


Abstract
Objectives: To determine the factors associated with the development of methicillin-resistant Staphylococcus aureus (MRSA), hospital stay and mortality, and early versus late MRSA infection.
Methods: Cases (n=44) were intensive care unit (ICU) patients admitted to King Fahd Specialist Hospital, Al-Qassim, Saudi Arabia between 2015 and 2019 who developed MRSA during their hospital stay. Controls (n=48) were patients from the same place and period who did not develop MRSA. Data were abstracted from hospital records.
Results: Admission with sepsis (case: 46% vs. control: 2%, p<0.001) and having at least one comorbid condition (case: 95% vs. control: 46%, p<0.001) were significantly associated with the development of MRSA. Age (mean ± SD: case: 65±18, control: 64±18, p=0.7) and gender (% male, case: 52%, control: 56%, p=0.70) were not associated with the development of MRSA. Approximately 73% of all MRSA cases developed within the first 2 weeks of admission. Among the early cases, 44% died during their ICU stay; the corresponding percentage among the late cases was 42% (p=0.69). There was no difference between early and late MRSA cases in terms of non-sepsis admissions (50% vs. 67%, p=0.32) or comorbid status (at least one: 97% vs. 92%, p=0.17).
Conclusion: Sepsis and comorbid conditions were significant risk factors for MRSA development among hospital patients.
Patients in the hospital, particularly those in the intensive care unit (ICU), are at increased risk of contracting hospital-acquired infections.1 In addition to Escherichia coli, Klebsiella, Pseudomonas and Acinetobacter, Staphylococcus aureus (S. aureus) is a common organism responsible for such infections. Staphylococcus aureus is often resistant to commonly used antibiotics, such as methicillin (a ß-lactam of the penicillin class), amoxicillin, and penicillin.1 Methicillin-resistant Staphylococcus aureus (MRSA) commonly affects skin or soft-tissues and often occurs with other co-infections, such as a methicillin-resistant Pseudomonas infection.2 The majority of MRSA studies in Saudi Arabia have focused on epidemiological trends, including its prevalence and incidence among patients and healthcare workers, its source (for example, nosocomial or community-acquired), its various strains, and its response to antibiotics.3-11 Reported MRSA cases were highest in Riyadh (central) and Asir (southwest) regions, followed by Makkah and other cities in the western regions.3,6,7 The western city of Jeddah reported a prevalence as high as 38% among hospital patients.3 The majority of studies have reported a higher prevalence of MRSA in males than in females7,9 although contrary evidence does exist.4 A study from the neighboring United Arab Emirates identified female gender as a risk factor for incident MRSA among ambulatory patients who came to the hospital with a skin or soft tissue infection. Methicillin-resistant Staphylococcus aureus is more commonly acquired during hospital stay than from community living.12 Of the hospital-acquired MRSA, around half of the cases are actual infections, and the rest are colonization.13 Saudi Arabia and neighboring Gulf countries have observed a wide variety of strains among MRSA cases.5,10,11 The Muslim pilgrimages to Makkah and Medina might contribute to the propagation of diverse MRSA strains, as there is evidence of MRSA’s high transmissibility through the respiratory route.14 In fact, MRSA has been shown to be one of the main organisms that affects the pilgrims and causes them pneumonia.15 Though there is an abundance of MRSA studies on the disease itself in Saudi Arabia, there is limited evidence on patient outcomes.16-18 Available studies chose mortality as a patient outcome. The mortality was found to be high, but the rate varied among the studies.3,9 For example, in a study in Jeddah, 61% of MRSA patients died, 38% of whom died from their infection.3 Other patient outcomes such as prognostic factors or hospital stay were not evaluated. Studies from elsewhere in the world have reported older age, the severity of patient condition, longer hospital stay, and immunosuppression as risk factors associated with MRSA.17 Studies have shown that ICU patients who are MRSA-positive are more likely to develop a systemic MRSA infection and to have a longer hospital stay compared to patients who are MRSA-negative.18 For example, in Glasgow, United Kingdom, the development of MRSA among ICU patients significantly increased their length of hospital stay though it did not increase their risk of death.16
All available Saudi studies on MRSA are patient-only studies; in the absence of an appropriate control group, it is not possible to assess the factors related to the development and prognosis of MRSA. Hence, with a case-control design, the current study aimed to assess i) the factors related to the development of MRSA, ii) hospital stay and its association with mortality, and iii) the factors associated with early versus late MRSA development.
