


Abstract
Objectives: To determine if there is a relationship between acute stress and either the onset or relapse of multiple sclerosis (MS) and to discover how different types of acute stressors may be involved.
Methods: This study was carried out in Saudi Arabia between September 2017 and June 2018 and involved King Fahad University Hospital in Eastern province, Arfa Multiple Sclerosis Society in the Central and Western province of Saudi Arabia. A cross-sectional descriptive study was performed using an Arabic self-constructed questionnaire consisted of 4 sections: 1) demographic data and time of diagnosis; 2) emotional/psychological stressors; 3) environmental/physical stressors; and 4) 4 specific stressors measuring their effect on the severity and recurrence of attacks.
Results: A total of 370 patients participated in the study. Almost half of patients reported no effect of family problems on their disease, whereas the other reported that family problems have an impact on the onset or relapse of the disease. Majority of patients reported that work and social life stressors affect the recurrence of attacks. Cold weather showed no effect on MS; however, hot weather and physical activity increased the number of attacks. Continuous thinking about social stress and problems, mood swings, and sleep deprivation showed an impact on the severity and recurrence of attacks. Financial problems showed no effect.
Conclusion: Study indicates that an association exists between acute stress and relapse in MS but not the disease onset.
Multiple sclerosis (MS) is a chronic, progressive, auto-immune disease that affects the central nervous system (CNS) with an unknown exact cause. It is one of the most common demyelinating diseases and the most common cause of disability in young adults.1 Clinical manifestations differ from one person to the other with complexity and variability of the symptoms. The prevalence of MS is high in North America and Europe (>100/100,000 population) compared to the prevalence in the Arabian Gulf Region (31-55/per 100,000 population) and Saudi Arabia (25/100,000 population) with an increase in the incidence in the last few years.2 Several factors can play a role in the pathogenesis of MS disease such as infection with Epstein--Barr virus (EBV), smoking, vitamin D deficiency, and a high salt diet, whereas stress and traumatic events have not been identified as risk factors for the disease onset or exacerbations. However, one study showed managing emotional stress reduced the development of new brain lesions in a sample of MS patients.3 Stress affects the corticotrophin-releasing hormone (CRH) that acts on the adrenal glands to produce cortisol. Too much cortisol decreases immunity, but the exact mechanism and effect of stress on autoimmune diseases is unclear. Stress can be emotional, physical, or environmental, and based on its duration it can be acute or chronic. Acute stress is a short-term type of stress resulting from specific events or situations that have a major impact on the person, whereas chronic stress is a long-term type of stress resulting from repeated exposure that ends up usually with adaption.4 Studies have shown that disease-related chronic stressors do not increase the possibility of attacks in MS patients compared to acute stressors, which can create more pressure and have a greater impact.5 We aimed in this research to study the association between different types of acute stress and the onset of MS disease, as well as the effect of acute stress on relapses in a sample of MS patients in Saudi Arabia. This study is considered to be one of the few studies in the Arabian Gulf countries and worldwide that can help us to identify if an association exists, which might be useful in treating and managing MS patients in the future.
The aim of this study was to determine if there is a relationship between acute stress and either the onset or relapse of MS. The study also sought to discover how different types of acute stressors may be involved.
Methods
This study was carried out in Saudi Arabia in September 2017 and was approved by the Institutional Review Board (IRB) which follow the principles of Helsinki Declaration in Imam Abdulrahman bin Faisal University (IAFU), Al Khobar, Saudi Arabia. Study participants were patients from the outpatient neurology clinic and diagnosed with MS based on 2010 McDonald criteria.6 The sample size was 370 patients calculated based on the prevalence and the confidence interval of 95% and collected randomly. Their age was between 15 to 50 years old, all met the inclusion criteria no patients were excluded. Approximately 100-150 patients were selected from the 3 biggest regions in Saudi Arabia: King Fahd University Hospital (KFHU) in the Eastern province and Arfa Multiple Sclerosis Society in the Central and Western province.
