


Abstract
Breast surgery operations are generally performed by general anesthesia. In order to decrease postoperative pain, regional anesthesia is usually combined with general anesthesia. Pectoral nerve blocks is a novel technique to provide perioperative and postoperative pain control for patients underwent breast surgery. We performed pectoral nerve block I and pectoral nerve block II as a sole anesthetic technique with sedation by dexmedetomidine for modified radical mastectomy, for a 75-year-old female patient with multiple diseases. Pectoral nerve blocks with sedation could be a good technique for breast surgery than general anesthesia in comorbid patients.
An increase in the world’s population has led to a rise in the incidence of breast cancer, the most common type of cancer in women. Furthermore, improvements in the health care system have increased the number of elderly patients who often suffer with comorbid diseases. These factors are a challenge for anesthetist’s to be able to perform safe anesthesia and provide good postoperative pain control. General anesthesia (GA) is frequently associated with postoperative vomiting and nausea, which may occur in up to 50% of cases. Regional or local anesthesia is an alternative to GA and results in fewer postoperative complications, a shorter hospital stay, and better perioperative pain control.1 Regional anesthesia (RA) techniques have less intraoperative, respiratory, and postoperative complications than GA.2 In breast cancer surgery operations, pectoral nerve blocks (PECs) I and II have been performed in combination with GA to reduce perioperative and postoperative pain.3 An ultrasound guiding PECs blocks is straightforward and provides analgesia for the chest wall. In this case, we administered PECs I and PECs II block on a 75-year-old patient who underwent a modified radical mastectomy, as the sole anesthesia technique to prevent complications related to GA.
Case Report
A 75-year-old female (height 160 cm, weight 102 kg and American Society of Anesthesiologists [ASA] was III) diagnosed with invasive ductal carcinoma was due to undergo a right side modified radical mastectomy with axillary lymph node dissection at the Hacettepe University Medical Faculty Hospital, Ankara, Turkey. She had type II diabetes mellitus, hypertension, atrial fibrillation, coronary artery disease, congestive heart failure with an ejection fraction (EF) of 40%, and moderate chronic obstructive pulmonary disease. She also had a cardiac resynchronization therapy defibrillator (CRT-D) device implanted when she was 66 years old.
Clinical findings
Monitoring with pulse oximetry, electrocardiography, and non-invasive blood pressure tests revealed that she had a baseline heart rate of 96 beats/min, blood pressure of 140/85 mmHg, and an oxygen saturation of 89% upon arrival to the operating theatre (Table 1).
Timeline of medical history, vital signs, evaluations and interventions.
As she had various comorbidities, we were reluctant to administer GA and decided to instead administer PECs I and II blocks combined with sedation.
Diagnostic assessment
In this case; to identify the muscle groups, ribs, and to visualize the needle placement and the local anesthetic spread an ultrasound has been used.
Therapeutic intervention
Supplemental oxygen was administered by nasal oxygen at 4 l/min following a premedication of 1.5 mg of intravenous midazolam was given. We subsequently induced a loading dose of dexmedetomidine (1µg/kg over 10 minutes), followed by 0.2 µg/kg/hour as a maintenance dose for sedation.
