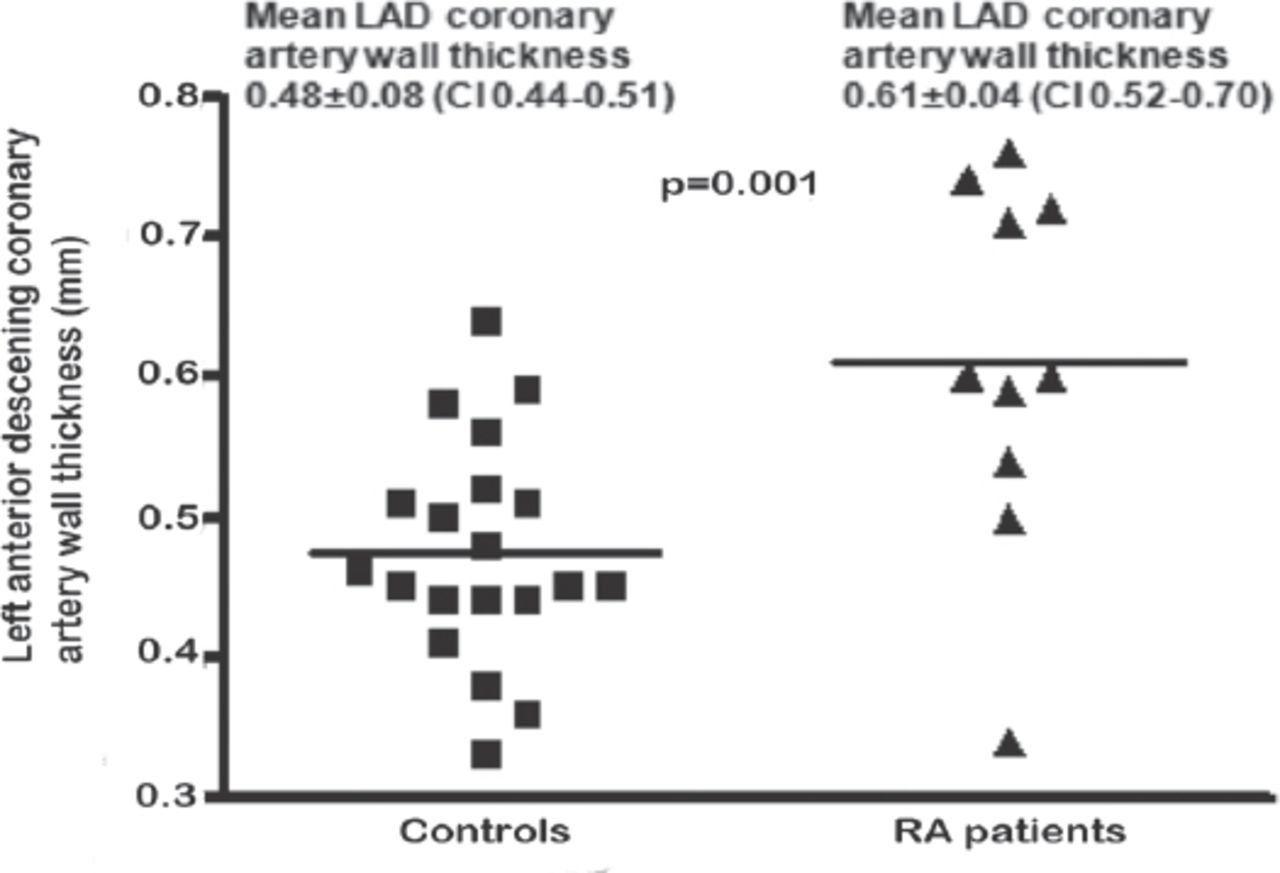
Left anterior descending coronary artery wall thickness (mm) in rheumatoid arthritis (RA) patients versus control group.