This cross-sectional descriptive observational study was carried out using an Arabic self-constructed questionnaire. Initially, a pilot study was carried out with a small sample to test and measure the strength of the questionnaire. Cronbach’s alpha values were used to determine the internal reliability of the instrument, the reliability of the measure was 0.73 that is significant.
Inclusion criteria were diagnosis of MS based on 2010 McDonald criteria with unspecified type of MS; age not less than 15 and not more than 50; all MS patients who are diagnosed and treated in Saudi Arabia regardless of their nationality. Exclusion criteria were not meeting the criteria for MS; any patient less than 15 years old or above 50 years old and patients who are not treated in any center in Saudi Arabia.
In order for a patient to be defined as having an MS relapse, he/she had to meet the following criteria: focal neurological disturbance affecting white matter tracts lasting more than 24 hours; 30 days of clinical stability prior to the onset of the neurological disturbance; absence of fever and/or infection and no alternative explanation for the patient’s symptoms.
The questionnaire was administered to patients in an interview style after obtaining verbal informed consent. All the information was kept confidential. The questionnaire consists of 4 main sections each related to the research objectives. The first section consists of questions concerning demographic characteristics (age, gender, marital status, academic level, and career) and time of diagnosis. The second section consists of questions about emotional/psychological stressors such as family problems or death of relatives, workload, and social life events. The third section consists of questions about environmental/physical stressors such as hot/cold weather and physical activity. For the second and third sections there are 4 response options: effect on the onset of MS, effect on the recurrence of attacks, effect on both recurrence and onset, and no effect at all. The fourth section consists of 4 specific stressors measuring the effect on disease severity and its recurrence, which are financial problems, sleep deprivation, mood swings, and over thinking; all having the yes/no response option. All the answers were subjective.
Statistical analysis
The data was collected and analyzed by using the Statistical Package for Social Sciences (SPSS) version 23 (Armonk, NY: IBM Corp.). Descriptive analysis of the sociodemographic characteristics of the participants are presented in a table. Data were analyzed descriptively using simple statistical ratios consisting of means, standard deviations, directions based on Likert-scale, counts, and percentages. Multinomial logistic model, binary logistic model, Spearman’s rank, and coefficient correlation were used to test the statistical correlation between questions. A p-value below 0.05 was considered statistically significant. Table 1 presents values for the 4-point and 2-point Likert-scale for the questions in sections 2 & 3 and questions in section 4, respectively.
Values based on 4-point and 2-point Likert scale.
Results
Section 1
A total of 370 out of 400 MS patients responded where 30 patients refused to participate. One hundred and forty-eight from western province, 120 from eastern province, and 102 from the central region. The response rate was 92.5%. Saudi MS patients were accounted for 93% of the sample. Two hundred and forty-nine participants were female (67.3%) and 121 (32.7%) were male with a female to male ratio of 2:1. The majority (75.4%) of patients were from 21 to 40 years of age and 55.9% of the patients were married. Near half of the patients (53.2%) completed higher education (bachelor’s degree) and only 0.5% were uneducated. Regarding employment, 306 patients were employed in different sectors, whereas only 64 were unemployed (Table 2). The majority (36.8%) of patients were diagnosed within 5-10 years of symptoms onset, and the remaining (34.6%) were diagnosed earlier (<5 years); and only 28.6% were diagnosed >10 years.
Demographic data of 370 Multiple sclerosis (MS) patients.