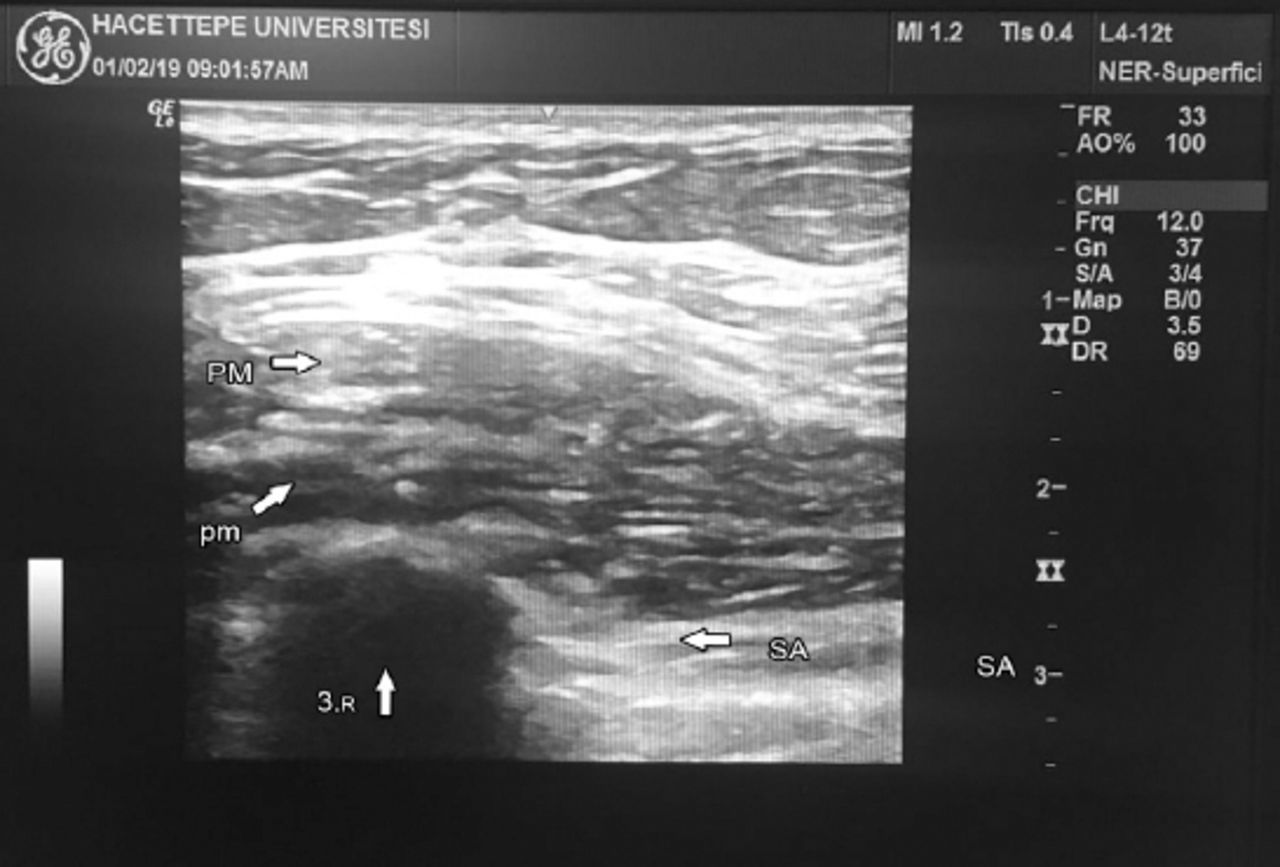
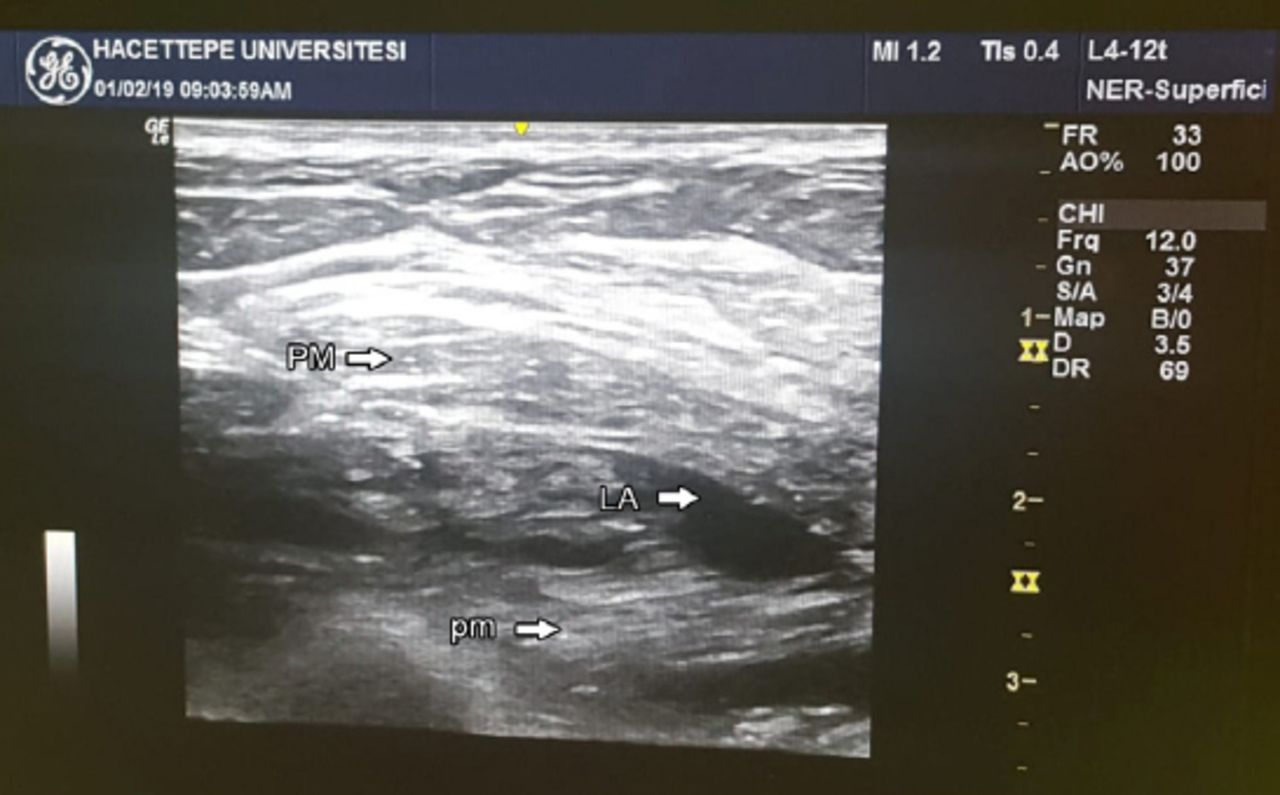
When a score of 5 had been achieved on the Ramsey sedation scale, the right chest wall and the right axillary region were cleaned using iodine. A high frequency (4-12 MHz) linear probe (GE Healthcare, USA) was placed inferior to the right clavicle to identify the pectoral muscles with axillary vessels; the probe was moved caudally to identify the 3rd and 4th ribs and after the oblique rotation of the probe, the skin was infiltrated with 2% prilocaine (Figure 1). Initially, the PECs II block was performed using a 10 mm 22G regional block (UniPlex, PAJUNK, Germany) needle, which was inserted using the in-plane technique into the tissue between the serratus anterior muscle and the pectoralis minor muscle. A total of 20 ml of a local anesthetic agent (bupivacaine 0.5%) was injected (Figure 2). To administer the PECs I block, the needle was withdrawn and subsequently inserted between the pectoralis major and minor muscles, and 10 ml of the local anesthetic (bupivacaine 0.5%) was injected between these 2 muscles (Figure 3). The whole procedure took approximately 10 minutes. Twenty minutes after performing the block, a cold test was used to evaluate the effectiveness of the sensory block. Surgery proceeded after a further 10 minutes. She was draped in the standard sterile manner. An elliptical incision was made, and the flaps were dissected laterally from the latissimus muscle superiorly to the clavicle. The breast was dissected from the pectoralis major muscle. The interpectoral lymph nodes and fat were removed along with the specimen.

