


Abstract
A mechanical heart valve thrombosis during pregnancy is one of the most lethal conditions to experience due to its detrimental effects on both mother and fetus. Cardiac surgery during pregnancy is reserved for cases where medical treatment fails due to harmful maternal and fetal effects. A 24-year-old female in the 38th week of pregnancy was admitted to the emergency room with aggravated dyspnea, tachypnea, and palpitations. She had 2 previous cardiac operations in her medical history. A stuck mechanical valve was diagnosed in the mitral position via transthoracic echocardiography, which had resulted from her decision to cease taking warfarin when planning to become pregnant. In pregnant patients who have prosthetic mechanical valve thrombosis, surgical approach should be considered depending on the conditions of the mother and the baby. When emergency delivery of the baby is feasible, emergent surgical treatment should be utilized for patients who are in critical condition.
In all pregnancies, the incidence of heart diseases is rising between 1% and 4%. The rheumatic mitral valve diseases (RMVD) are the most commonly acquired heart disease in pregnancy. Mitral stenosis is the most common valvular pathology between RMVD.1,2 A mechanical heart valve thrombosis (MHVT) during pregnancy is a rare complication, but it can be a life-threatening condition and has a high mortality rate. Patients with prosthetic mechanical valves (PMV) who stop anticoagulant treatment prior to or during pregnancy are at high risk for MHVT.2,3 Mechanical heart valve thrombosis during pregnancy is one of the most lethal conditions due to its potential detrimental effects on both mother and fetus. Cardiac surgery during pregnancy is reserved for cases where less-invasive medical treatments fail or are contraindicated due to their harmful maternal and fetal effects. In such cases, a surgeon has to decide that a surgical approach is warranted by the conditions of the patients. In this case report, we present our perioperative strategy and surgical approach for a pregnant patient with MHVT who ceased anticoagulant therapy prior to and during her whole pregnancy.
Case Report
Patient information
A 24-year-old female who was in her 38th week of pregnancy was admitted to the emergency room with aggravated dyspnea, tachypnea, and palpitation. She was referred to our hospital with a preliminary diagnosis of pulmonary embolism. She had 2 previous cardiac operations in her medical history. First, she had been operated on for a secundum type atrial septal defect at the age of 11. Then at the age of 13, she had received a prosthetic mitral valve replacement due to severe mitral regurgitation. She had no other history of family and genetic disorder.
Clinical findings
In the emergency room, physical examination revealed severe dyspnea, tachypnea (respiratory rate: 35 per minutes) and bilateral leg swelling. Her oxygen saturation was 90%, blood pressure was 120/70 mmHg and pulse rate was 110/minute. Metabolic acidosis was present in her arterial blood gas sample. Her cardiothoracic ratio was 55% at chest x-ray. She also exhibited diffuse pulmonary congestion and bilateral pleural effusion. The past medical history and final follow-up of the case was summarize in Table 1.
Timeline summary of the case.
Diagnostic assessment
Firstly, we also thought pulmonary embolism because of the potential risk of computerized tomographic pulmonary angiography to the mother and the baby, we had to prefer transthoracic echocardiography (TTE) as a less invasive diagnostic assessment. On TTE, immobile and mobile thrombi were found to be blocking valve movement on both sides of her mitral prosthesis surfaces. Across her mitral prosthesis, the peak pressure gradient was 30 mmHg, and the mean gradient was 20 mmHg.
The baby was determined to be mature via ultrasonographic examination. The fetal heart rate was normal, and the mother was experiencing no uterine contractions. The obstetrician decided to deliver the baby via cesarian section (C/S) before the cardiopulmonary bypass was carried out.