Sections 2 and 3
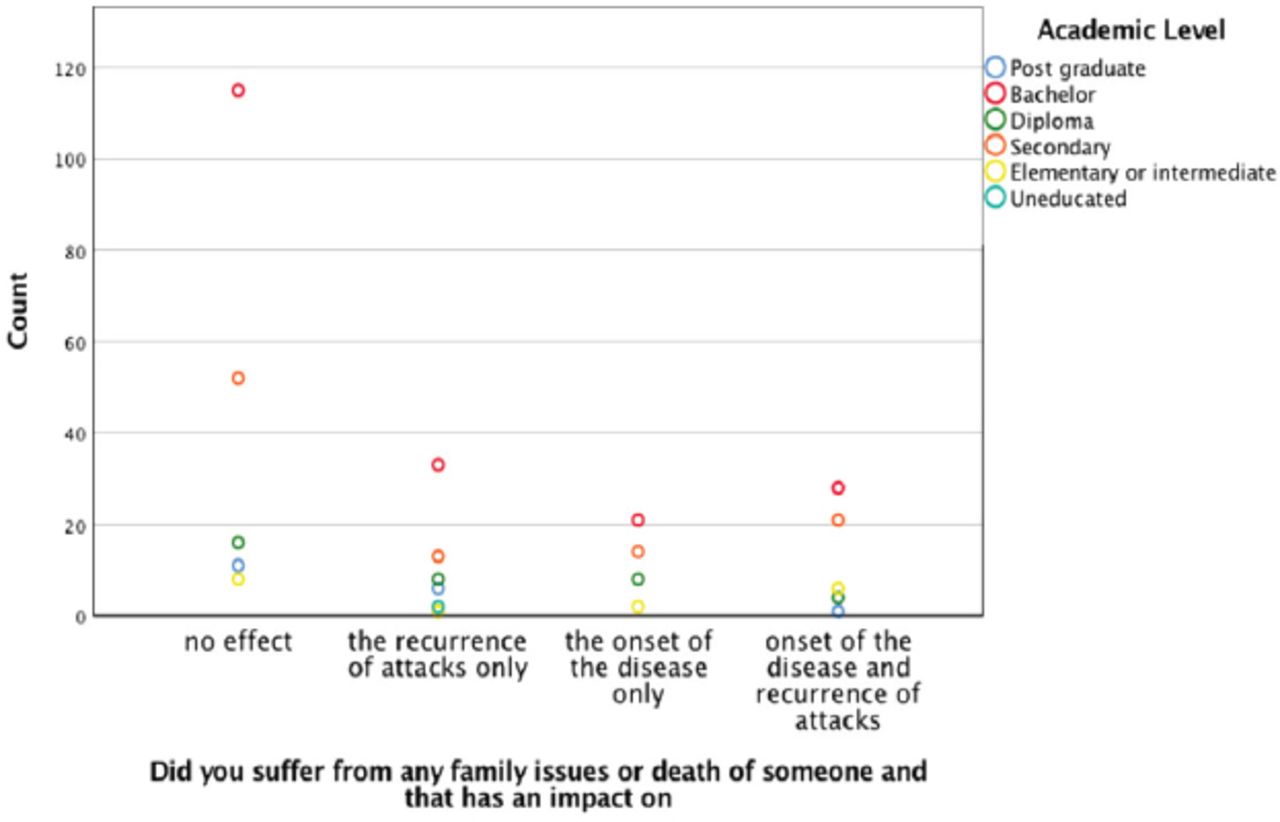
Based on the Likert-scale, suffering from family problems or death of relatives showed a direction with the recurrence of attacks only (mean±SD: 0.9±1.144). Slightly more than half of the patients (54.6%) reported family problems or death of relatives had no effect on their illness, whereas 45.4% reported these factors had an effect either on the onset of the disease, relapse, or both. Most of those patients were diagnosed between 5 to 10 years of symptom onset; the correlation was statically significant between the family issues and the onset of disease (p=0.003). Most also correlated with a higher level of education (bachelor’s degree) (p=0.001, Figure 1). The correlation between family issue or death of someone with over thinking of social life problems, Mood swings, difficulty in making decisions and poor concentration, financial problems, and sleep deprivation were significant toward the onset of the disease and recurrence of attacks (p=0.01).
