


Abstract
Objectives: To estimate the benefits of non-invasive ventilation (NIV) used immediately after planned postextubation in patients with chronic respiratory disorders.
Methods: Cochrane Library, PubMed, the Chinese BioMedical Literature Database of clinical trials (CBD) and Embase were searched for pertinent studies by 2 trained investigators. Pooled odds ratios and 95% confidence intervals (CIs) were calculated by employing both fixed-effects and random-effects models.
Results: Eight studies enrolling 736 patients were included in the meta-analysis. Compared with general oxygen therapy, NIV used immediately after planned extubation in patients with chronic respiratory disease reduced the reintubation rate (p=0.02), ventilator-associated pneumonia (VAP) incidence rate (p=0.000), and ICU mortality (p=0.002) and increased the level of PO2 (p=0.03).
Conclusion: Non-invasive ventilation used immediately after planned extubation seems to be advantageous for decreasing the reintubation rate, VAP incidence, and ICU death rate in patients with chronic respiratory disease.
Chronic respiratory disorders include airway diseases, occupational lung diseases, interstitial diseases, pulmonary vascular diseases and genetic diseases and severely affect people’s quality of life.1,2 More than one billion people suffer from chronic respiratory disorders worldwide. Non-invasive ventilation (NIV) is an efficient method for providing ventilatory support and improves the clinical results of patients with acute respiratory failure, particularly those with chronic respiratory disorders.3-6 Although NIV used early after planned extubation has a vital function in a wide variety of clinical situations, its effect in chronic respiratory disorders remains unclear. Previous studies have concluded that non-invasive ventilation (NIV) used prophylactically in postextubation (use of NIV immediately after extubation) could reduce the rate of reintubation, mortality, length of stay, and occurrence of pneumonia.7-10 However, Jun Duan reported that NIV used prophylactically in postextubation was not correlated to reintubation.11 Su CL suggested that prophylactic use of NIV in postextubation was not beneficial for reducing the rate of extubation failure and mortality.12 However, few studies have assessed the role of NIV used immediately after planned postextubation in patients with chronic respiratory disorders. Therefore, we attempted to perform a summarized meta-analysis to confirm the relationship between NIV used immediately after planned extubation and chronic respiratory disorders.
Methods
This meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.13 (Supplementary Material)
Search strategy and criteria
We used the Population, Intervention, Comparison, and Outcome (PICOS) strategy to obtain relevant articles published through August 2016 in the Cochrane Library, PubMed, the Chinese BioMedical Literature Database of clinical trials (CBD) and Embase; to identify potential randomized controlled trials (RCTs); and then to assess the relationship between the use of NIV immediately after planned extubation and chronic respiratory disorders. The search strategies used the following text and MeSH terms: (“chronic respiratory disorders” OR “chronic respiratory diseases” OR “CRDs” OR “COPD” OR “chronic obstructive pulmonary disease” OR “chronic bronchitis” OR “chronic pulmonary vascular disease” OR “chronic pulmonary interstitial diseases” OR “pulmonary genetic diseases” OR “occupational lung diseases”) and (“NIV” OR “noninvasive ventilation” OR “non-invasive ventilation” OR “noninvasive positive-pressure ventilation” OR “nasal ventilation” OR “NIPPV” OR “ BiPAP” OR “CPAP” OR “bilevel positive airway pressure” OR “continuous positive airway pressure”) and (“planned extubation” OR “planned postextubation” OR “postextubation” OR “extubation” OR “after extubation” OR “after postextubation”). The literature search strategies were created on the basis of the following eligibility criteria: (1) the study language was English and Chinese language articles available in full text; (2) the study population included patients with chronic respiratory disorders; (3) the interventions were NIV versus conventional oxygen therapy; (4) the study design was randomized controlled trials; (5) the reported outcomes included reintubation rate, intensive care unit (ICU) mortality, ventilator-associated pneumonia (VAP) incidence, arterial partial pressure of oxygen (PO2), heart rate (HR), and intensive care unit (ICU) length of stay; (6) the reported indexes contained country, publication year, the mean, standard deviation, outcome incidence, sample size, and gender; and (7) the publication status was journal articles. Studies were eliminated if they met any of the following criteria: (1) article type: reviews, letters, laboratory research or animal experiments; (2) language other than English or Chinese and (3) patients without chronic respiratory disorders.
