


Abstract
Fournier gangrene is a rapidly progressive necrotizing fasciitis of the perianal and genitourinary area. Although typically affects men, we present here a rare disease founding in a pregnant woman. An obese 36-year-old female patient in her third trimester of pregnancy presented with a history of perianal pain and swelling. She was subsequently diagnosed with Fournier gangrene and underwent emergency cesarean section with a surgical debridement. The key to successful outcomes in such a complicated presentation of Fournier gangrene includes a high index of suspicion, fluid resuscitation, rapid administration of broad-spectrum antibiotics, and an early interdisciplinary approach by multiple teams. This helps share decisions and balance the risk-benefit of the emergency caesarian section without delaying the surgical debridement.
Fournier gangrene is a rapidly progressive necrotizing fasciitis of the perianal and genitourinary area. The reported mortality rates have varied but the most recent evidence ranged it from 5% to 10%.1,2 It is a rare disease especially in women as the reported incidence is 1.6/100,000 of the male population with male cases outnumbering female cases at a ratio of 10:1 and the highest incidence is persons aged 50 to 70 years.3,4 Although typically affects men, we present here a rare disease found in an obese pregnant woman managed with unique multidisciplinary interventions.
Case Report
A 36-year-old female obese patient from Yemen, Gravida 4 Para 3, in her 34th week of pregnancy. She was in her usual state of health until 10 days before the presentation to our emergency department (ER) when she started to feel perianal pain during a prolonged period of travel (the timeline shown in Figure 1). Initially the pain was tolerable but for the last 3 days before the presentation, the pain significantly increased in intensity, and she developed perianal swelling and fever without any urinary symptoms, abdominal pain, change in the bowel habits, or vaginal or rectal bleeding. She initially visited a private clinic in which she underwent multiple attempts of needle aspiration that failed to collect any pus; therefore, she was diagnosed with cellulitis and hemorrhoids and was discharged on lactulose and oral Amoxicillin Clavulanate tablet 875 mg/125 mg every 12 hour.

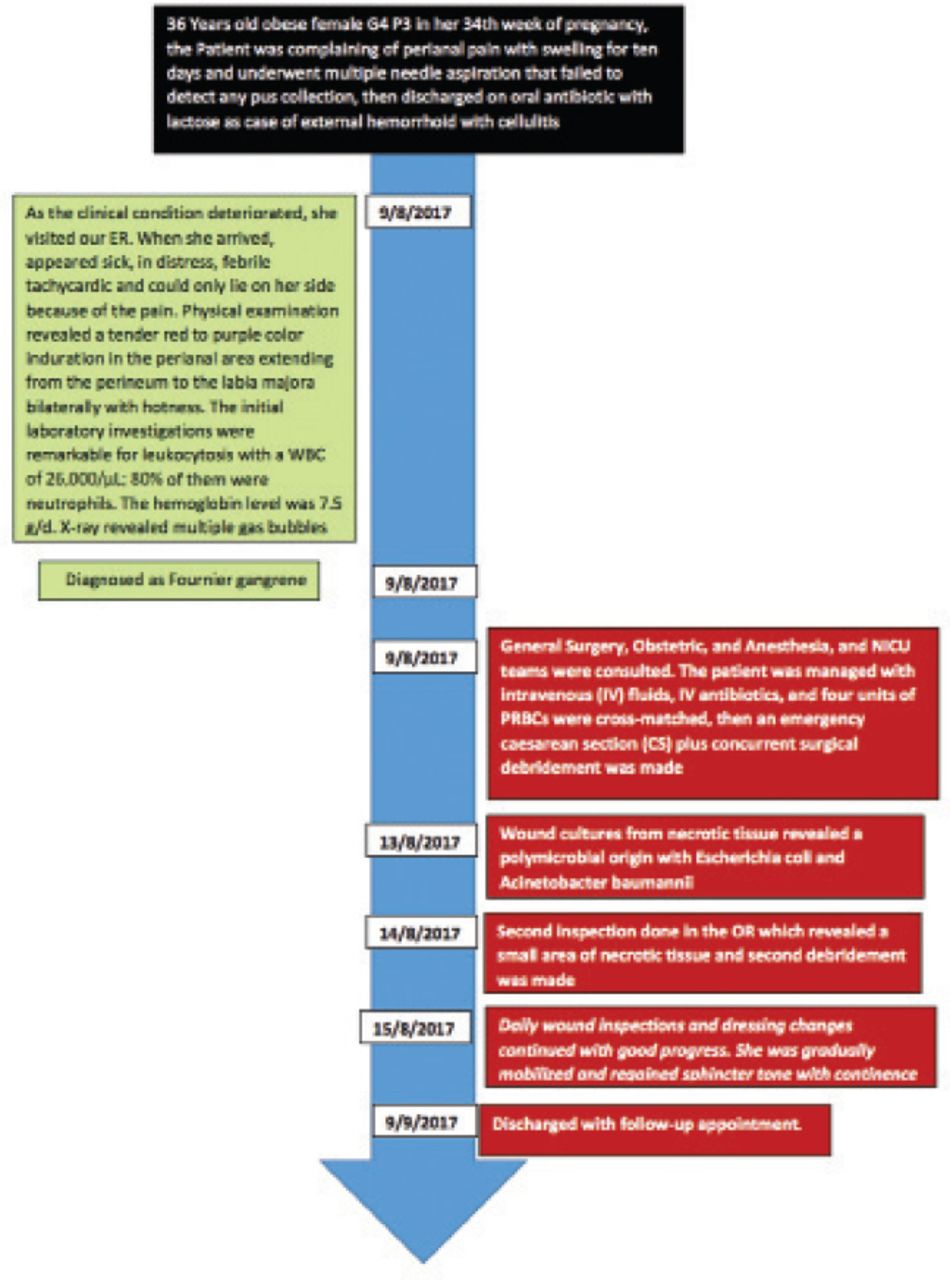
Timeline summarizing the case presentation and the sequence of interventions.
Clinical finding
