


Abstract
Objectives: To compare King Saud University Medical City experience in laparoscopic liver resection with our previously established database for open resections.
Methods: A retrospective study was conducted at King Saud University Medical City, Riyadh, Saudi Arabia. All adult patients who underwent liver resection from 2006 to 2017 were included. Patients who had their procedure converted to open were excluded.
Results: Among the 111 liver resections included, 22 (19.8%) were performed laparoscopically and 89 (80.1%) were performed using the open technique. Malignancy was the most common indication in both groups (78.5%). The mean operative time was 275 min (SD 92.2) in the laparoscopic group versus 315 min (SD 104.3) in the open group. Intraoperative blood transfusion was required in the laparoscopic (9%) and open groups (31.4%). The morbidity rate was 13.6% in the laparoscopic group and 31.4% in the open group, and the mortality rate was 0% in the laparoscopic group and 5.6% in the open group.
Conclusion: Laparoscopic liver resection appears to be a safe technique and can be performed in various benign and malignant cases.
In the last 3 decades, laparoscopic surgical liver procedures have evolved rapidly and become the standard of care in many cases.1-3 In 1992, Gagner et al4 reported the first case of a laparoscopic non-anatomical liver resection for a focal nodular hyperplasia. A year later, Azagra et al5 performed the first laparoscopic anatomical resection. Since the publication of these case reports, multiple reports of major liver tri-segmentectomies and lobectomies have been recorded in the literature.6 Studies suggest laparoscopic liver resection minimizes the increase in portal hypertension, the risk of ascites, and postoperative bleeding.7 Moreover, it reduces insensible fluid loss because the viscera are not subjected to exposure. Therefore, the need for intravenous fluid is reduced, and third space sequestration associated with hyperaldosteronism is avoided.8 The laparoscopic techniques gained their appeal because of their numerous advantages in comparison with the open technique in terms of postoperative pain, hospital stay, return to activity, and abdominal wall preservation.1-3 However, laparoscopic liver resection is not without challenges, with many reports on the learning curves of performing such procedures.9 These points include the techniques for liver mobilization, vascular control, and parenchymal transection; the possibility of port site metastases, and the points related to the laparoscopic equipment.1 As majority of the lesions requiring liver resection are malignant tumors,1 laparoscopic liver resection oncological efficacy remains a point of debate; although several studies proved that expert surgical teams could perform a laparoscopic liver resection with a safety record that was indistinguishable from that of the open technique.5,8,10-14 Laparoscopic liver resection is a safe, evolving technique that should be thought as a first-line in various hepatic pathologies.
Methods
A retrospective study conducted at King Saud University Medical City, Riyadh, Kingdom of Saudi Arabia from 2006 to 2017. A total of 111 consecutive liver resections were performed: 89 were performed using the open technique and 22 using the laparoscopic technique. A written ethical approval was not obtained as the data collected retrospectively.
Patients who had their laparoscopic surgery converted to open were excluded.
The procedures were performed by 3 surgeons. Laparoscopic surgeries were performed in a low central venous pressure anesthesia. For left lobe lesions, patients were placed in a supine position, whereas for right lobe lesions, patients were placed in a left lateral position. Umbilical port was used for scope, in addition to 3 other working ports. Laparoscopic ultrasound was always performed, and line of resection is marked with cautery. We did not use Pringle’s maneuver during laparoscopic resection, and parenchyma was divided using harmonic scalpel. Large vessels and pedicles were stapled using a stapler, and specimen was retrieved using a bag through a Pfannenstiel incision. Demographic data, body mass index, past medical history, American Society of Anesthesiologists grade, pathology, operative details, and postoperative course were collected. Postoperative complications were graded using the Clavien-Dindo classification.15 Liver dysfunction was reported on the basis of the Schindl score,16 which defined dysfunction based on total serum bilirubin, lactate, prothrombin time, and encephalopathy. Mortality was defined as any death occurring in-hospital or within 90 days of surgery.