Data collection and quality assessment
We independently extracted and assessed the data, which included publication information, demographic characteristics and outcome variables. Any inconsistencies were resolved by group discussion. A quality assessment of each study was performed independently by 2 authors using the Jadad scale.14,15 (Supplementary Material)
Statistical analysis
We examined the relationship between NIV used immediately after planned extubation and chronic respiratory diseases based on the mean, sample size, standard deviation in each group, the number of males and females, study design, country, year of publication for each study and study outcome incidence rate. The standard mean difference (SMD) or odds ratio (OR) was considered statistically significant when the 95% confidence interval (CI) did not include 1.16 Cochrane Q-test and I2 index were used to determine the heterogeneity across studies. When p≥0.05 or I2≤ 50%, a homogeneous fixed-effects model was implemented to merge effect sizes. We considered a p<0.05 or I2>50% to indicate heterogeneity, and we evaluated the sources of heterogeneity by means of sensitivity and subgroup analyses. If the sources of heterogeneity were not identified , a random-effects model was applied.17 A sensitivity analysis was conducted in which the difference between the pooled effect size and total effect size was observed in the remaining studies after individual studies were removed one by one. Subgroup analyses were performed by classifying study data. For binary data, the Mantel-Haenszel (M-H) method for the fixed-effects model and the DerSimonian-Laird (D-L) method for the random-effects model were used to pool the OR and 95% CI. For continuous data, the inverse variance (IV) method for the fixed-effects model and the D-L method for the random-effects model were used to pool the SMD and 95% CI.18,19 Funnel plots, Egger’s test and Begg’s test were used to examine publication bias.20,21 All reported p-values were 2-sided, and p-values<0.05 were considered to indicate statistical significance. The STATA software (version 12.0; Stata Corporation, College Station, TX, USA) was used to analyse the data.22
Results
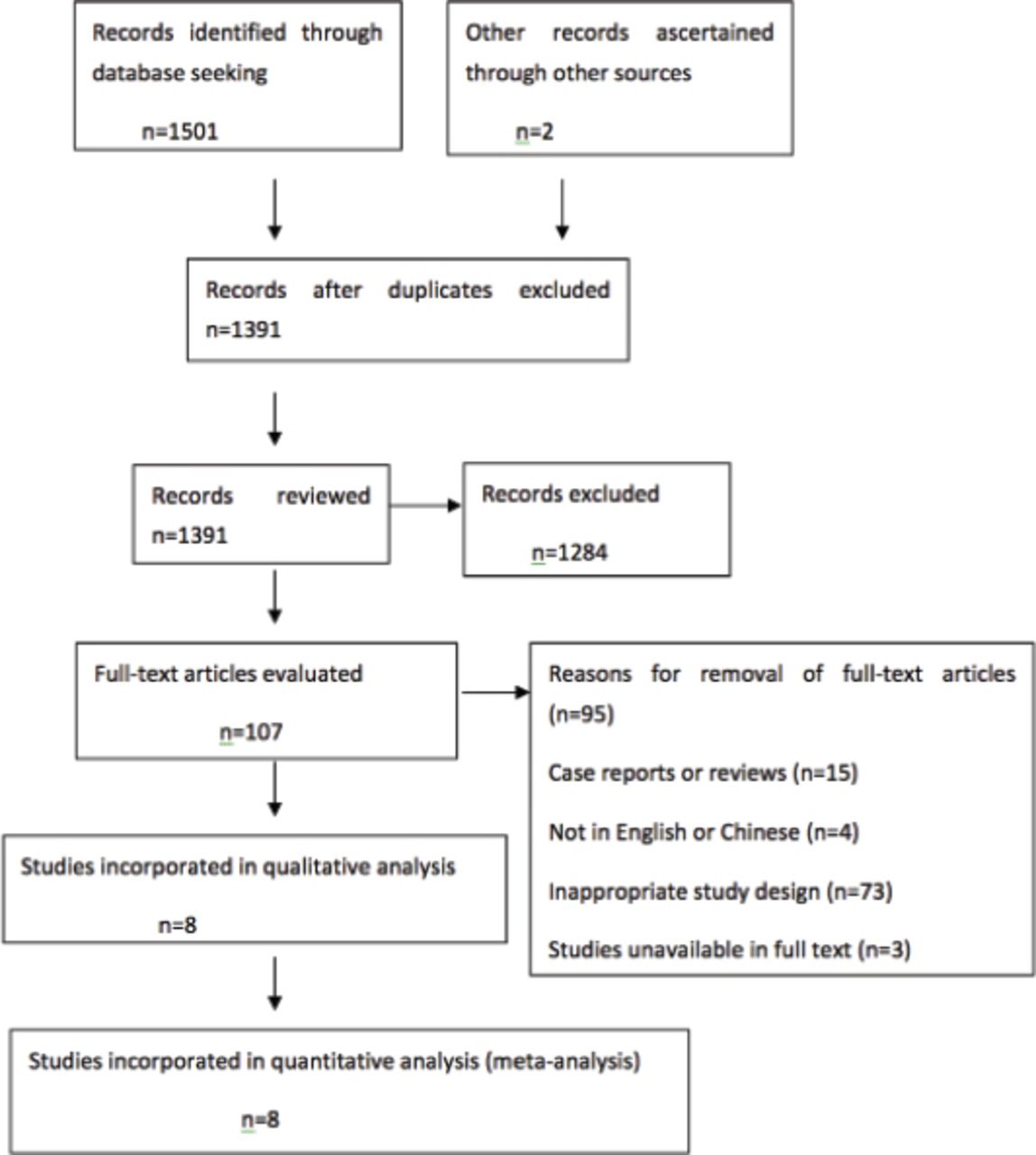
