


Abstract
Objectives: To assess knowledge and practice levels in asymptomatic hyperuricemia (AH) and investigate predictors of urate-lowering therapy (ULT) misprescribing among primary health care (PHC) physicians.
Methods: A cross-sectional study was conducted among 201 PHC physicians from December 2017 to May 2018. A based clinical guidelines for hyperuricemia management from American Professional Organizations, a semi-structured questionnaire was administered to collect demographic and professional data; knowledge and practice levels in management of AH; and barriers to the management of hyperuricemia and gout, with focus of the misprescribing of ULT in AH. A 2-stage stratified sampling technique was used to select 4 PHC centers were from each of the 5 advisory sectors in Jeddah, Kingdom of Saudi Arabia; and to recruit a minimum of 10 eligible participants per primary health care center (PHCC). Binary logistic regression was used to analyze predictors of ULT misuse in AH.
Results: Only 32.8% participating physicians had adequate knowledge about AH. Regarding practice, while majority (88.1%) correctly recommended a low-purine diet and lifestyle changes to patients, almost half misprescribed ULT and 10.9% misprescribed non-steroid anti-inflammatory drugs. Lack of knowledge and awareness about guidelines were the most frequently self-reported barriers to adequate practice. Predictors of ULT misuse included the percentage of patients having gout (1-10%: OR=5.40, p=0.047) or receiving ULT (>10-20%: OR=20.02, p=0.001)among patients seen in clinic, attendance of rheumatology conferences (OR=2.55, p=0.017), and having a close relative with hyperuricemia or gout (OR=2.45, p=0.026).
Conclusion: There are inadequate levels of knowledge regarding AH among Saudi PHC physicians increasing risk of malpractice including misprescription of ULT and anti-inflammatory medications.
Asymptomatic hyperuricemia (AH) is defined as serum uric acid level >6mg/dL without the occurrence of specific symptoms such as gout and renal stones.1 This level corresponds to a significantly increased lifelong risk of occurrence of gout and matches the recommended target of urate-lowering drugs (ULDs) among gouty persons.2 Asymptomatic hyperuricemia is a general condition in men and is positively correlated with age and weight gain in both genders.3 Epidemiological studies have reported increased incidence of hyperuricemia in recent years. Possible factors include increasing prevalence of obesity and metabolic disorders, along with changes in dietary habits, particularly greater consumption of purine-containing foods and sugar-sweetened soft drinks.3-5 The pathophysiological mechanisms of AH involve overproduction of urate, inefficient urate excretion by kidneys, or both.6
Above a certain threshold, a fraction of soluble monosodium urate crystallizes and accumulates in the synovial fluid or other soft tissues; this leads to gouty arthritis attacks and chronic gout and joint damage.7 Furthermore, AH is associated with higher risk of hypertension, chronic kidney disease, coronary artery disease, diabetes, and insulin resistance syndrome.8-11
Unfortunately, there is a lack of consensus about the definition and management of AH, thus hindering understanding of this condition among both physicians and patients.2 In 2012, the American College of Rheumatologists (ACR) issued guidelines for the management of gout; however, no specific therapeutic measure was recommended for AH, even though it is a major precursor of gout and is frequently associated with subclinical deposition of urate in joints.2-15 The American College of Physicians (ACP) in turn published recommendations for the management of acute and recurrent gout; they advised against the prescription of ULT after a first gout attack and recommended caution in initiating prophylactic ULT using in patients with recurrent gout attacks. These cautions are related to the lack of evidence regarding treatment efficacy in situations with infrequent gout flares and concerns about side effects.12
In addition to the unclear ACR and ACP guidelines of AH management, the literature contains conflicting reports regarding the usefulness of treating AH, both to reduce the risk of progression to gout and to prevent complications such as renal deposits of urate crystals.15-19 Cost-benefit analyses for both symptomatic treatments and ULT should be taken into consideration.14
Consequently, management of AH may be highly inconsistent, especially among non-specialists such as PHC physicians. This entails a high risk of malpractice and misprescription, which may in turn lead to high morbidity and expenditures. Thus, this study was designed to provide insight into the current knowledge and practice levels regarding AH among physicians in Kingdom of Saudi Arabia, and to investigate factors and predictors of ULT misprescribing along with perceived barriers to management of AH.