As the patient’s clinical condition deteriorated, she visited our ER. When she arrived, she appeared sick, in distress, and could only lie on her side because of the pain with difficultly in mobilizing herself. Her vital signs were a temperature of 39.5°C, a heart rate of 139 beats per minute, blood pressure 120/66 mm Hg, respiratory rate 24 per minute, oxygen saturation 97% and random glucose 108 mg/dl. Weight: 91 kg, height: 160 cm, body mass index (BMI): 35.5 The physical examination revealed foul odor edematous perianal skin with red to purple color induration in the perianal area extending from the perineum to the labia majora bilaterally with severe tenderness and hotness but no crepitations or hemorrhagic bullae noted.
Diagnostic assessment
The initial laboratory investigations were remarkable for a hemoglobin of 7.5 gm/dL and white blood cell of 26,000/cmm with 80% neutrophils. Because of the pain and clinical condition, she could not lie in a supine position for the CT scan, so a lateral pelvic x-ray was carried out which revealed multiple gas bubbles in the perianal soft tissues (Figure 2) and therefore a preoperative diagnosis of Fournier’s gangrene was made.

Lateral view of pelvic x-ray showing the increased soft-tissue opacity with a variant size of subcutaneous gas bubbles.
Therapeutic interventions
In the ER, she was managed with intravenous (IV) fluids, 1 g IV ceftriaxone, 1g IV vancomycin, 500mg IV metronidazole, and 4 units of PRBCs were cross matched. General surgery, obstetric, anesthesia, and NICU teams were consulted for multi-aspect evaluation and shearing the decision regarding the emergency cesarean (CS) section with concurrent surgical debridement and subsequently this what was decided and planned. In the operation room (OR) under general anesthesia a lower segment CS was carried out via a Pfannenstiel incision without complications. The surgical team then took over, and a long incision was placed from the perianal area at 4 o’clock up to the left labium marjoram. A significant amount of brown-grayish foul smelling purulent collection was drained. A large abscess cavity was revealed with extensive areas of necrotic tissue at the base. This partially involved the anal sphincter and reached the left lateral wall of the rectum, which luckily had been spared of necrosis. This also revealed a diffuse area of necrotic tissue extending from the upper buttock bilaterally to the perianal area, ischiorectal fossa, perineum, and labia majora. Wide debridement was carried out sparing the anal sphincter.