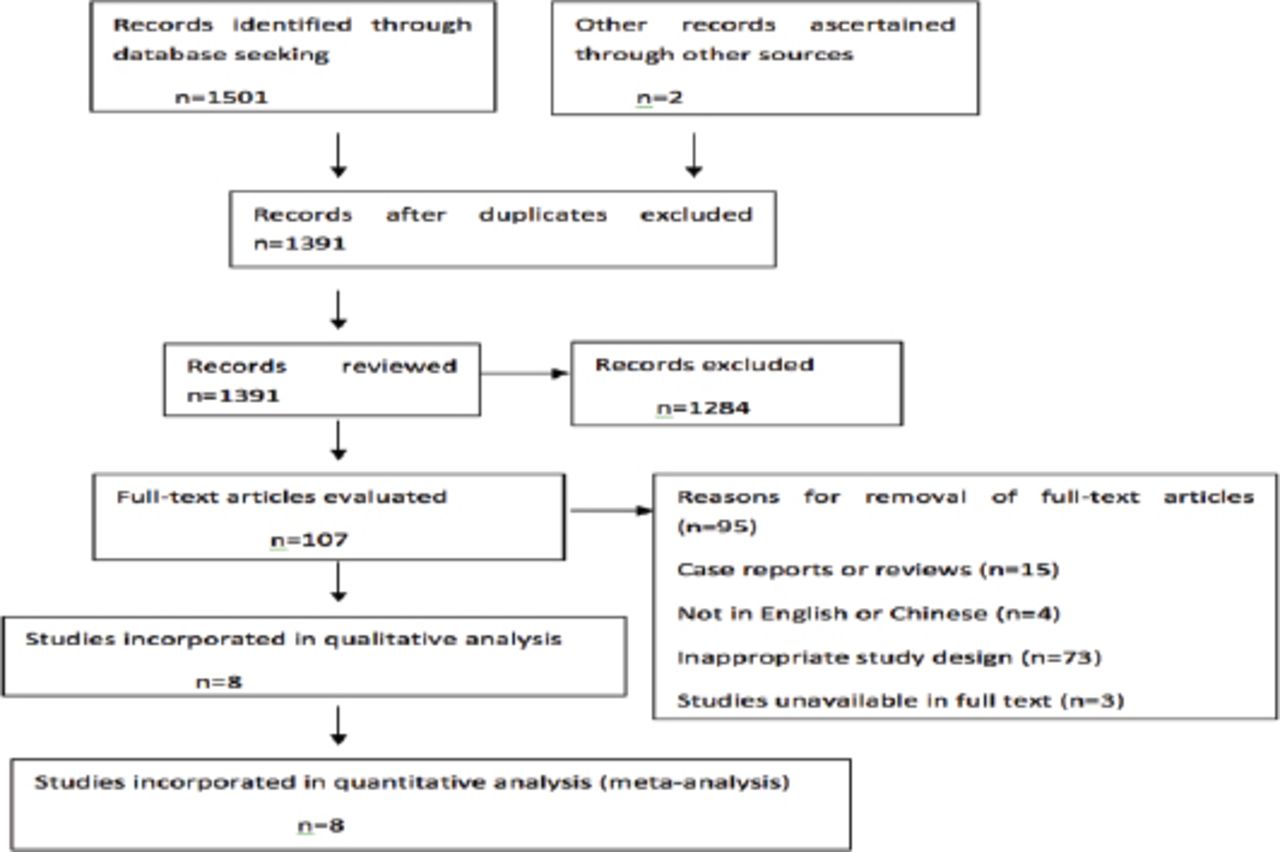
After the first retrieval of studies, a total of 1,501 potentially relevant studies were preliminarily included in our study, and 1,394 irrelevant or duplicate articles were excluded after scanning the titles and abstracts. The full texts of the articles were searched for the remaining 107 articles. In the end, 8 studies met all the criteria for inclusion in the analysis (Figure 1).23-30 Table 1 shows the demographic characteristics of the incorporated studies. These 8 studies included 372 NIV treatments and 364 controls, and all were randomized controlled trials. Four studies were conducted in China, 2 in Spanish, one in Brazil, and one in Australia.23-30 The average age of the NIV treatments was 50.79-76.2 years, while it was 48.88-78.2 years in the control group. The quality of the articles was evaluated by the Jadad scale. All of the incorporated RCTs scored 3/5 on the Jadad. Table 2 presents a summary of the reported statistics for the research indexes after extubation.
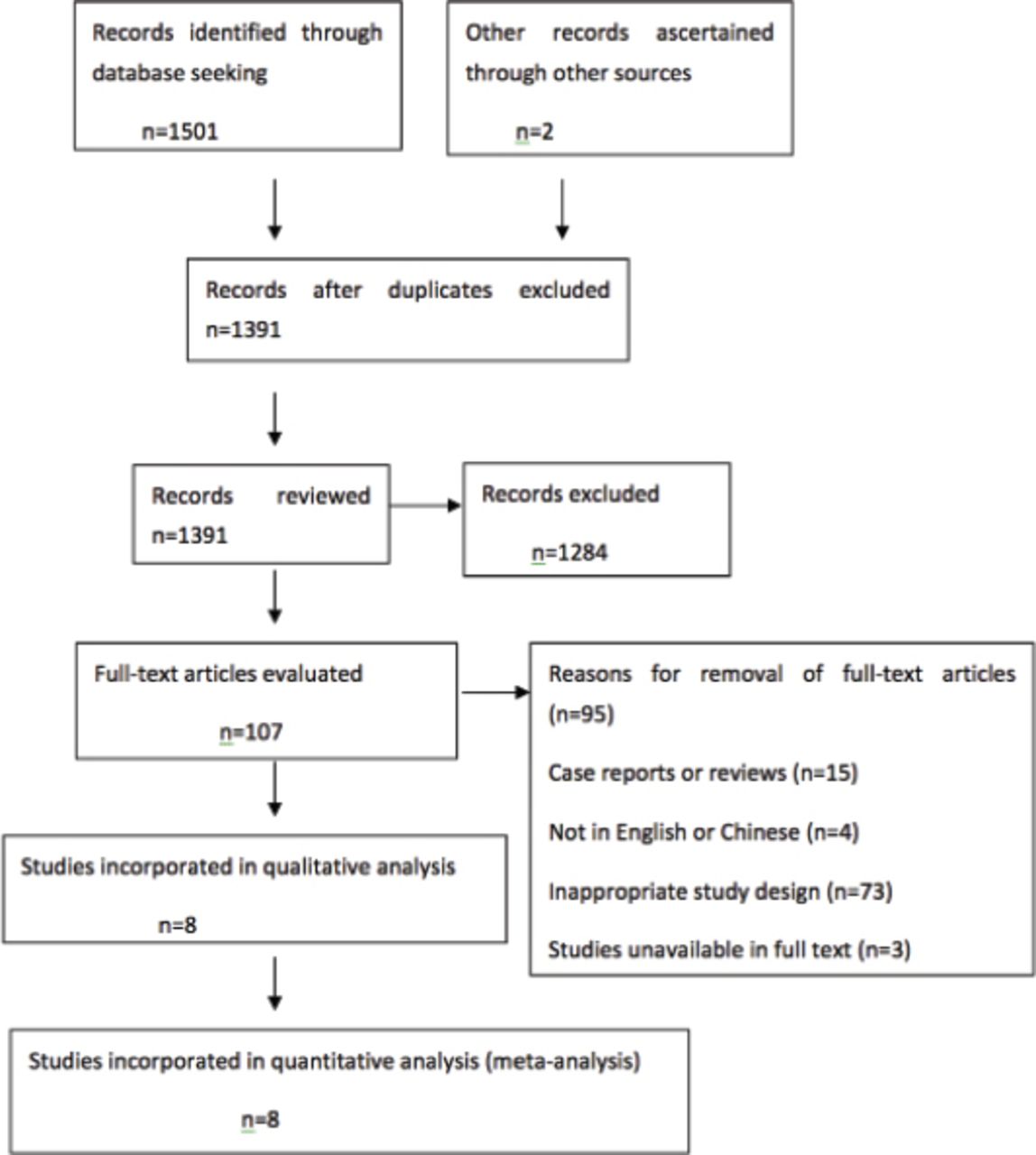
Diagram of study selection process.