The ultrasound vision of pectoral major, pectoral minor and serraus anterior muscles. PM - pectoral major muscle, pm - pectoral minor muscle, 3.R - the third rib, SA - serraus anterior muscle

PECs II block: The distribution of local anesthesia between pectoral minor and serratus anterior muscles. PECs II - pectoral nerve blocks II, PM - pectoral major muscle, pm - pectoral minor muscle, 3.R - the third rib, LA - local anesthesia, SA - serraus anterior muscle

PECs I block : The distribution of local anesthesia between pectoral major and pectoralis minor muscles. PECs I - pectoral nerve blocks I, PM - pectoral major muscle, pm - pectoral minor muscle, LA - local anesthesia
Following the axillary dissection, the en bloc resection technique was applied to remove the axillary lymph nodes and adipose tissue. The long thoracic and thoracodorsal nerves were identified and were carefully preserved. While the 2 surgical drains were being placed, she felt pain, and an additional 100 mg of prilocaine was administered to the site where the drains were located. The whole operating time was 110 minutes and 34 x 32 x 6 cm (2830 g) of breast tissue was excised. She was hemodynamically stable throughout the surgery.
Follow-up and outcomes
During the postoperative period, the vital signs were stable; there was no postoperative nausea and vomiting (PONV) with no additional need for analgesics. The visual analogue score (VAS) was 2. Analgesia was required for the first time 6 hours after the surgery had begun. She was discharged after 5 days without complications.