Methods
We conducted a case-control study in King Fahad Specialist Hospital (KFSH), Al-Qassim, Saudi Arabia. The Al-Qassim regional research ethics committee (Ministry of Health, approval number 20181118) reviewed and approved the study protocol.
Case definition are all patients who were ≥18 years of age admitted to the ICU of KFSH between January 2015 and November 2019 and were diagnosed with MRSA. They screened negative for MRSA at the beginning of their admission to the ICU. They developed MRSA thereafter, during their stay in the unit. A positive nasal swab (n=20), blood culture (n=12), wound culture (n=7), urine culture, or sputum culture (n=5) was used to confirm the diagnosis of MRSA (n=44). Pregnant patients were excluded.
Control definition are patients who were ≥18 years of age admitted to the ICU of KFSH anytime between January 2015 and November 2019 and did not develop MRSA during their ICU stay (n=48). Controls were matched with cases by age (±2 years).
We reviewed the medical records of cases and controls and extracted the following data: age, gender, nationality, admission diagnosis, admission date, MRSA culture date, duration to develop MRSA for cases (time to MRSA in days), antibiotic used for the treatment of MRSA, sepsis status (sepsis or septic shock, non-septic), comorbid conditions (chronic kidney injury, hypertension, diabetes mellitus), and outcome at discharge status (alive, deceased). We used the Charlson comorbidity index to identify patients’ comorbidities.19
Statistical analysis
We entered the extracted data into the IBM SPSS Statistics for Mac, version 24.0 (IBM Corp., Armonk, N.Y., USA). Descriptive statistics were reported with mean and standard deviation (SD) for continuous variables and frequency of figures and tables for categorical variables. We graphed the frequency of cases by time to develop MRSA (in weeks). Cases were defined as ‘early infection’ (within 2 weeks) and ‘late infection’ (after 2 weeks) based on the time it took them to develop MRSA.
We compared cases and controls by age, gender, admission status (septic, not septic), comorbid status (none, one condition, 2 or more conditions), antibiotic choice (vancomycin, linezolid), and deceased (yes, no). We also compared early and late cases by age, gender, admission status (septic, not septic), comorbid status (none, one condition, 2 or more conditions), antibiotic choice (vancomycin, linezolid), and deceased (yes, no).
Results
Between January 2015 and November 2019, 117 patients developed MRSA infection during their stay at KFSH. However, only 44 cases developed MRSA after their admission to the ICU and fulfilled the definition of cases to be included in the analyses. We identified 48 controls during the study period.
Comparison of cases and controls
. The mean ages of the cases and controls were 65 years (SD: 18, range: 47-83 years) and 64 years (SD: 18, range: 46-82 years). Males comprised 52% of the cases and 56% of the controls. The cases and controls did not statistically differ in age or gender. The frequency of non-septic admissions (55% vs. 98%, p<0.001) and of having at least one comorbid condition (96% vs. 46%, p<0.001) were significantly higher among the cases than controls. The majority of cases (57%) received vancomycin, while 43% received linezolid for treatment of MRSA. Among the cases, 43% died during their ICU stay; the corresponding percentage among the controls was 29% (p=0.214). Most cases and controls were non-septic on admission (Table 1). The distribution of comorbid conditions in our sample was as follows: diabetes (cases: 17, controls: 18), hypertension (cases: 20, controls: 18), chronic kidney disease (cases: 10, controls: 2), and miscellaneous conditions (cases: 25, controls: 8).
Descriptive comparison of Methicillin-resistant Staphylococcus aureus (MRSA) cases and controls.