Characteristics of the incorporated studied in the meta-analysis.
Summary of reported statistics for research indexes after extubations.
Reintubation
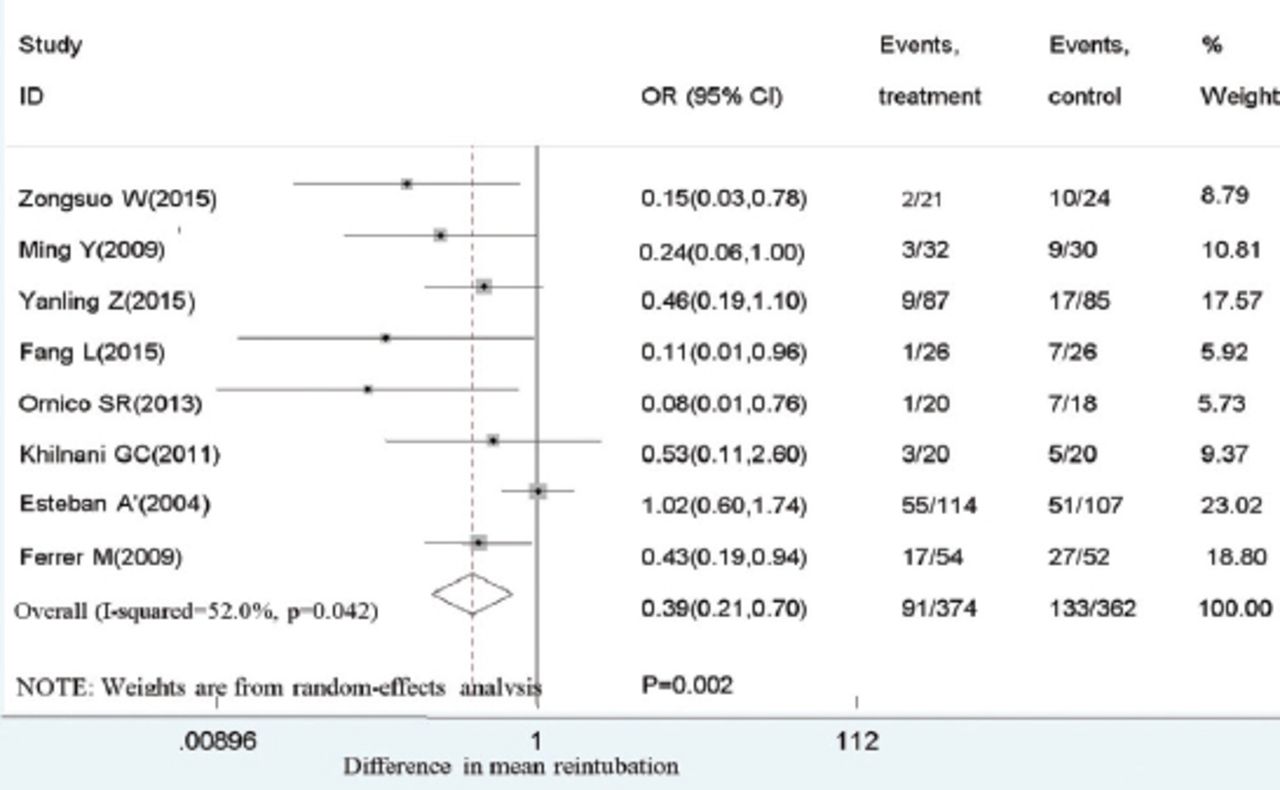
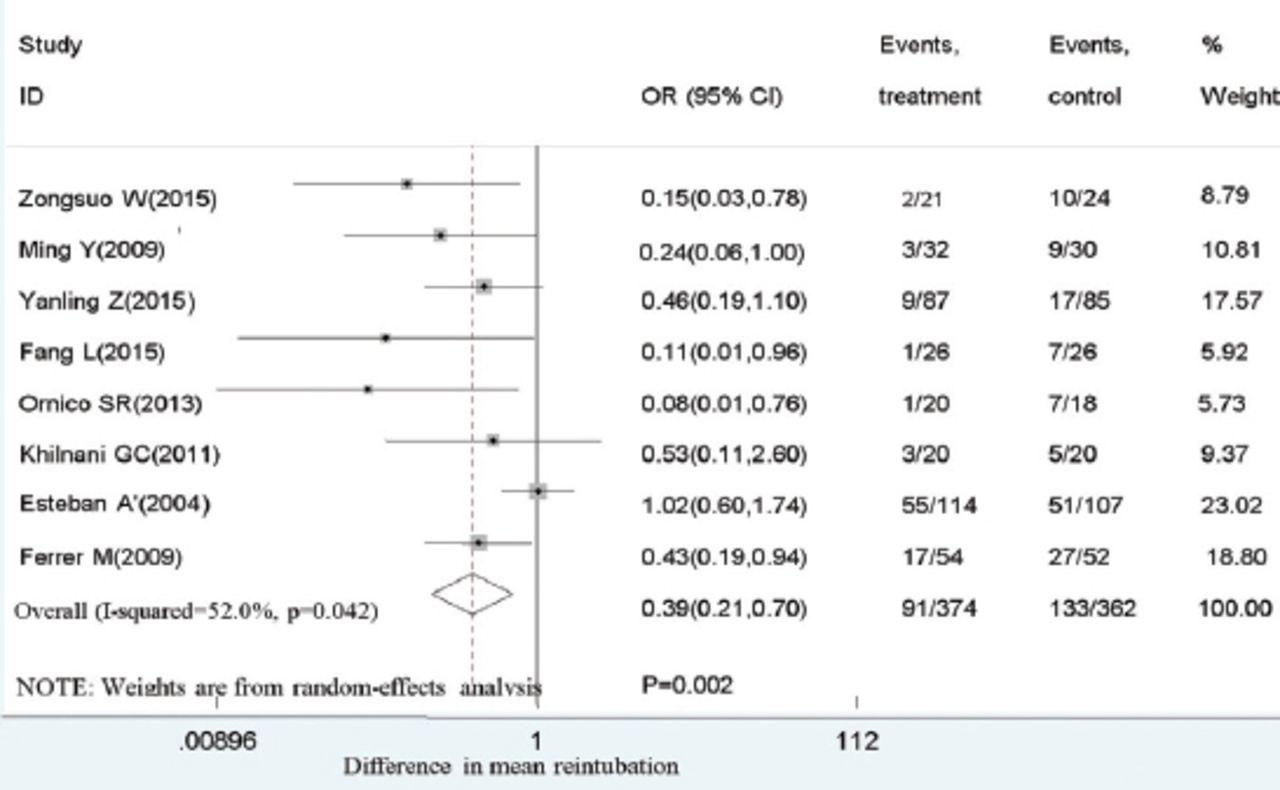
Eight studies showed a correlation between NIV and reintubation rate. Compared with conventional oxygen therapy, NIV reduced the rate of reintubation when it was used immediately after planned extubation for those with chronic respiratory diseases, as shown in Figure 2.

Effect of non-invasive ventilation (NIV) vs conventional oxygen therapy on reintubation after extubation. OR - odds ratio, 95%CI - 95% confidence interval.
VAP
Two studies showed a relationship between NIV and VAP incidence. Compared with common oxygen therapy, NIV reduced the incidence of VAP when it was applied immediately in planned postextubation for those with chronic respiratory disorders, as shown in Figure 3.