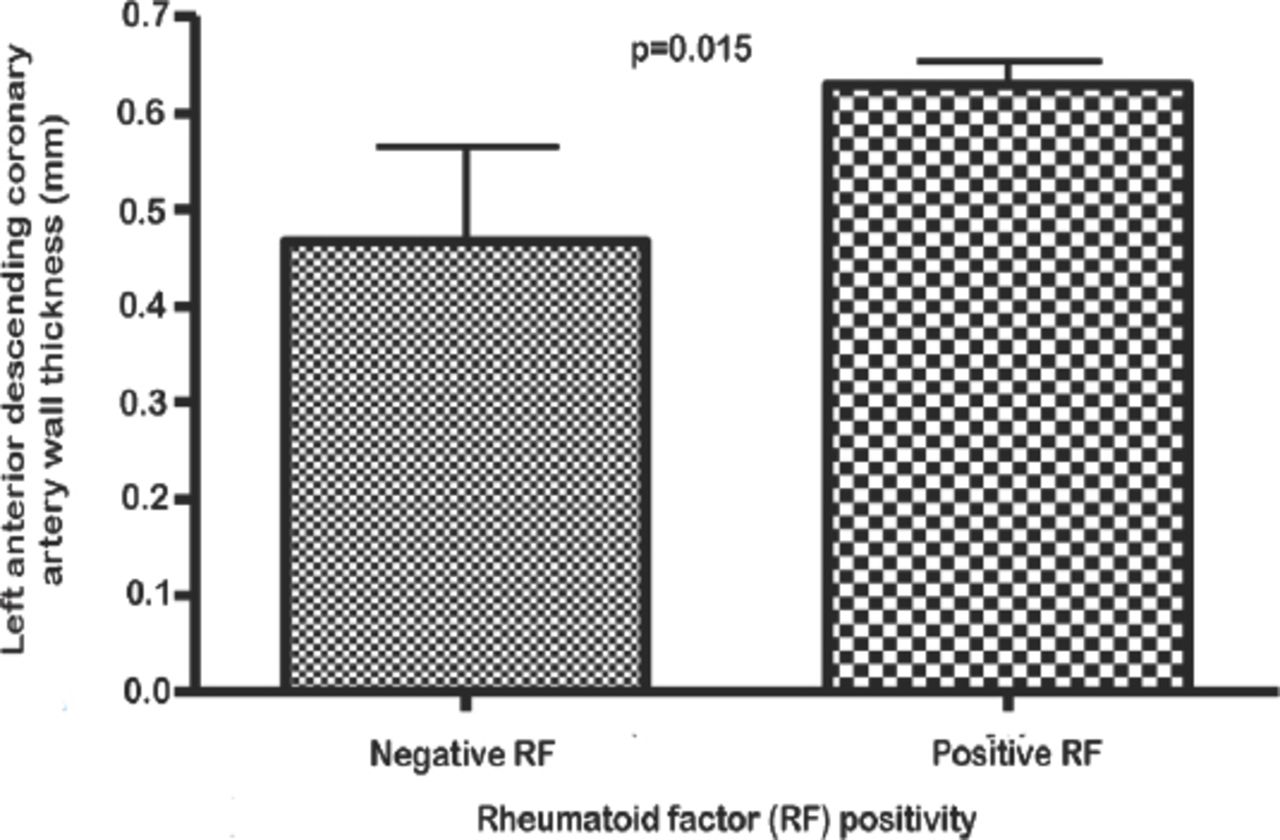
Left anterior descending coronary artery wall thickness (mm) in rheumatoid factor (RF) positive rheumatoid arthritis (RA) patients versus RF negative RA patients.
Discussion
These patients have higher chances of coronary arteries atherosclerotic problems compared to healthy subjects matched for age, gender and CVD risk factors.5 Atherosclerosis is a slowly progressive disease affecting coronary arteries as well as the large and medium-sized arteries.14 It has been demonstrated that changes in the size of the coronary artery lumen are not adequate for the diagnosis of subclinical coronary atherosclerosis because the disease is considered to be present in the arterial wall before luminal changes are evident.15 Therefore, detecting the progression of atherosclerosis requires an evaluation of variations in the coronary arterial wall thickness.14 Transthoracic echocardiography has been demonstrated to be a valid, feasible and reliable technique for measurement of distal LADCA diameter,16 and coronary wall thickness.16,17 The distal portion of the LADCA positioned close to the chest wall16 facilitates the scanning process. Furthermore, since coronary artery disease is a diffuse process, and the LADCA is the most frequently involved vessel, the coronary segment we scanned should represent an adequate sample of the coronary vasculature for the detection of subclinical atherosclerosis. Such noninvasive technique would permit the early detection of coronary atherosclerosis, and consequently, reducing the unfortunate coronary events, even in asymptomatic RA patients.18 The previous study showed that the standard LADCA thickness is 0.357 ± 0.06 mm for males and 0.25 ± 0.03 mm for females.19 Moreover, the LADCA thickness could be as high as 0.78 ± 0.3 mm in patients with coronary atherosclerosis.20 The mean LADCA thickness in this study was found to be 0.48 ± 0.08 mm for healthy control and 0.61 ± 0.04 mm for early RA patients. Differences between our measurements and any other study using the same techniques could be justified by presence of inflammatory activity in RA patients and population characteristics of the participants. In addition to this the LADCA wall thickness exhibited a significant correlation to the Disease Activity Score, PGADA, and to RF positivity. Furthermore, the variation in readings may also be due to the difference of recording site, or the transducer frequency. Unfortunately, we did not find any previously published report regarding LADCA wall thickness measurement in early RA patients to compare our outcomes. In addition to LAD coronary intima US, other new cardiovascular risk imaging techniques are continually being proposed, such as computed tomography (CT) and coronary magnetic resonance (CMR). CT can be used for coronary artery calcium score (CACS) or coronary angiography (CA). It has been reported that patients with long-term RA have coronary artery calcification which is associated with inflammatory activity.19 Although it has been suggested that CACS is a simple test to estimate the degree of calcification within the coronary arteries and it is a direct measure of early atherosclerosis.20 A more recent study suggests that some patients identified as low risk with traditional scoring methods would fall into higher risk categories with coronary artery calcium scoring.21 Others found that high CACS can modify predicted risk obtained from Framingham scores alone, especially among patients in the intermediate-risk category in whom clinical decision making is most uncertain.22 Although increasing CACS content is generally predictive of a higher likelihood of