Time to develop MRSA
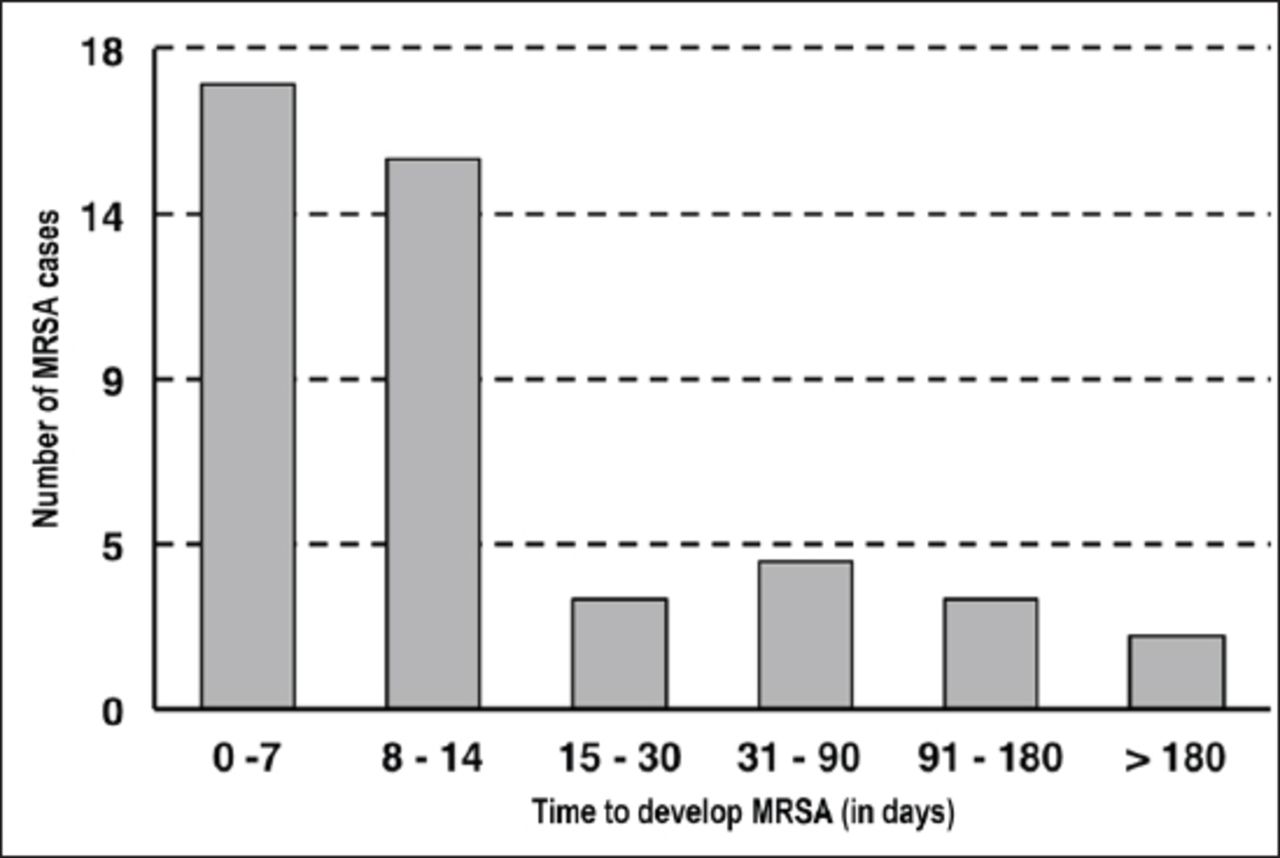
Time to MRSA was the difference between the date of admission to ICU and the date of the first MRSA-positive culture. No case developed MRSA before the third day of ICU admission. Most of the cases were diagnosed with MRSA within the first 2 weeks. Early cases (first 14 days) developed during the first week (n=17, 39%) and second week (n=15, 34%). Late cases developed during the third week (n=3, 7%), the fourth week (n=4, 9%), the fifth week (n=3, 7%), and sixth week (n = 2, 5%) (Figure 1). The largest proportion of cases (15%) started on the third day after ICU admission, followed by 11% on the sixth day; approximately 23% of all cases were positive for the infection within the first 5 days of ICU admission (data not shown).
