


Abstract
Heterotopic pancreas is defined as aberrantly located pancreatic tissue without anatomical, vascular, or neural connection to the pancreas. Usual sites include the stomach, duodenum, jejunum, and spleen; in rare cases, heterotopic pancreas can be found in the lungs, gallbladder, Meckel’s diverticulum, and the mediastinum. In most cases, it is an insignificant, incidental finding. Pre-operative diagnosis is not possible, and histopathological examination is mandatory for establishing a definite diagnosis. Less than 40 cases of heterotopic pancreas in the gallbladder have been reported worldwide. Recently, a laparoscopic cholecystectomy specimen from a 43-year-old male showed a small nodule in the gallbladder neck. Microscopy revealed heterotopic pancreas composed of exocrine and endocrine glandular tissue with ducts. We report this case to highlight this rare, incidental finding. This condition should not cause pathologists to over diagnose such occurrences as malignancies; neither should they be neglected because they have potential complications.
Choristoma in the form of ectopic or heterotopic pancreas is an embryological abnormality and is defined as aberrantly located pancreatic tissue without anatomical, vascular, or neural connection to the pancreas.1,2 The sites usually involved include the stomach, duodenum, jejunum, and spleen; however, heterotopic pancreas is rarely encountered at other sites including the ileum, mesentery, lungs, gallbladder, liver, bile ducts, Meckel’s diverticulum and the mediastinum.3,4 In most cases, the condition is an incidental finding during autopsy or laparotomy for unrelated reasons. However, heterotopic pancreas has the potential to lead all the metaplastic and neoplastic conditions that affect orthotropic pancreas.4 Pre-operative diagnosis is not possible, and histopathological examination is mandatory for establishing a definite diagnosis.1,2 The incidence of heterotopic pancreas at all sites ranges from 0.55%-13.7% in autopsies and 0.2% in laparotomies.1,5,6 A number of cases have been reported in which heterotopic pancreatic tissue was incidentally found during microscopic examination of gallbladders after cholecystectomies for polyps, nodules, and acute or chronic cholecystitis with or without gallstones.1,2,3,5,6 The clinical significance of such incidental findings is still unclear.2,5 Here, we present a case study of heterotopic pancreatic tissue in the gallbladder to familiarize pathologists with the condition and to stress that it should be considered in differential diagnosis of polyps, nodules and acalculous cholecystitis. Moreover, the microscopic appearance should not lead to over diagnosis of malignancy, nor should one overlook the condition as an insignificant incidental finding, considering its potential for sinister pathologies.
Case Report
Patient’s information
A 43-year-old male presented to the Department of General Surgery, King Abdullah Hospital, Bisha, Saudi Arabia.
Clinical findings
Our patient presented with history of mild yellowish discoloration of the sclera and skin and fatty dyspepsia that was aggravated after meals. On physical examination tenderness was noted in the right upper abdomen; however, associated guarding or rebound tenderness was not present, no other significant past medical or surgical history was present.
Diagnostic assessment
Laboratory results showed alkaline phosphatase, 102 U/L (40-129 U/L); gamma glutamyl transferase, 75 U/L (8-61 U/L); total bilirubin, 22.9 µmol/L (0-18.1 µmol/L); and conjugated bilirubin, 9 µmol/L (0-7 µmol/L) in patient’s serum. These findings were consistent with clinical picture of obstructive jaundice. Serum amylase level was 96 U/L (normal range: 28-100 U/L). Serum lipase was 139 U/L (normal range: 13-60 U/L). Abdominal ultrasound revealed multiple tiny stones, biliary sludge in the lumen of the gallbladder, and minimal wall edema. On magnetic resonance cholangiopancreatography (MRCP) multiple small gallbladder stones with a normal biliary tree were reported. A preoperative diagnosis of chronic cholecystitis with obstructive jaundice was made.
Therapeutic intervention
The pain and jaundice responded to conservative medical therapy, however laparoscopic cholecystectomy was carried out to prevent further episodes.
Histopathology and diagnosis
Macroscopic examination revealed a gallbladder measuring 75 mm into 25 mm. The average wall thickness was 3 mm. The mucosa showed focal ulceration and a single solid, whitish, intramural nodule measuring 6 mm in the neck region. Thick biliary sludge and multiple small stones were present in the lumen. Multiple representative sections were submitted for analysis.