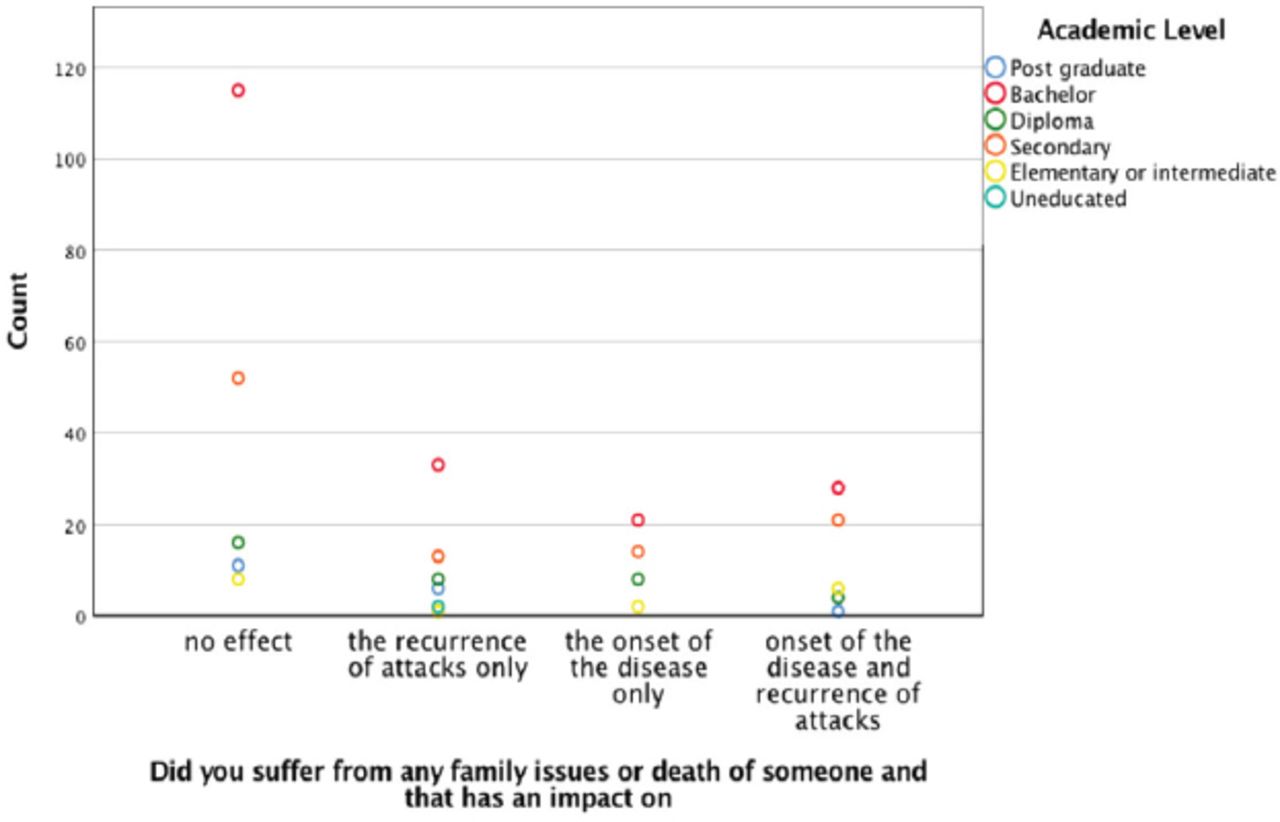
Correlation of family issues and death with patient’s academic level on the onset and recurrence of MS attacks.