Discussion
Pectoral nerve blocks are a well known technique, similar to thoracic paravertebral and thoracic epidural blocks, that provide analgesia for patients undergoing breast cancer surgery.3 The thoracic paravertebral block is still recognized as the gold standard analgesic procedure for breast surgery. However, there can be consequential complications such as unintentional vascular injection, hypotension, intrathecal spread, epidural hematoma and nerve damage, which makes this procedure unsuitable for ambulatory breast surgery.3,4 Compared to other regional anesthetic techniques, the PECs blocks can be performed in the supine position, away from vital organs such as the spinal cord and pleura. If the patient is under GA, these blocks are easy, comfortable, and less complicated.
The medial and lateral branches of pectoral nerves are anesthetizes by PECs I block that innervate these 2 muscles. The PECs I technique provides analgesia to pectoral muscles and is mainly used in breast expander and subpectoral breast prostheses operations. The PECs II block anesthetizes the thoracodorsal and long thoracic nerve, as well as the lateral branches of the intercostal nerves from T2-T6.5 In addition to the region under the pectoralis minor muscle, PECs II also provides analgesia to mammary glands and the skin from the T2-T6 dermatomes extending into the mid-axillary line by blocking the lateral intercostal nerves.4
Under extreme circumstances, a PECs block can be performed to provide postoperative analgesia under GA. In a recent study, GA without a PECs block and GA with a PECs block was compared.6 They found that the patients with a PECs block had less nausea, vomiting, and pain. Fewer patients have had PECs blocks as the sole anesthetic technique. Moon et al,4 reported on a successful breast surgery performed under PECs I and II blocks when a patient refused GA. Hong et al,7 reported on a pregnant women who refused GA for breast surgery.
Campos et al,8 reported that a patient with several comorbidities and a high surgical risk, underwent a PECs II block as the exclusive anesthetic technique, similar to our patient. In the absence of visceral pain throughout the thoracic wall surgery, this block may be an effective and adequate option instead of GA. Our patient had an excellent anesthesia period; we only used local anesthesia for drain incision at the end of the procedure.
The main reason for selecting dexmedetomidine for sedation is that dexmedetomidine provides sedation without respiratory depression. However, bradycardia and hypotension are common side effects of dexmedetomidine. During the procedure, the patient was hemodynamically stable without any bradycardia or hypotension. We started the induction of dexmedetomidine with a loading dose (1 µg/kg over 10 minutes), followed by 0.2 µg/kg/hour as a maintenance dose to maintain sedation without delayed recovery.
The potential benefits of RA and analgesia on long-term oncological outcomes are exciting. Regional anesthesia may reduce cancer progression by attenuating the surgical stress response, producing better analgesia, reducing opioid usage, and inhibiting cell migration.9 We need to have more robust and well conducted prospective randomized trials for studying the impact of RA on cancer recurrence and metastases in breast cancer surgeries.9
If adequate analgesia can be provided during breast surgery by RA, the occurrence of persistent breast cancer pain syndrome and phantom breast pain could be reduced. A meta-analysis and Cochrane review on persistent pain following breast surgery revealed that pre-operative regional blocks were effective at reducing subsequent chronic pain.10
Furthermore, high-quality studies are warranted to assess the impact of RA and analgesia on breast cancer surgery, not only on post-operative pain as the primary outcome, but also on other important outcomes such as chronic pain, phantom breast pain, nausea, and vomiting; this would potentially help in formulating plans for perioperative care of patients undergoing breast cancer surgeries. Ongoing randomized controlled trials to determine the impact of RA on oncological outcomes will provide definitive guidance in the future.
In conclusion, the use of a PECs block as the sole anesthetic in patients with multiple comorbidities may provide better analgesia, lesser side effects, reduced hemodynamic instability, and would be a safer option when compared to GA.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
Disclosure. The manuscript was presented as an oral presentation in the 16th Natıonal Regıonal Anesthesıa Congress (Radkon 2019) in Izmir, Turkey, on 29 April 2019. The abstract was published in Radkon 2019 Book of abstract of the conference page 98.
http://www.rad.org.tr/wpcontent/uploads/2019/05/Radkon2019-Bildiri-Kitab%C4%B1.pdf
- Received September 11, 2019.
- Accepted October 13, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.