Follow-up and outcomes
Postoperatively she was transferred to a surgical ward bed and received broad-spectrum antibiotics coverage (4.5 g IV Piperacillin/tazobactam every 8 hours and 1g vancomycine every 12 hours), IV fluids, analgesics, and daily dressing changes. Wound cultures from necrotic tissue revealed a polymicrobial origin with Escherichia coli and Acinetobacter baumannii. She complained of anal pain with partial stool incontinence and weak anal tone, and a second inspection carried out in the OR day 5 postoperatively. This revealed a small area of necrotic tissue and second debridement was made. Daily wound inspections continued with good progress without fistula formation. Moist saline dressing were changed daily for the first 3 weeks, after which they were gradually spaced as the healing progress. She was gradually mobilized and regained good sphincter tone with continence, and eventually discharged after 31 days of hospital admission with follow-up appointment at an outpatient clinic.
A female baby born in 34th week and had an Apgar score of 6 at 1 minute and 9 at 5 minutes with a weight of 1.75 kg. This preterm baby developed respiratory distress and was connected to a non-invasive continuous positive airway pressure (CPAP) ventilation machine from which she was successfully weaned after 3 days. After that, she remained in stable condition and was united with her mother on discharge
Discussion
Fournier’s gangrene is an acute and rapidly progressive necrotizing fasciitis of the genitalia that may spread to the thighs or abdomen. It is typically a polymicrobial infectious origin from the genitourinary and anorectal tract or the skin of the genital area that acts synergistically with vascular necrosis leading to localized ischemia and further bacterial proliferation.5 Risk factors include diabetes mellitus, alcohol abuse, hypertension, renal and hepatic failure, obesity, smoking, immunodeficiency diseases, and preexisting injury.6 Finding a woman in the third trimester of pregnancy with Fournier’s gangrene is extremely rare. As we did an extensive search looking for cases of “fournier gangrene, pregnancy” from 1950 to the present-day in PubMed, Cochrane, Elsevier, Lancet, Centers for Disease Control and Prevention, and Google Scholar, but found only a single Case Report.7 Despite some similarity between this case and this prior case, this case is unique in that the patient underwent emergency CS with radical surgical debridement during the same operation sitting.
The development of Fournier gangrene in this young woman without significant previous history might be attributed to her pregnancy in different aspects. The pregnancy could alter immunity, and the weight of the uterus places physical stress on the rectum and vagina beside the hormonal changes on the pelvic floor.8 However, regardless of the pregnancy condition, our patient was obese with pre-pregnancy BMI of 32 and her BMI upon arrival was 35.5 that is considered a contributing factor to the development of Fournier gangrene.6 Another possibility can be a perianal abscess evolving in Fournier gangrene by the multiple needle aspiration attempts, which can be avoided by using ultrasound instead of blind needle exploration of the perianal area.
The diagnosis of Fournier gangrene is not clinically straightforward nor timely. As in this case, not all Fournier gangrene cases have the classical finding of hemorrhagic bullae or crepitation, which only present in 20-50% of the cases.9,10 In addition to that, the obesity with the severe tenderness in the edematous perianal area may mask such subtle findings. This reemphasizes the importance of maintaining high index of suspicion and requesting radiological imaging in low-probability cases to confirm the diagnosis and determine the extent of gangrene or abscess.
Diverting colostomy remains a difficult controversial option in Fournier gangrene with perineal involvement. It was believed to play a role in preventing fecal contamination and improved wound healing, but associated higher mortality.11 In this case, considering colostomy may negatively affect the nearby SC wound, and furthermore because of the critical condition of the patient, it was deferred to be carried out along with the second intraoperative debridement if needed. However, the subsequent condition of the wound was remarkably improved with the vigilant care of the perineal wound, and therefore the colostomy was avoided.
It is important to conclude that the keys for a successful outcome in such a complicated presentation of Fournier gangrene include early diagnosis, fluid resuscitation, rapid administration of broad-spectrum antibiotics, and early interdisciplinary approach by multiple teams for sharing decisions, and balancing the risk benefit of emergent-CS without delaying the surgical debridement.
Acknowledgment
This work was supported by the College of Prince Sultan Bin Abdulaziz for Emergency Medical Services, Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia. We would like to express our appreciation to the Deanship of Scientific Research at King Saud University. Furthermore, we would like to thank all the healthcare providers participated in this case at Al-Iman General Hospital, Riyadh, Saudi Arabia
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 3, 2017.
- Accepted February 21, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.