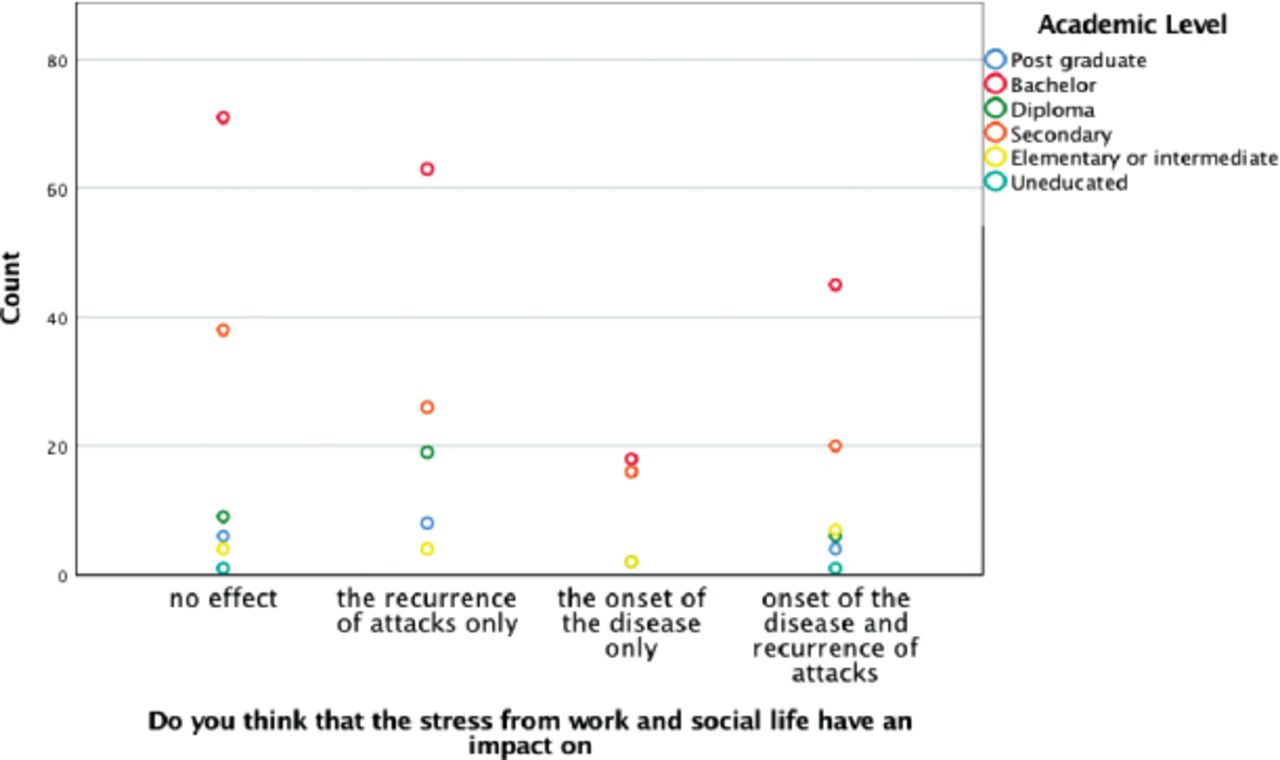
The direction based on the Likert-scale for the question (the impact of lifestyle and work stress on the disease) goes more with having an effect on recurrence of attacks only (mean±SD: 1.2±1.145). The percentage of patients who reported no effect was 34.9%, whereas 65.1% reported a positive effect either on the onset of the disease, relapse, or both. In addition, most of the patients who have a bachelor’s degree showed a significant p-value of 0.034 with the impact of lifestyle and work stress on the disease (Figure 2). The impact of lifestyle and work stress on patients who were diagnosed between 5 and 10 years from symptoms onset was significant (p=0.033). The correlation between lifestyle and work stress on the disease with over thinking of social life problems, mood swings, difficulty in making decisions and poor concentration, financial problems, and sleep deprivation were significant toward the onset of the disease and recurrence of attacks (p=0.01).