Therapeutic intervention
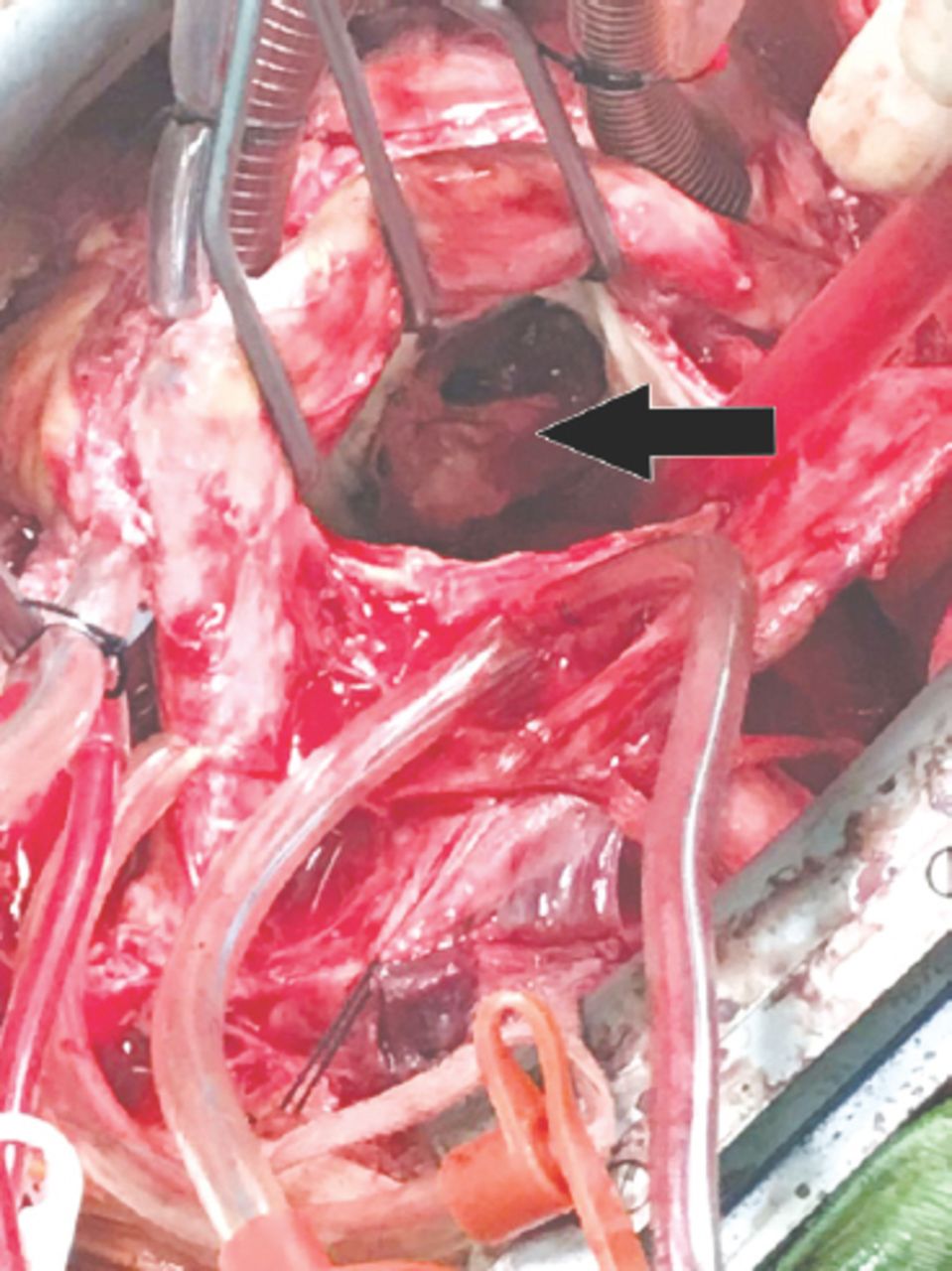
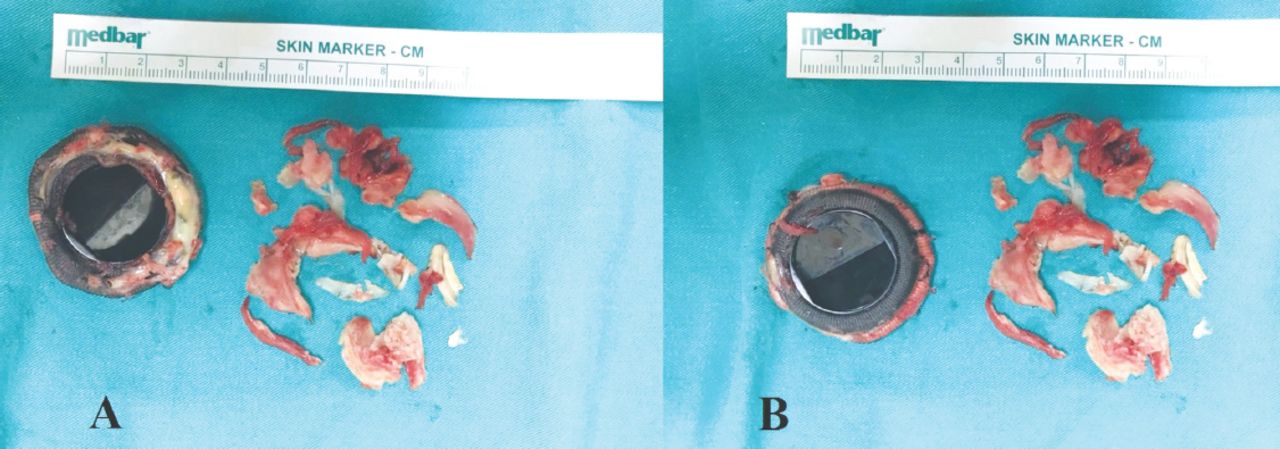
The 3800 grams baby was delivered in good health. After the delivery of the baby, uterine stimulant medications (uterotonics/oxytocics) were administered during and after the cardiac operation to avoid the uterine atony. Cardiovascular surgery team started the operation after the obstetrician completed C/S. The right femoral artery and vein were prepared for emergency situations. After sternotomy, all adhesions were divided with blunt and sharp dissections. A cardiopulmonary bypass (CPB) was established through aortic arterial and bicaval venous cannulation. Antegrade blood cardioplegia was performed for cardiac arrest. After left atriotomy, mitral valve exploration revealed severe pannus tissue and thrombi on both sides of mechanical valve’s hinge area and sewing cuff (Figure 1). All pannus tissue and thrombus material were cleaned away, and the stuck mechanical mitral valve was removed. The stitch line of the removed mitral prosthetic valve was covered with pannus on both sides of the valve (Figure 2). A new, 31 mm bileaflet mechanical mitral valve was then implanted in the patient. The operation took place at St. Jude Medical, Inc, Minneapolis, MN, USA. Approximately 3000ml serous fluids were aspirated from both pleural spaces totally.

Intraoperative atrial view of severe pannus tissue and thrombi (arrow) on mechanical valve’s hinge area and sewing cuff.

Pannus tissue can be seen on both A) atrial and B) ventricular sides of the removed mitral prosthetic valve.
Follow-up and outcomes
Following the cardiopulmonary bypass, she had no need for inotropic agents. She was able to be extubated 24 hours after the operation. Approximately 6000ml of pleural effusion were drained from the bilateral chest tubes during postoperative 10 days. Chest tubes were removed at the postoperative 11th day. She was discharged on the 23rd day, after the operation, in good health. She was administered in our outpatient clinic 6th month after the operation. Transthoracic echocardiography revealed functional mitral prosthesis. She had no complaint and her international normalized ratio was in therapeutic range during this period.