Statistical analysis
Data were analyzed using the Statistical Package for Social Studies version 22.0 (IBM Corp, Armonk, NY, USA). The continuous variables were expressed as the mean (standard deviation), and the categorical variables were expressed as percentages. Student’s t-test was used for the continuous variables, and the Chi-square test and Fisher’s exact test were used for the categorical variables. Survival curves were estimated using the Kaplan-Meier method, followed by the log rank test. A p=value of less than 0.05 was considered statistically significant.
Results
The mean age was 55.9 + 14.3 years in the laparoscopic group (LG) and 49.4 + 15.1 years in the open group (OG). Most of the patients in the LG were female at 63.6% (versus male patients at 36.3%), whereas most of the patients in the OG were male at 51.6% (versus female patients at 48.3%). The median preoperative hospitalization periods were 4 days (IQR: 1.5-5) in the LG and 4 days (IQR: 2-8) in the OG. The most common American Society of Anesthesiologists grade was grade II in both groups at 10 (45.45%) and 28 (31.46%) in the LG and OG, respectively (Table 1).
Comparison of the clinicopathologic features between the two groups.
The most common resection indication was malignancy-related pathology at 81.9% in the LG and 54.5% in the OG. Metastasis from colorectal cancer was the most common indication for both LG (77.7%) and OG (54.5%). Hepatocellular carcinoma was the second most common malignant indication. Benign disorders were only 15.9% in combination, with focal nodular hyperplasia being the most common benign condition in both LG (66.6%) and OG (28.5%) (Table 2).
Indications for liver resection.
The mean operative time was 275.3 min (92.2) in the LG and 315.6 min (104.3) in the OG. A major liver resection (defined as the resection of 3 or more segments) was performed in 36.3% (LG) and 44.9% (OG). Two patients (9%) required blood transfusion in the LG and 28 patients (31.4%) in the OG (p=0.015). Concurrent intra-abdominal surgery, which is defined as a major surgical procedure performed in the same setting, was performed in 13.6% (LG) and 7.8% (OG) (Table 3). Epidural anesthesia was used in only one patient (4.5%) in the LG and 33 (37%) in the OG (p<0.001).
Major intra-abdominal surgeries done in concurrent with liver resection in both groups.
Complications were graded according to the Clavien-Dindo classification. A Clavien–Dindo grade 1 or more accounted for 13.6% in the LG and 31.4% in the OG. Based on the Schindl score, severe liver dysfunction was noted in one patient in the LG and 12 in the OG (p<0.001). None of the 22 LG patients required postoperative blood transfusion, whereas 11 patients (12.3%) required it in the OG. One patient (4.5%) in the LG and 14 (15.7%) in the OG developed septic shock. The median total hospital stay was 9 days [IQR (7.5-11)] in the LG and 12 days [IQR (8.1-9.2)] in the OG (p=0.034). No 90-day mortality was seen in the LG, but it was observed in 5 patients in the OG. One case had a positive margin in the LG and 5 cases in the OG (Table 4).