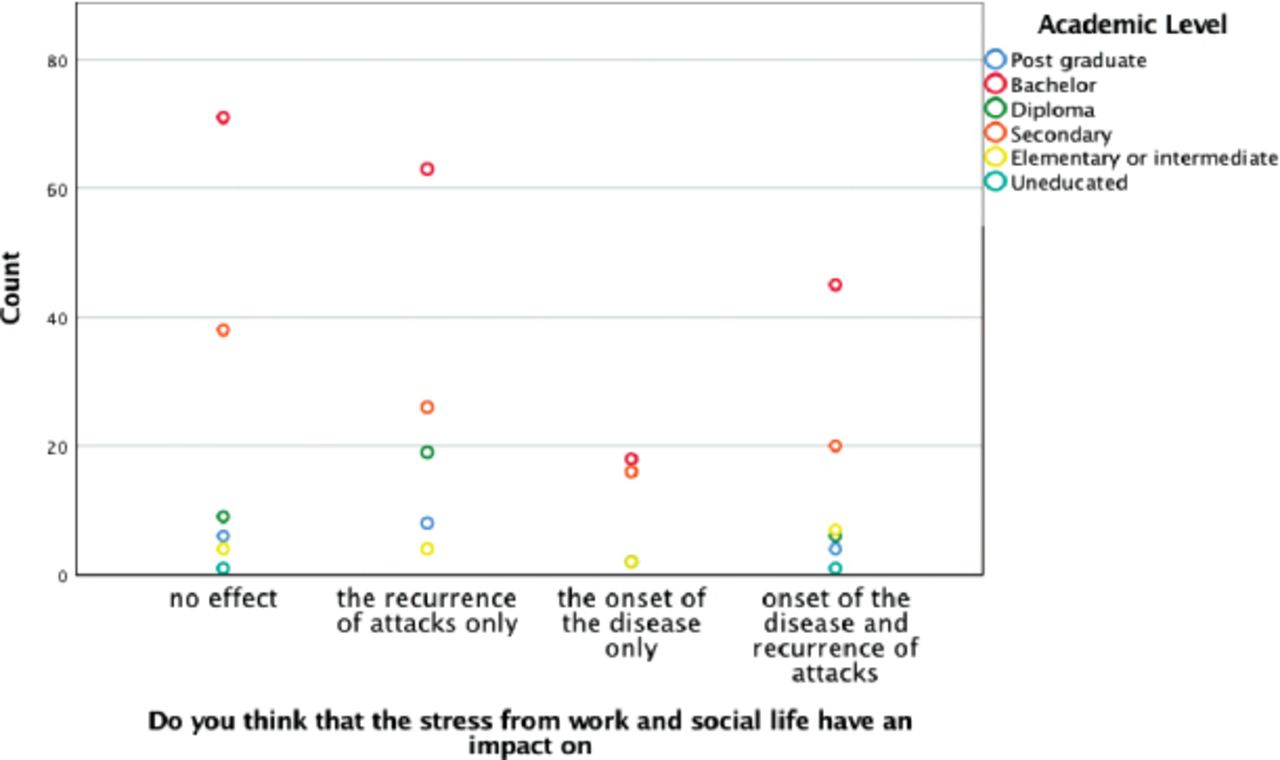
Correlation of stress from work and social life with patient’s academic level on the onset and recurrence of MS attacks.
Direction in Liker-scale carried out for the weather showed that cold weather had no effect on the disease (mean±SD: 0.34±0.744) whereas hot weather had an impact on the recurrence of attacks only (mean±SD: 0.88±0.896). Furthermore, a large percentage of patients (78.6%) stated that they were not affected by cold weather, but 45.9% noted they were affected by hot weather, especially on relapse, and the majority were diagnosed between 5 to 10 years of symptom onset (p=0.009). The direction in the Liker-scale for physical stress such as heavy exercise was toward the recurrence of attacks (mean±SD: 0.91±0.838). Approximately 48.6% of patients reported a relationship between physical stress and the recurrence of attacks. Table 3 summarize the results of sections 2 & 3.
Values for the 4-point Likert-scale for sections 2 & 3 questions.
Section 4
The majority of patients reported that over thinking of social life problems, mood swings, and sleep deprivation had an impact specifically on relapse and its severity, whereas only 26.5% reported that financial problems had an impact on relapses, and the direction of the mean for financial problems showed no effect. Table 4 presents the exact percentage for each factor. For all questions there was no significant correlation with academic level (p>0.05). There was insignificant correlation between marital status and overthinking of social life(p>0.05) which indicates that married patient who have social stress will not have effect on their disease. Career showed no relationship with financial problems (p>0.05) which indicates employed patients with financial problems will not have an impact on their disease compared with patients without financial problems.
Values for the 2-point Likert-scale for sections 4 questions.