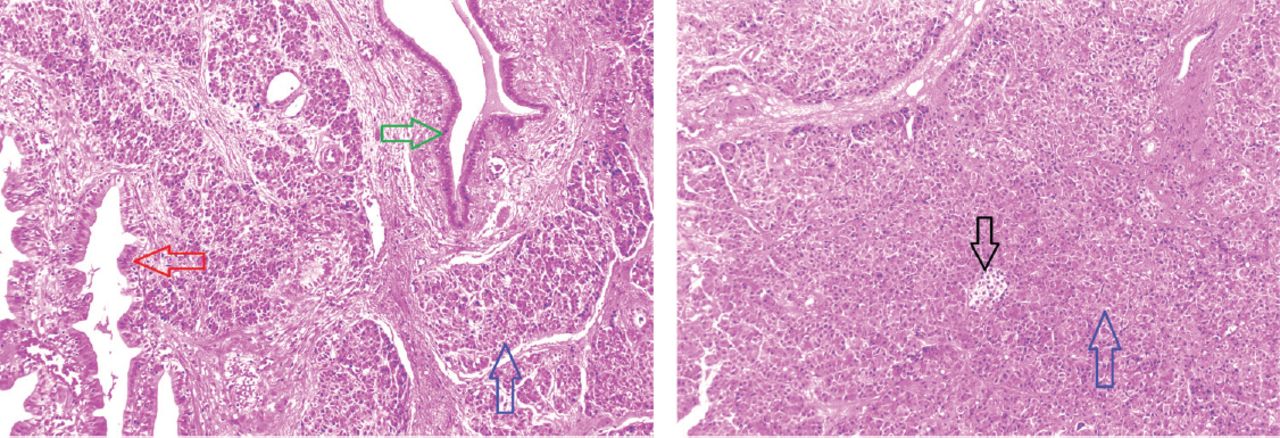
Microscopic examination of the sections from the gallbladder neck revealed a well-circumscribed, intramural nodule of aberrant pancreatic tissue. Both exocrine and endocrine pancreatic tissues were present, consisting of acini and ducts along with a few islets of Langerhans (Figure 1). Our case was classified as type I according to the von Heinrich classification of pancreatic heterotopia. The remainder of the section showed chronic inflammatory reaction with epithelial changes consistent with chronic cholecystitis. No evidence of dysplasia or malignancy was found in any of the sections examined.
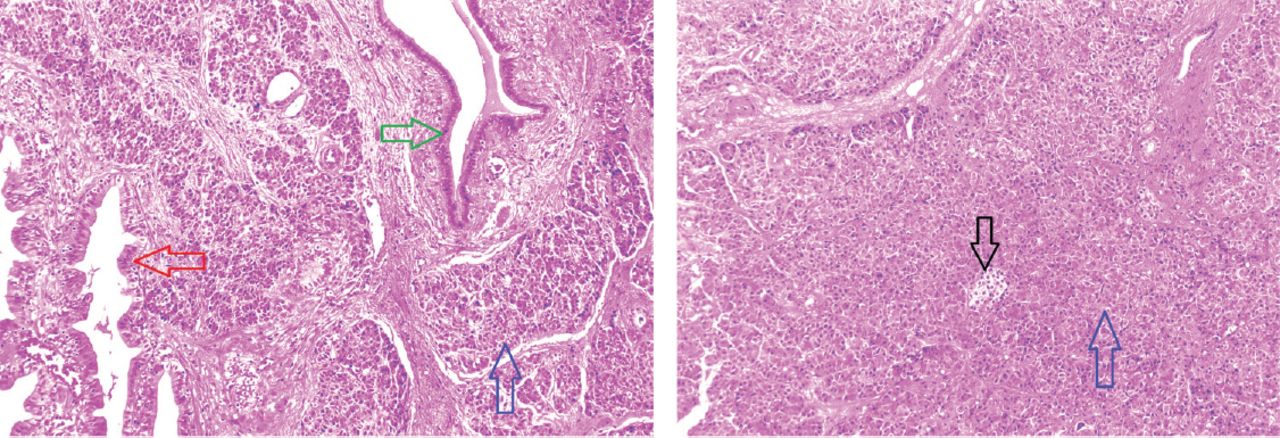
Heterotropic pancreas in gallbladder (hematoxylin and eosin stain, 10X) showing: surface epothelium of gallbladder (red arrow), pancreatic acini (blue arrow), pancreatic duct (green arrow), and islet of langerhans (black arrow).
Follow-up
A smooth, uneventful recovery followed the surgery, and none of the symptoms persisted. No complication has been reported so far.