Methods
During the period December 2017 to May 2018, we conducted a cross-sectional study among physicians practicing as family medicine doctors (Family Medicine Board graduates) or general practitioners or in other specialties (internal medicine, obstetrics-gynecology and geriatrics specialists) in the Ministry of Health (MOH) PHCCs in Jeddah, Kingdom of Saudi Arabia. Jeddah contains 46 PHCCs distributed across 5 geographic sectors. Physicians of both genders, all ages, and all nationalities practicing in MOH PHCCs for at least one year were eligible. The study was approved by the Directorate of Health Affairs, MOH in Jeddah, kingdom of Saudi Arabia. All the data obtained from the study were blinded and thus, informed consent was not required.
A 2-stage stratified sampling technique was used in this study. Stage 1: 4 PHCCs were selected from each of the 5 sectors using a simple random sampling technique. Stage 2: convenience sampling was used to recruit eligible physicians present at the time of data collection, with a minimum of 10 participants per PHCC.
Data collection
The semi-structured English-language questionnaire included the following parts: Demographic and professional information such as age, gender, specialty, years of practice, and average number of patients seen per day; perceptions about AH, including its definition, correlation with gout, and awareness about its major causes; knowledge about AH (subscales included pathophysiology, common etiological factors, and dietary recommendations for people with hyperuricemia); level of practice in AH management (subscales included history taking, physical examination, evaluation of comorbid conditions, complementary investigations, and treatment/management of AH, including medication prescribing patterns); perceived barriers to the management of hyperuricemia. The questionnaire was developed based on hyperuricemia management guidelines from the ACR and the ACP.12,20 Two rheumatologists and an epidemiologist reviewed the questionnaire items for validity. The questionnaire was tested among 20 eligible participants to assess its clarity, and internal consistency was measured using Cronbach’s alpha.
Scoring system
The knowledge part of the questionnaire allowed calculation of a knowledge score; related questions had incorrect (score=0) or correct (score=1) answer options. The knowledge score was calculated as the number of correct answers (range: 0-40). Further, subscores were calculated on knowledge subscales (pathophysiology factors and mechanisms, dietary recommendations) to explore the most deficient areas.
Data collection technique
Participating PHCCs were visited during regular working hours. Physicians who were present during the visit were invited to participate in peer-to-peer interviews lasting 18-25 minutes.
Statistical methods
Data were coded, entered, and analyzed using Statistical Package for Social Science (SPSS) version 21 for Windows (IBM Corp., Armonk, NY, USA). Knowledge score distribution was analyzed using Kolmogorov-Smirnov and Shapiro-Wilk tests concluding to non-normal distribution. Adequate knowledge was defined using an assumed cut-off >20/40 correct answers (50% of the maximum possible score). Chi-squared tests were used to analyze factors associated with misuse of ULT. Multivariate binary regression was used to analyze the predictors of and independent risk factors for ULT misuse in AH. A p-value<0.05 was considered significant.
Results
The study included 201 PHC physicians; 66.2% were female, 65.2% were married, and mean age was 34.53±6.82 years. Of the participants, 58.7% were family medicine specialists and 28.4% were general practitioners. The majority (59.2%) had more than 5 years of practice. More than half of the participants (54.2%) had more than 20 patients per day. The average percentage of patients with gout or receiving ULT was 12.79%, and 64.7% reported that ≤10% of their patients had gout or received ULT (results not presented).
Questionnaire internal consistency
As shown in Table 1, the overall knowledge scale showed high internal consistency (Cronbach’s alpha=0.837). Knowledge subscales rated highly as well (pathophysiology: 0.767, factors/mechanisms: 0.756, and dietary recommendations: 0.887). Overall internal consistency for the practice scale was very high (Cronbach’s alpha=0.972), ranging from 0.830 for history taking to 0.961 for comorbidity evaluation. However, treatment management scale showed negative value of Cronbach’s alpha (-0.920) because one of the items had a negative covariance.
Internal consistency of the questionnaire and levels of knowledge and practice regarding asymptomatic hyperuricemia among primary health care physicians (N=201).