ischemia, its absence does not eliminate the possibility of flow-limiting coronary artery disease.23 On the other hand, CT requires the administration of iodinated contrast medium that might be associated with intolerance symptoms or renal impairment. Furthermore, the patients are exposed to ionizing radiation which is higher than in invasive CA.24 As a result, CMR angiography has been introduced to overcome these limitations. CMR is associated with non-invasive visualization of the epicardial coronary arteries. Generally, CMR has high sensitivity and overall accuracy for detecting coronary artery diseases.25 However, coronary arteries with diameters less than 1.5 mm are not well visualized by CMR angiography that results in an unsuccessful rate of 13%-14%.26 Consequently, CMR has a lower diagnostic accuracy of distal coronary artery lesions than the CT.27 Other limitations of CMR include its expense and contraindications for patients with retained metal objects or old metallic medical prosthesis. Therefore, it is hard at this stage, with a limited data to compare LADCA thickness with the CACS or CMR but what favor LADCA thickness that it can be done in the clinic setting while the CACS test is usually done by a radiology technologist and is not an office-based technique. Nevertheless, with all the techniques LADCA, CTA and CMR presently have incomplete longitudinal prognostic data specific to RA patients to guide rheumatologist in using them in CVD risk stratification.
The strength of our study comes from matching controls for age and gender to RA patients without any comorbid conditions including CVD/CBD and DM. Since CVD is a diffuse process and it rarely spares the proximal LADCA (Hausmann, Friedrich, et al. 1996). Therefore, this segment of coronary artery proved to be a good sampling site for the detection of subclinical coronary artery disease among RA population. Additionally, it has been verified that high-resolution broadband transducer, TDTE have sufficient penetration and resolution to appraise the coronary artery wall thickness,20 that represent subclinical coronary atherosclerosis.
Our study has some limitations, as it involves only early RA patients, we cannot extrapolate our findings to all RA population. However, we showed that high-resolution transthoracic echocardiography is sufficiently sensitive to detect coronary atherosclerosis in early RA patients. Another limitation of the study is that it is difficult to distinguish that we have measured consecutively the same segment of the LADCA because of rotation and translational effects throughout the cardiac cycle. We tried to decrease this variability by maintaining the transducer in a fixed position throughout the scanning process.
This study supports our earlier published report about the presence of subclinical atherosclerotic changes among early RA patients.5 Furthermore, our results indicate that a transthoracic ultrasound examination of the LADCA could be a clinically valuable tool in the detection of subclinical coronary artery disease among RA patients.
In conclusion, this is the first study to demonstrate that LADCA wall thickness could be measured in early RA patients and these patients are at higher risk of developing coronary arteries atherosclerotic ailments compared to healthy subjects, matched for age, gender and cardiovascular risk factors.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. Dr. Fahda Alokaily is a member of the Editorial Team, and was therefore excluded from any final editorial decisions regarding this paper.
- Received June 19, 2018.
- Accepted November 5, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}