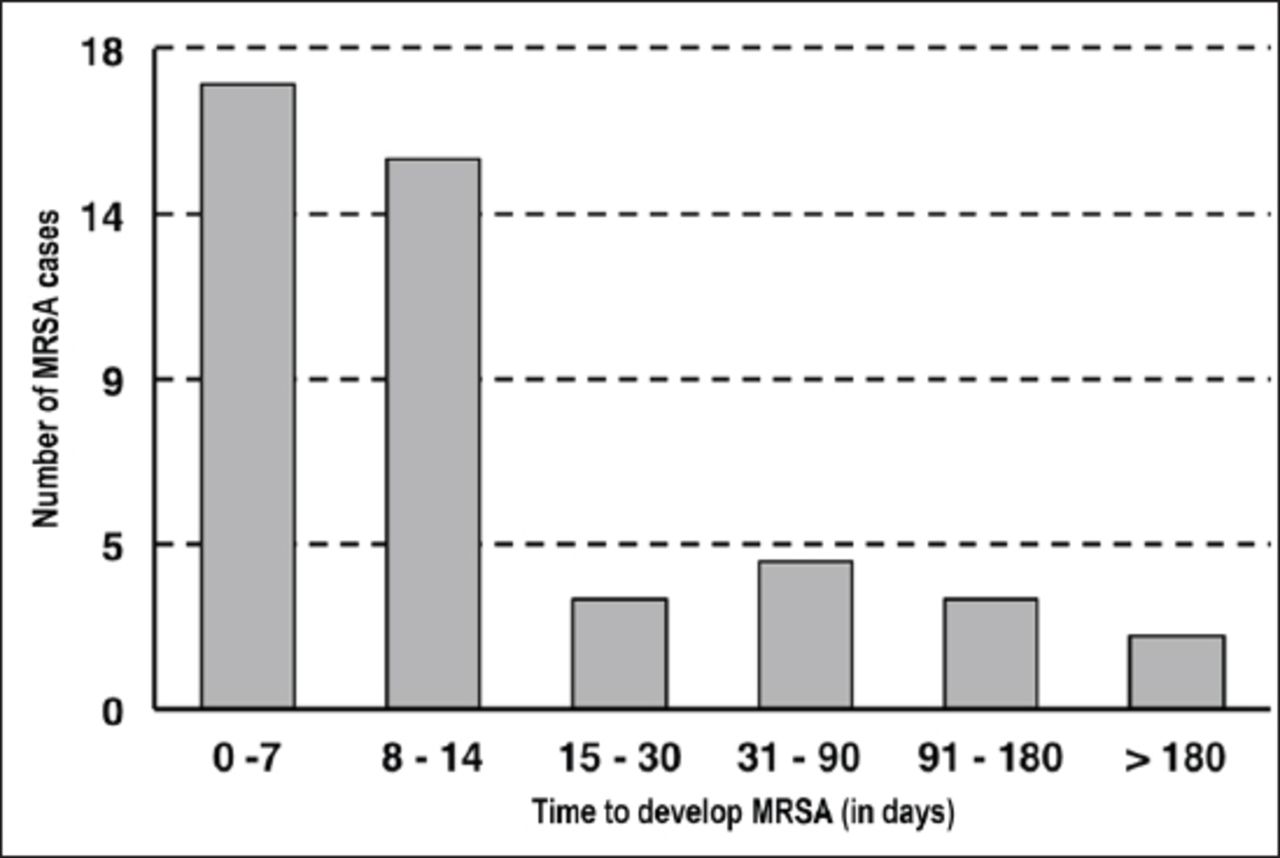
Bar graph of Methicillin-resistant Staphylococcus aureus (MRSA) development in the intensive care unit.
Comparison between early and late MRSA cases
The mean age of early cases was 63 years (SD: 18, range: 45-81 years); the mean age of late cases was 70 years (SD: 19, range: 51-89 years). Of the early cases, 59% were male. Of the late cases, 67% were female. There was no difference between the early and late MRSA cases in terms of non-sepsis admissions (50% vs. 67%, p=0.32) or comorbid status (at least one: 97% vs. 92%, p=0.17). The majority of early and late cases (56%, 58%) received vancomycin, followed by linezolid (44%, 42%) for the treatment of MRSA. Among the early cases, 44% died during their ICU stay; the corresponding percentage among the late cases was 42% (p=0.69) (Table 2).
Comparing early and late Methicillin-resistant Staphylococcus aureus (MRSA) cases (n =44).
Discussion
We explored factors associated with the development of MRSA among ICU patients as well as factors associated with early versus late MRSA infection. The salient findings of this study were the median time for developing MRSA was 10 days, the majority (73%) of MRSA cases developed within the first 2 weeks of admission, and 38.6% developed it in the first week. Patients who had ≥2 comorbid conditions were more likely (56%) to develop an early infection (≤2 weeks after admission), females were more likely than males (67% vs. 33%) to develop a late infection, and deaths were higher in females (n=3) as compared to males (n=2).