Discussion
Our results showed that most of the patients were female and were 21-40 years old. Most were also married, which might be a risk factor for relapse, as it may add more physical and emotional stress. However, a previous study concluded that being married was associated with a good prognosis in terms of disease progression.7 In addition, our results demonstrate a direct relationship between patients with a higher academic level and MS disease because most of the patients had a bachelor’s degree, which was opposed by a study published in 2016 which showed an inverse relationship.8 Regarding the first and second questions that examined the effect of stress in general, such as work stress or family issues, the direction based on the Likert scale indicates more of an impact on relapse rather than onset. Physical activities such as weightlifting and sports affected relapse occurrence only in our study, possibly explained by the effect of air temperature and humidity, which can raise core temperature. Hot weather affected relapse only, supported by a previous study that stated “MS patients experience a transitory exacerbation of their symptoms when they are exposed to high temperatures such as hot weather or fever”.9 Although high temperature increases the number of relapses among MS patients, it can be a pseudo-exacerbation that was related to hot weather in some articles, that has not been evaluated in our study.10 According to our results, most of the patients reflected overthinking of social life problems even during their rest time. The emotional burden, mood swings, and difficulty in making decisions can have a large impact on their disease course, particularly in terms of relapse or its severity as well as in the quality of life and psychological well-being. Additionally, our results showed that the quality of patient’s sleep played a crucial role in the severity or recurrence of MS relapses, supported by a 2005 study noting that sleep problems are common in patients with MS.11
Patients who reported a negative effect of work and social life stressors were also suffering from other problems such as overthinking of social life issues and mood swings; all of these affecting MS relapse, but not onset. Work and social life stressors can cause sleep deprivation. Also, patients who stated that family problems or death of relatives affected their illness were also suffering from mood swings, and the presence of these 2 factors increase the likelihood of getting more relapses. Our study found that physical, emotional, and environmental stressors are related to relapses in multiple sclerosis. There was no association between MS onset and acute stressors. As for other studies that have investigated the relationship between MS disease and stress in all its forms, we found many studies but with different points of view and different conclusions. A study performed in 2013 found that the majority of MS patients were from 20-40 years of age, with twice the incidence in females compared to males.12 Regarding the relationship between patients with higher levels of education and MS disease, contrary to our findings a study published in 2016 showed no relationship. A systemic review published in 2015, which included 9 studies addressing the association of stress and the onset of MS, and 14 studies on the association between stress and MS progression, concluded that there was a strong association between stress and MS relapse, whereas there was no effect of stress on disease onset.13 Recent studies from 2017 found that physical activities of different types can slow the progression of MS and encouraged patients to exercise.14 Regarding mood, a 2003 study established that there were high levels of mood changes and distress in MS patients especially in the early period after the diagnosis.15 In 2014, a study concluded that the number of stressors, not their severity, was associated with MS relapses among Iranian patients.16
Study limitations
Subjective answers to questions as opposed to testing the health of the participants objectively before and after different types of stressors. Additionally, different types of MS disease could influence the results. Classifying patients based on their type can provide important results, as well as ruling out other diseases (confounders) could change some results. In addition, MS relapses should be differentiated from pseudo-exacerbation.
In conclusion, our epidemiological and statistical results are in line with the existing data. This study highlights the association between acute stress and relapse in MS, but not its onset. Our findings have implications for improving medical treatment and the lifestyle of patients with MS as a mean of relapse prevention. Such strategies include altering the lifestyles of MS patients and using stress management techniques on the clinical course of the disease. Additionally, we can prevent the severity and frequency of attacks by suggesting the implementation of a multidisciplinary team including psychologists, social workers, and occupational medicine specialists along with neurologists in the management of stressors encountered by MS patients.
Acknowledgment
We would like to thank Mr. Moharib Amir and Nuha Salem for their efforts with the SPSS program and data analysis, and the Arfa Society for Multiple Sclerosis Disease, Riyadh, Saudi Arabia for their help and support in the collection of some patients’ data. We also thank Ms. Ibtesam Belharith, the multiple sclerosis therapeutic nurse for her help and support in the clinic, and the English Editing Company (Editage) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 19, 2019.
- Accepted February 14, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.