Outcome of patients undergoing laparoscopic vs. open liver resection
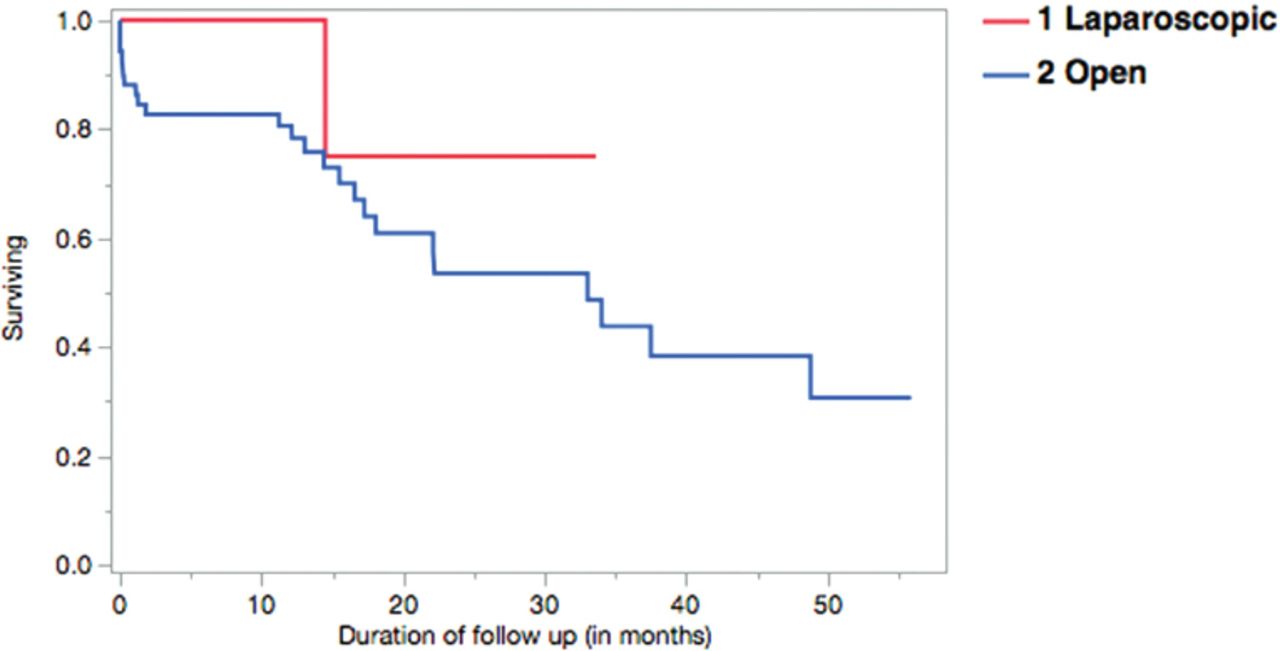
The median follow-up was 10 months (IQR: 3.25-21.85) for the LG patients and 13 months (IQR: 1.99-22.43) for the OG patients. Recurrence of the disease was observed in 4 cases in the LG, 2 developed intrahepatic recurrences, and 2 developed recurrence in the lung. In the OG, 27 cases had recurrence, mainly intrahepatic (21 cases), and 5 cases had recurrence in the lung. The median times to recurrence were 12.4 months (IQR: 1.80-18.80) in the LG and 5.78 months (IQR: 2.02-9.75) in the OG. The overall and disease-free survival curves are shown in Figures 1 and 2.

Kaplan-Meier overall survival for Laparoscopic Vs Open hepatectomy. Hazard ratios (HR) = 4.04 with (95% CI) = (0.54 – 30.11) and p=0.174.
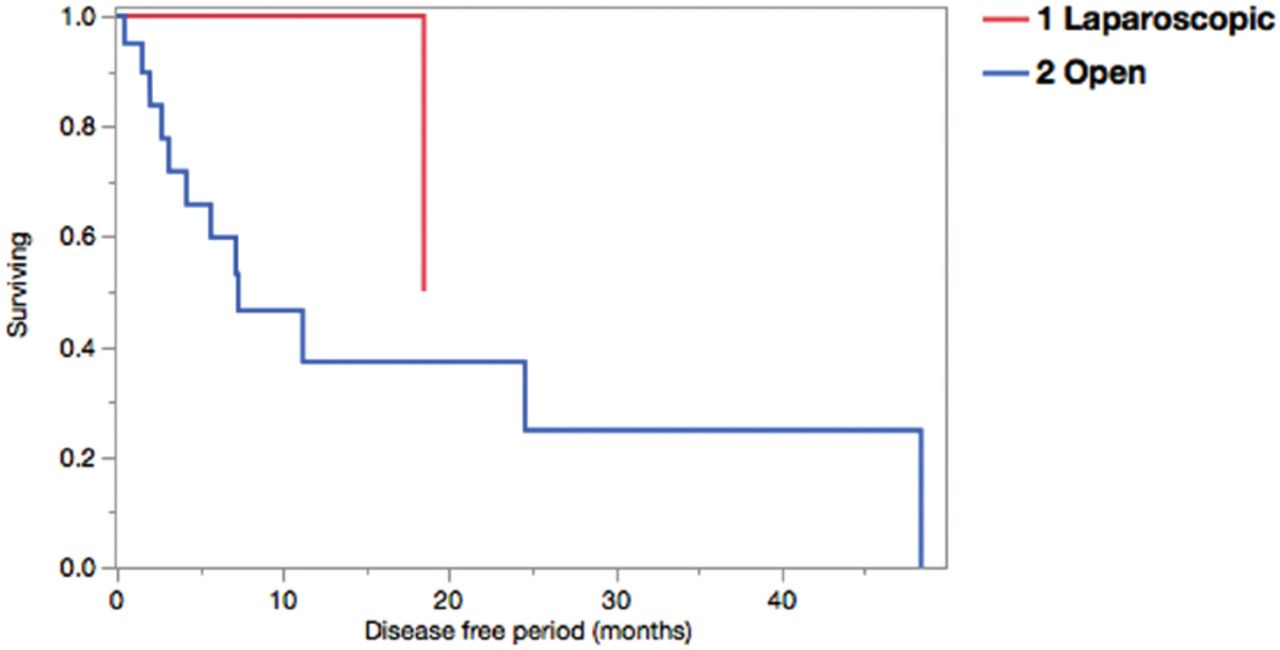
Kaplan-Meier disease-free survival for Laparoscopic Vs Open hepatectomy. Hazard ratios (HR) = 2.69 with (95% CI) = (0.39 – 21.41) and p=0.350.
Discussion
Laparoscopic liver resection is gaining popularity among hepatobiliary surgeons, and some authors consider it as the gold standard among favorable resections.17-19 In our study, we compared the open technique20 with the laparoscopic liver resection in cases performed at King Saud University Medical City, Riyadh, Saudi Arabia with a focus on morbidity, mortality, and several intraoperative variables. The rate of complications (13.6%) and the median hospital stay (9 days) in our LG were comparable with those in the literature.21-24 Silva et al25 and Kooby et al26 reported the poor effect of intraoperative blood transfusion on the post-liver resection outcome. In our study, the intraoperative requirement of blood transfusion was significantly lower in the LG. Postoperative liver dysfunction is a major cause of morbidity and mortality in post-hepatectomy patients.27 On the basis of the Schindl score, we found that the laparoscopic approach was superior to the open technique. No significant difference in the 90-day mortality was found between the 2 groups, consistent