Effect of non-invasive ventilation (NIV) vs conventional oxygen therapy on ventilator-associated pneumonia (VAP) after extubation. OR - odds ratio, 95%CI - 95% confidence interval
ICU mortality
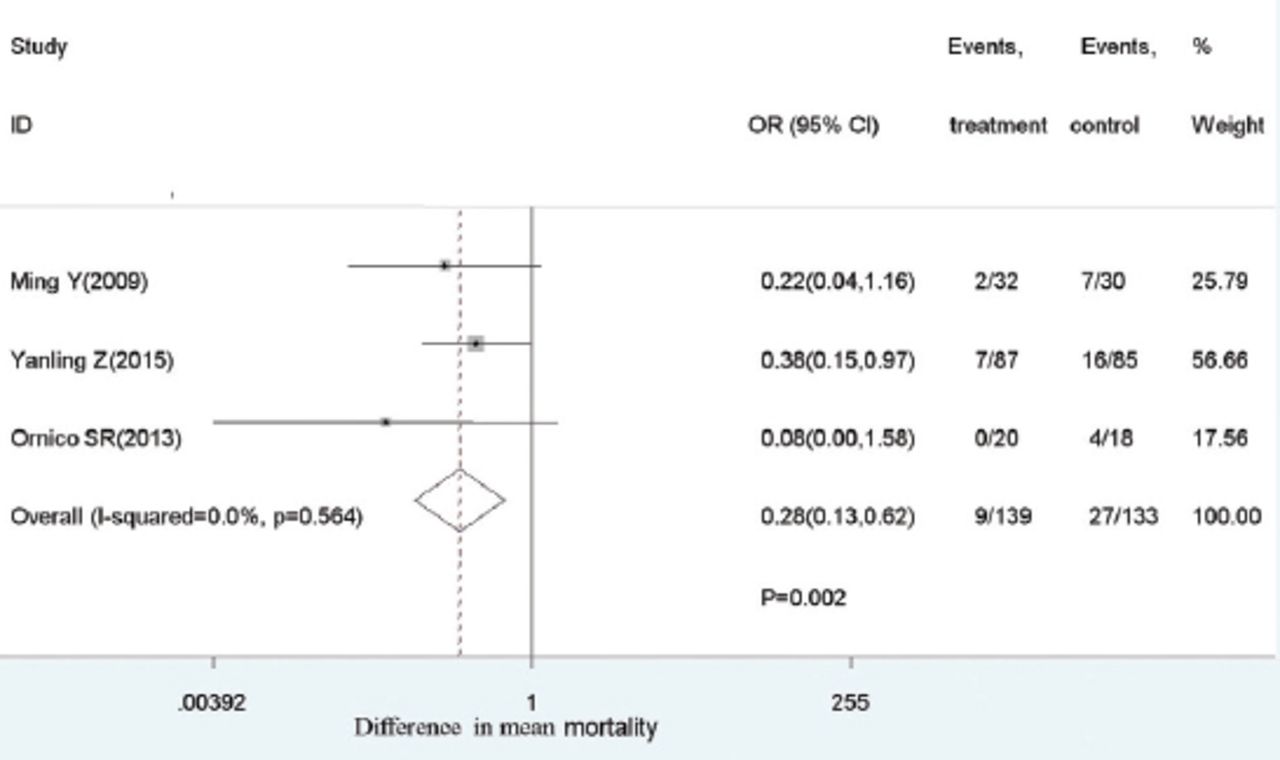
Three studies showed a connection between NIV and ICU mortality. Intensive care unit mortality was decreased by NIV when it was used immediately after planned extubation for those with chronic respiratory disorders in comparison with controls, as shown in Figure 4.

Effect of non-invasive ventilation (NIV) vs conventional oxygen therapy on ortality after extubation. OR - odds ratio, 95% CI - 95% confidence interval
Two studies showed an association between NIV and PO2. The level of PO2 was increased by NIV when it was used immediately after planned postextubation for those with chronic respiratory disorders compared to controls. However, the analyses showed that HR and ICU length of stay were not associated with NIV.
Heterogeneity and publication bias
Funnel plots, Egger’s test and Begg’s test showed no evidence of publication bias. Cochrane Q-test and I2 index showed that the parameter of reintubation exhibited mild heterogeneity, but the sources of this heterogeneity were not identified by sensitivity analysis or subgroup analysis.