Discussion
Many significant changes in the cardiovascular system and hemostasis occur during pregnancy. During the first trimester, uterine blood flow (UBF) typically accounts for 3% of cardiac output. Uterine blood flow increases to 10-15% of cardiac output during the 3rd trimester. As a result, the cardiac workload increases. The women therefore experience a state of hyper coagulability and an increasing risk of thromboembolism during pregnancy.4 In the pregnant patient, while fibrinolytic activity decreased, coagulation activity and platelet count increased.2
Anticoagulation management is very important during pregnancy. It has been reported that the risk of MHVT increases substantially for pregnant individuals, by as much as 25% in those who have prosthetic mechanical valves and are not on any anticoagulant treatment.3 This means that the patient described in this report had a very high risk of MHVT, because she ceased her anticoagulant treatment prior to and throughout her pregnancy. The treatment strategies for heart diseases in pregnant patients fall into 2 categories: medical treatments and surgical approaches. Medical treatment strategies and follow-up are preferred until the 30th week of gestation, after which surgical treatment can be performed according to both mother’s and baby’s conditions. When considering surgical approaches, urgent or emergent surgery options may be considered based on the patient’s hemodynamic status. The neonatal mortality rate during maternal cardiac surgery is higher than 90% before 25 weeks’ gestational age; however, the rate drops below 15% after the 30th week of gestation.5 The patient discussed in the above case report was operated on in the 38th week of gestation in an emergency condition, which meets all of the above recommendations.
In pregnant cardiac patients, the most common reasons for fetal loss are associated with fetal stress and fetal bradycardia. The standard method for monitoring fetal heart rate and uterine contractions to identify fetal distress is external ultrasound tococardiography (EUT). It is critically important to monitor how a fetus heart rate responds throughout surgical and pharmaceutical therapies when its mother is undergoing such treatments.3 With the patient in this case, we observed the fetal heart rate and uterine contractions via EUT up until the baby was delivered. Because of the increasing tone and contractions of uterus in hypothermia during CPB, placental gas exchange impairs. The hypothermia below 35°C has a higher risk in terms of fetal mortality. Avoiding from hypothermia during CPB is very important to prevent fetal stress. According in previous studies, maintaining a high flow rate of circulation (20%-40% higher than non-pregnant patients) during this procedure and to keep a mean perfusion pressure greater than 2.5 L/m2/min is crucial. During CPB, the maintenance of the mean arterial pressure (MAP) above 70 mm Hg and using the pulsatile perfusion would be sufficient for improvement of fetal outcomes.2,6 In our case, hypothermia was able to be used during the CPB, because the baby was delivered before the procedure was undertaken.
The relatively high rate of fetal mortality resulting from cardiac surgery during pregnancy has been shown to be associated with the using of CPB in pregnant patients. The maternal mortality rate during these surgeries is similar to that of non-pregnant women. In surgery using CPB during the 3rd trimester, pregnant patients have demonstrated a high risk of fetal loss and complications.2 If the mother has a good hemodynamic status, babies that are at or near term delivering via C/S before CPB was suggested by many authors in previous studies.7,8 In this case, we decided to deliver the baby before undertaking the mother’s CPB. When medical treatments fail in pregnant MHVT patients, an emergent surgical approach can be utilized successfully to ensure both maternal and fetal survival. To increase the chance of success in surgical treatment with CPB for pregnant MHVT patients, the surgical team should take care of the patient to avoid deep hypothermia, maintain a high flow rate of circulation (>2.5L/min m2) and use pulsatile perfusion to maintain a MAP of more than 70 mm Hg. Surgical approaches that include CPB must be avoided whenever possible prior to 24 weeks’ gestation.
Surgical approaches in pregnant patients who have MHVT should be preferred depending on the conditions of the mother and the baby. Earlier in gestation, when the fetus is most sensitive (before 30 weeks), emergent cardiac operations for stuck valves can be performed, but they carry a high risk of mortality for the baby. When emergency delivery of the baby is feasible, emergent surgical treatment should be utilized for patients who are in critical condition.
Acknowledgment
All authors have given written permission to be acknowledged. An informed consent was obtained from the patient. Lastly, we would like to thank Scribendi (www.scribendi.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 14, 2018.
- Accepted November 7, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.