with recent studies.28-30 Epidural anesthesia is frequently used in major abdominal surgeries, including liver resections.31 The need for epidural analgesia was found to be significantly lower in the laparoscopic approach, and patients were placed on patient controlled analgesia instead. Most of the cases that required laparoscopic liver resection were malignant conditions, and metastatic colorectal cancer was the most common indication of liver resection. We found no difference in the surgical margin of resected specimens, as reported by Leong et al32 and Mala et al33 The differences between the 2 groups could be explained by volume disparity and selection bias. The unit is still early in the learning curve of laparoscopic liver surgery. Therefore, the main determinant of our approach is the lesion site, as more anterior lesions are easily feasible for laparoscopic surgery. Nevertheless, when we compared the patient characteristics between the OG and LG, we found no significant differences in the type of resection, body mass index, or age.
In conclusion, this study showed that laparoscopic liver surgery is feasible, safe, and comparable with the previously published open benchmark. However, additional prospective studies are required to overcome the small sample size and retrospective limitations. The further standardization of the technique and the accumulation of laparoscopic surgical experience in liver surgery are still needed to improve the outcomes and to extend our selection of cases.
Acknowledgment
We would like to thank Scribendi, Ontario, Canada (https://www.scribendi.com/) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 6, 2019.
- Accepted March 14, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Postoperative morbidity after liver resection- A Systemic review, meta-analysis, and metaregression of factors affecting them
- Recent trends in postoperative mortality after liver resection- A systemic review and metanalysis of studies published in last 5 years and metaregression of various factors affecting 90 days mortality