Studies in Saudi Arabia have focused on epidemiological trends of MRSA. For instance, Khanfar et al5 discussed the prevalence, incidence, and possible predictors of MRSA infection, while Eed et al20 discussed the molecular characteristics of MRSA among hospital isolates. Our study is the first in the region to address the in-hospital features of MRSA patients compared to controls. Internationally, though, there have been several case-control studies studying MRSA and its risk factors. When it comes to age group, patients with MRSA were younger (median, 61 vs. 70 years) than matched controls in a Danish study.21 In our study, the age difference between cases and controls was less tangible (65 in cases vs. 64 in controls). More consistent with our findings were those of a 2004 study of a similar design which reported the mean age among cases to be 68.2 ± 15.6 and 64.9 ± 19.9 among controls.22
The death rate in our study among MRSA cases was higher (43%) compared with the Spanish study (29.5%).23 In Jeddah, the total mortality rate of MRSA patients was 61%, of which only 38% were due to MRSA infection.3 Other studies in Saudi Arabia showed a 15% mortality in MRSA patients.9 The risk of developing MRSA is mainly related to an ICU stay of more than 4 days.2 This is in line with our findings, where no MRSA cases developed in the first 3 days of ICU admission. It has been shown that the detection of MRSA doubles within the first and second week of ICU admission.24 In our study, the majority of infections were detected within the first 2 weeks of ICU admission. Patients who were MRSA-positive after ICU admission were known to have lengthier hospital stays than MRSA-negative patients matched by age.16 Moreover, the risk of MRSA acquisition in ICU patients increases when patients have a confirmed non-MRSA infection within the first 2 days of ICU admission.16 Interestingly, results from a meta-analysis of risk factors associated with MRSA colonization showed that admission to an ICU was not associated with increased risk of MRSA colonization.25 However, exposure to nosocomial pathogens and prior hospitalization were associated with MRSA carriage, and the type of ICU admission, medical versus surgical, did have a significant association with MRSA carriage.25
While comorbid conditions have been associated with MRSA carriage,18 McMaster et al16 reported that MRSA in critically diseased patients did not significantly affect their mortality. In our sample, more males contracted MRSA infection than females. In addition, we found that patients who developed an early infection were more likely to be younger males with more than one comorbidity, while those who developed a late infection were older females with one comorbid condition. In 2013, a prospective study was conducted in Riyadh, Saudi Arabia that revealed a significantly higher prevalence rate in males (48%) than in females (32%).7 We reported that patients with multiple comorbidities were more susceptible to contracting a MRSA infection within the first 14 days of ICU admission. One postulation lies in privacy curtains; one study reported that curtains become contaminated within 3 days of being hung, with MRSA positivity increasing 10 to 14 days after curtains are hung around burn units.26
Study limitations
The study’s case-control design is inherently inferior to other designs. However, due to the rarity of the studied condition and the data available, a case-control study was the only feasible option. The case number was small. The case to control ratio was 1:1. Therefore, we did not have much statistical power to detect the difference between cases and controls or between early and late cases. We abstracted the data from medical records, but they did not have comprehensive information, which we could have used in our analysis. For example, the medical records stated that each patient tested negative for MRSA prior to admission to the ICU, but they did not specify the dates of screening. In addition, the full potential of the control group was not reached due to the lack of essential documented data (namely, time until discharge). If designed prospectively, we could investigate other factors that might impact the temporal effect of ICU stays and MRSA infection. A superior study design (namely, retrospective or prospective cohort) would better clarify this relationship.
In conclusion, the first 2 weeks after ICU admission are critical as most MRSA infections were acquired during that period, and more than a third occurred within the first 7 days. Patients with 2 or more comorbid conditions were more likely to develop an early infection. Females were more likely than males to develop a late infection, and deaths were higher in females as compared to males. Optimal care should be provided to all patients along with MRSA-specific preventive measures, especially during their first 2 weeks of ICU admission. Future studies should explore MRSA development in ICU patients in more depth.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 15, 2020.
- Accepted October 6, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.