Perceptions about AH
Table 2 shows that among participating physicians, 64.7% correctly identified AH and gout as being different but related diagnoses; 84.6% chose the correct AH definition, 71.1% correctly identified urate hyperproduction, and 55.2% correctly identified decreased renal excretion as being possible mechanisms of hyperuricemia.
Perceptions about asymptomatic hyperuricemia including its definition, relationship with gout, and major mechanisms (N=201).
Knowledge and practice levels regarding AH
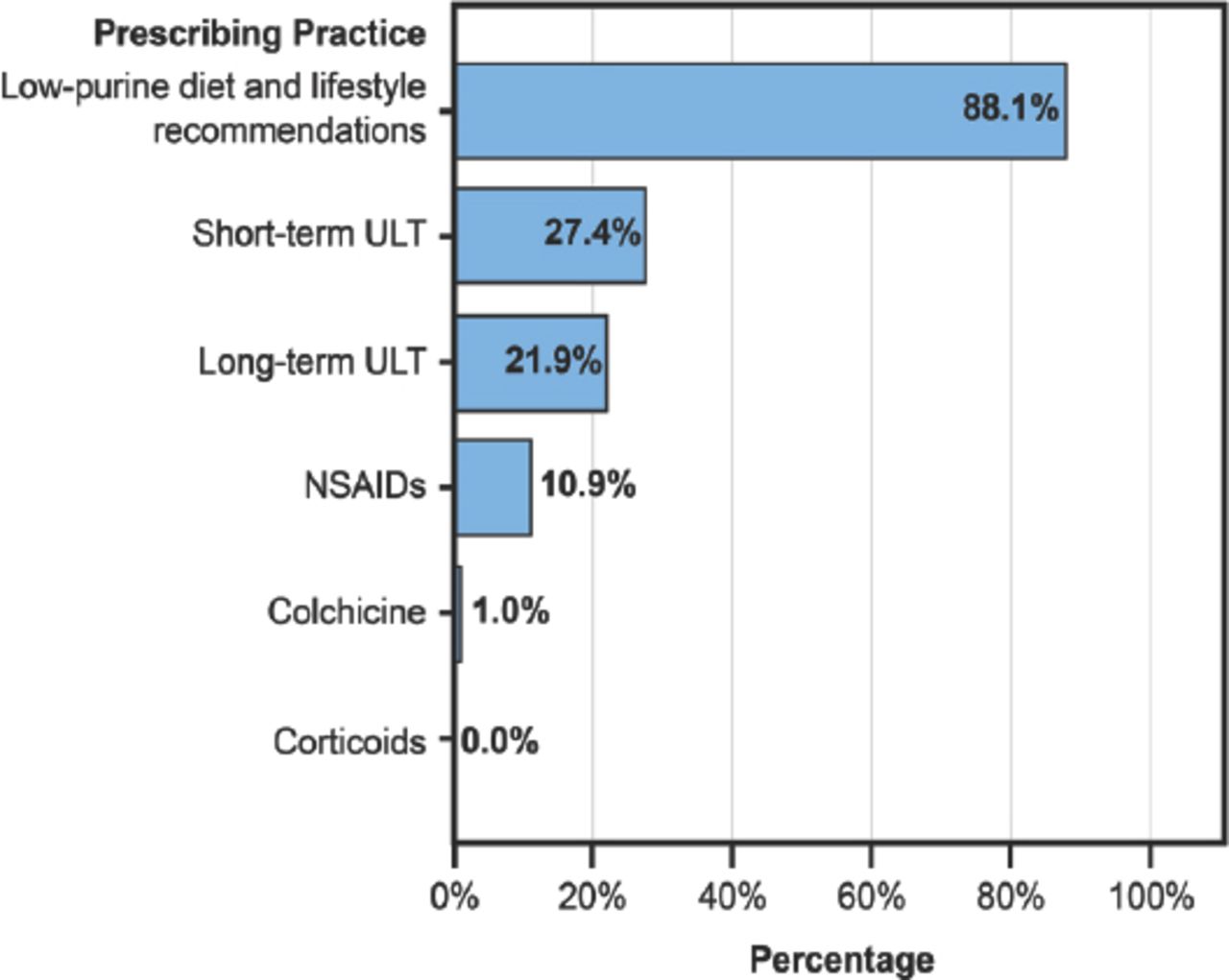
Table 2 showed that mean knowledge scores (18.1) was generally low, with only 32.8% of participants having adequate knowledge about AH by consideration of the used cutoffs. With respect of respective subscales, knowledge adequacy rates ranged from 3% (factors/mechanisms) to 62.7% (dietary recommendations); and practice adequacy rates ranged from 41.3% (physical examination) to 74.6% (complementary investigations). Management/treatment practice subscale was separately analyzed in and presented in Figure 1, showing that a majority of participants (88.1%) would recommend a low-purine diet and lifestyle changes to patients with AH, while 27.4% would prescribe short-term ULT and 21.9% would prescribe long-term ULT.