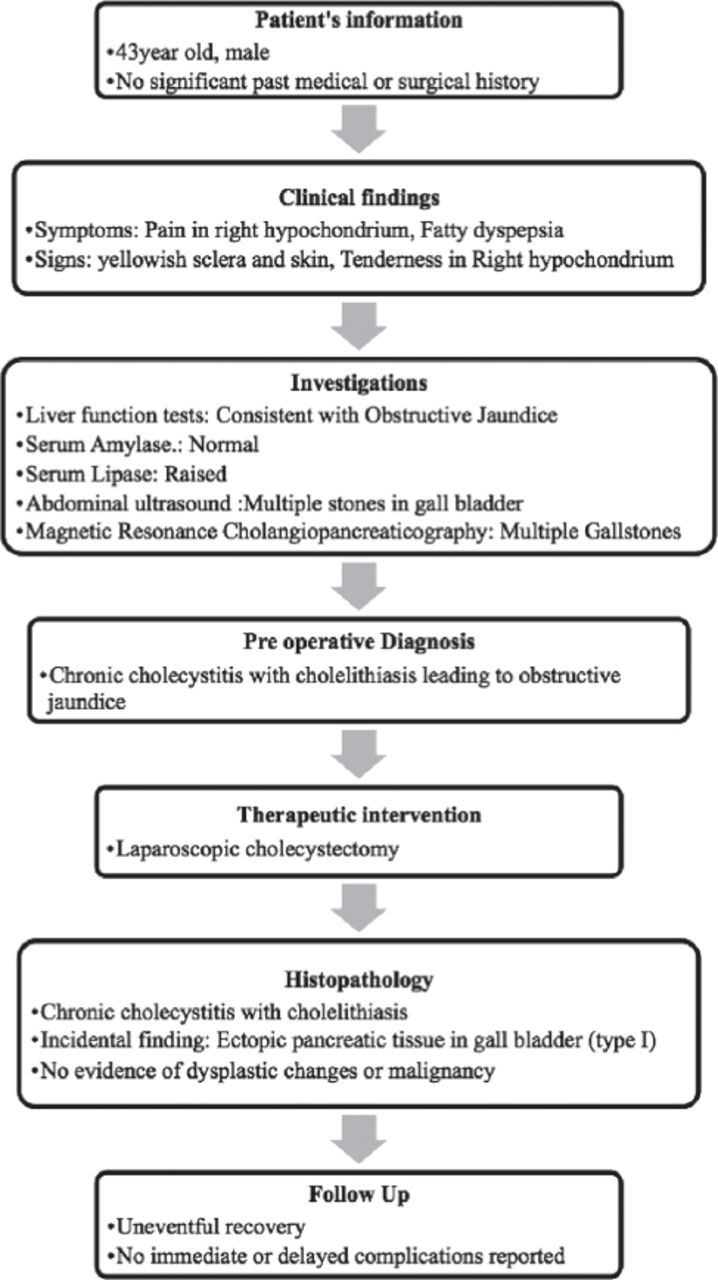
(Figure 2) represents the timeline from patient’s presentation to final outcome.

Timeline summarizing the patient’s information, clinical findings, investigations, preoperative diagnosis, therapeutic intervention, histopathology, and follow up.
Discussion
Pancreatic heterotopia is a rare anomaly that is mostly found in the stomach and duodenum.1-3 The gallbladder is an extremely rare location for heterotopic pancreas.1-3,5,7 The first reported case of heterotopic pancreas in the gallbladder dates back to 1916 in a description by Otschkin.2 So, far less than 40 cases of such occurrence have been reported.7 It is usually an incidental finding during autopsies or laparotomies due to unrelated reasons. The overall incidence ranges from 0.55%-13.7% in autopsies and 0.2% in laparotomies.1,5
Different theories have been proposed for the origin of this aberrant tissue at unusual sites. The most widely accepted hypothesis is that the tissue becomes separated from the developing pancreas during rotation of the gastrointestinal tract during the embryonic period.2,3
Macroscopically, these lesions can present as thickenings, nodule forms, or as a polyp. The tissue is located in the neck region of the gallbladder in half the patients, as in our case.2,5 Histologically, exocrine and endocrine tissues can be present in various proportions. Von Heinrich classified pancreatic heterotopia into 3 groups in 1909.2 later this classification was modified by Fuentes in 1973 (Table 1).5,7 Accordingly, our case was classified as Type I.
Pancreatic heterotopia can occur at any age, but it is most often found in the 4th-6th decade of life.1 Overall, men are affected 3-5 times more frequently than women.2 However, when the site of ectopic pancreatic rests is the gallbladder, the patient is usually a female.1,2 This is probably due to the greater number of cholelithiaisis-related cholecystectomies in female patients. Our patient was a male in his 5th decade.
The majority of cases are asymptomatic, and histologically discovered tissue is usually benign. However, heterotopic tissue can cause symptoms related to its location; such symptoms include jaundice due to obstruction of the bile duct, cholelithiasis, cholecystitis, intussusception and gastrointestinal hemorrhage.3,4 Although ectopic pancreas is usually found incidentally, it nonetheless has the potential to develop all of the metaplastic and neoplastic changes that occur in normally located pancreas, including acute or chronic pancreatitis, cyst formation, calcification, pancreatic cancers, and endocrine tumors.1,3,4 Therefore, complete excision of incidentally found pancreatic tissue is the treatment of choice. In cases of heterotopic pancreatic rests in the gallbladder, cholecystectomy is adequate.2,3 As there are only a few such reported cases, the clinical and radiological features are not well defined.6 Preoperative diagnosis of this rare finding is not possible due to nonspecific features, and definitive diagnosis is only possible by histopathological examination.1,5
In conclusion, pancreatic heterotopia is a rare entity, when it is located in the gallbladder wall. Pathologists should be familiar with this rare, incidental finding, as it can mimic a tumor and lead to over diagnosis of malignancy. However, a careful examination is needed to rule out potential complications and related sinister pathologies.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 3, 2018.
- Accepted June 14, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.