Discussion
This meta-analysis shows that the use of NIV prophylactically in postextubation (use of NIV immediately after extubation), when compared with common oxygen therapy, can decrease the reintubation rate, the risk of VAP, and ICU mortality and increase the level of PO2 in patients with chronic respiratory diseases. This finding is different from that of studies in which NIV was used generally in postextubation (use of NIV in established postextubation respiratory failure). Lin C suggested that the use of NIV generally in postextubation for patients should be monitored closely.8 Krishna B31 concluded that the therapeutic use of NIV after extubation (use of NIV prior to the establishment of respiratory failure) was not beneficial for patients.In our study, although the use of NIV prophylactically in postextubation was found to increase the level of PO2, we believe that NIV was found to be not beneficial for PO2 because only pooled patients from 2 available studies were included in the analysis, and there are many factors that influence the level of PO2, such as chronic chest disease.
A literature review found that no systematic review has included proof of the effect of NIV used immediately after planned extubation for patients with chronic respiratory diseases. Respiratory therapy, particularly mechanical ventilation, is being continuously developed internationally, but there are still many countries lagging behind, such as China. Mechanical ventilation plays an important role in respiratory therapy, and decision makers must fully understand this issue. This meta-analysis adds to the proof of the effect of NIV used early in postextubation.9,10,32 It emphasizes the valuable role of NIV used immediately in postextubation in decreasing the rate of reintubation, the risk of VAP and ICU mortality. At the same time, it also emphasizes the potential role for specialty development among researchers.
Implications for practice and future research.Based on this literature review, NIV used immediately in postextubation appeared feasible for patients with chronic respiratory diseases. However, NIV is mainly operated by respiratory therapists (RTs), who function as part of respiratory treatment. Respiratory therapists (RTs) are an emerging medical profession and provide diagnosis, treatment and care to patients with cardiopulmonary dysfunction or abnormality under the guidance of doctors; their responsibilities include supplying different ventilation treatments and oxygen therapy for critically ill patients. Respiratory therapy originated in America and has developed for more than 50 years, playing an important role in rescuing patients with critical and respiratory diseases. Respiratory treatment units have been established in hospitals in most countries and regions where the respiratory treatment system is internationally available. However, the work of RTs has been provided by clinical doctors or nurses in China, where RTs are available in only a few large hospitals. It will take a long time for China to formalize respiratory therapy. Currently, there is no respiratory therapist license available in China, which may substantially contribute to the slow development of respiratory therapy.
In Germany, respiratory therapy has developed for more than 10 years. They have started to explore different levels of qualification aimed at achieving interprofessional teamwork.33 The role of RTs in mechanical ventilation, respiratory treatment and lung-protective ventilation has been demonstrated in some studies.34,35 However, in the current medical environment, viability of the RTs requires space for more autonomous and developed professionals who are as approved as other medical professions.36
With the improvement in the treatment level of critically ill patients, the demand for respiratory therapy is increasing and is becoming increasingly important. In the future, we should implement various measures to strengthen standardized training for RTs, to improve the level of respiratory therapy and to improve the effects of NIV. Second, the government should explore how to establish a well-organized and relevant system, such as an examination system for qualification. More professionals will thus be encouraged to participate in respiratory therapy. Third, we should pay attention to the value of respiratory therapists in respiratory therapy, particularly in mechanical ventilation.
This study still has some limitations. This meta-analysis incorporated only published studies and did not incorporate unpublished articles. The language and search terms were in English and Chinese. It is expected that this restriction has little or no influence on the conclusion of the meta-analysis. Heterogeneity was not found in this meta-analysis regarding intervention, gender or country; however, there were differences in our study outcomes. For some outcomes, only 2 to 3 studies were included, and pooled effect sizes were plausible. However, publication bias is unavoidable due to the small quantity of studies. Thus, we expect to conduct future studies.
In conclusion, this meta-analysis emphasized the effect of NIV used immediately after planned extubation in chronic respiratory diseases. There is much left to explore with regard to usage time, weaning time and selection of NIV mode. The correct use of NIV after planned extubation is also not very clear. Therefore, more rigorous and multicentre evaluation studies are needed in future studies.
Footnotes
Disclosure. The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
- Received October 29, 2017.
- Accepted December 25, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.