Prescribing patterns in asymptomatic hyperuricemia among primary health care physicians (N=201). Bars represent the percentage of participants who would prescribe the given therapeutic option for patients with asymptomatic hyperuricemia. ULT - urate-lowering therapy, NSAIDs - non-steroidal anti-inflammatory drugs.
Barriers to practice regarding AH
Figure 2 illustrates that lack of knowledge about the guidelines was the most frequently reported barrier to adequate practice in AH, followed by lack of awareness of the guidelines’ existence and inadequate knowledge about the disease.

Barriers to management of asymptomatic hyperuricemia among primary health care physicians (N=201). Bars represent the number of participants who declared that the given factor was a true), somewhat true, or false barrier.
Factors associated with ULT misuse in AH
Among all participants, 48.8% declared using or recommended the use of short-term and or long-term ULT in AH. Table 3 presents factors associated with ULT misuse in AH. Misuse of ULT was less reported among young physicians (p<0.001) and those with relatively short experience (p<0.001) compared to their counterparts. Misuse was also associated with the percentage of patients having gout or receiving ULT, displaying an inversed U-shaped relationship, with highest rates of misuse observed among physicians who declared that 10-20% of their patients having gout or receiving ULT. Paradoxically, attendance of rheumatology conference and having a close relative with hyperuricemia or gout were associated with higher rates of ULT misuse, compared to their counterparts. Analysis of knowledge score showed significant association of ULT misuse with knowledge about pathophysiology (p=0.039) but not with overall knowledge (p=0.513) or other knowledge subscales scores (p>0.050).
Factors associated with urate-lowering therapy misuse (N=201).
Predictors of ULT misuse in AH
The risk of ULT misuse in AH was independently associated with the percentage of patients having gout (1-10%: OR=5.40, p=0.047) or receiving ULT (>10-20%: OR=20.02, p=0.001), attendance of rheumatology conferences (OR=2.55, p=0.017), and having a close relative with hyperuricemia or gout (OR=2.45, p=0.026) (Table 4).
Predictors of urate-lowering therapy misuse in asymptomatic hyperuricemia (N=201).
Discussion
The clinical relevance of AH and whether it should be treated has long been controversial.6 Nevertheless, in accordance to ACR and ACP guidelines, physicians should be aware of hyperuricemia management practices, including clinical and etiological diagnosis, lifestyle and dietary recommendations, proper monitoring of serum urate levels, and screening for eventual complications.15,17,18,21 Nonetheless, some major discrepancies have been highlighted between ACP guidelines and recommendations published by other rheumatology expert panels, such as the ACR and the European League Against Rheumatism (EULAR); and these discrepancies result from differences in the fundamental approach. The ACP approach is focused on patient-perceived benefits and burdens and clinically-driven management strategy; while the rheumatology expert recommendations are based on a pathophysiological approach considering the chronicity and progressiveness of the disease with the subsequent disorders, which represents a more evidence-based approach.22
Findings of this study suggest a high prevalence of hyperuricemia and gout among patients visiting PHCCs, as one-third of the physicians estimated that more than 10% of their patients had gout or received ULT. Few epidemiological studies on gout and hyperuricemia in Kingdom of Saudi Arabia exist; Al-Arfaj,23 estimated the prevalence of hyperuricemia as 8.4% in 2001. Since that time, prevalence may have increased in Kingdom of Saudi Arabia as it has worldwide, especially given increases in obesity and diseases associated with poor lifestyle and dietary habits.3-5
Approximately, one-half of the participating physicians were able to correctly define AH as elevation of serum urate level without presence of gout symptoms. However, knowledge about hyperuricemia and AH was overall poor to moderate, notably in factors/mechanisms underlying hyperuricemia (only 3% adequacy).
Practice in AH was marked by high rate of ULT misuse, as almost half of the physicians declared that they would prescribe either short-term or long-term ULT for AH, which was predicted by several factors. In a 2014 Saudi study by Mustafa,6 84.1% of physicians would recommend allopurinol treatment for AH, suggesting a higher level of misprescription than seen here. Allopurinol prescription for AH is a frequent practice among United Kingdom’s physicians as well.24 Further, ULT misprescribing may be associated with the lack of screening for medication interactions and inadequate follow-up; this increases the risk of severe side effects and complications. Other potentially misprescribed medicines advocated by physicians participating in this study included non-steroidal anti-inflammatory drugs (NSAIDs) (10%) and colchicine (1%). These medications are indicated for pain during gout attacks or prophylactically in chronic gout whereas AH is by definition characterized by absence of clinical justification for such treatment.12,13
According to ACR and ACP guidelines, the sole therapeutic options warranted for AH are a low-purine diet and lifestyle changes; 88.1% of the physicians in this study concurred. In contrast, Mustafa,6 reported earlier that only 42.5% of physicians provided dietary advice for patients with AH. Dietary and lifestyle recommendations are crucial to reduce health risks associated with hyperuricemia, and include limiting intake of high-purine foods, as well as controlling obesity, smoking, and alcohol consumption.4,14,23
We observed that less than half (41.3-47.8%) of physicians achieved adequate history taking, physical examination, and comorbidity evaluation in patients with AH. Diagnosis of AH depends on ruling out conditions such as arthritis or nephrolithiasis that may evoke symptoms similar to gout, or even undiagnosed gout attacks. For the latter, diagnosis and management of gout, rather than AH, is warranted. History taking also facilitates screening for family history of gout, which may uncover important genetic background factors.25 Furthermore, history taking enables physicians to rule out external causes of hyperuricemia such as urate-elevating medications.12 Similarly, physical examination may detect signs of arthritis, tophi, synovitis, or any comorbidity (such as kidney disease, metabolic syndrome, or obesity) that may affect AH diagnosis or management.12,26,27 Complementary investigations may be helpful in detecting subclinical arthritis or urolithiasis (through imaging, namely ultrasound) or detecting urate overproduction (through measurement of urine uric acid levels).2,16
This study showed paradoxical association of attendance to rheumatology conference with higher risk of ULT misuse; which may be explained by physicians having gaps in rheumatology being more interested in related conferences. The other inconsistency association includes having a close relative with hyperuricemia which was predictive for higher risk of ULT misuse. Unfortunately, for both issues, the questionnaire does not include sufficient details to explain these inconsistencies.
Study limitations
Females, young doctors (up to 5 years of practice), and family physicians were relatively overrepresented in the sample. This could be due to selection bias, as there was some difficulty obtaining consent from relatively older physicians. The study questionnaire showed very good internal consistency in all scales/subscales. However, it should be further validated using the test-retest method and by measuring its reliability in different populations.
In conclusion, this study shed light on major gaps in knowledge and practice regarding AH among physicians in western Kingdom of Saudi Arabia, especially concerning factors leading to hyperuricemia and their respective mechanisms, as well as treatment prescribing patterns with high rate of ULT misuse. Lack of awareness and knowledge about international guidelines and inadequate knowledge about the disease were primary reasons for low confidence and practice levels among the surveyed physicians. Notably, physicians who attended conferences and meetings in rheumatology had significantly higher risk for ULT misuse. Combined, these observations suggest important gaps in formal training in hyperuricemia/rheumatology, emphasizing the need for strengthened theoretical and clinical training to reduce the risk of malpractice, associated morbidity, and resulting costs.
Acknowledgment
The authors would like to thank all the physicians who participated in this study.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 24, 2018.
- Accepted November 4, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.