


Abstract
Objectives: To explore the changing patterns of long-stay patients (LSP) to improve the utilization of pediatric intensive care units (PICUs) resources.
Methods: This is a 2-points cross-sectional study (5 years apart; 2014-2019) conducted among PICUs and SCICUs in Riyadh, Saudi Arabia. Children who have stayed in PICU for more than 21 days were included.
Results: Out of the 11 units approached, 10 (90%) agreed to participate. The prevalence of LSP in all these hospitals decreased from 32% (48/150) in 2014 to 23.4% (35/149) in 2019. The length of stay ranged from 22 days to 13.5 years. The majority of LSP had a neuromuscular or cardiac disease and were admitted with respiratory compromise. Ventilator-associated pneumonia was the most prevalent complication (37.5%). The most commonly used resources were mechanical ventilation (93.8%), antibiotics (60.4%), and blood-products transfusions (35.4%). The most common reason for the extended stay was medical reasons (51.1%), followed by a lack of family resources (26.5%) or lack of referral to long-term care facilities (22.4%).
Conclusion: A long-stay is associated with significant critical care bed occupancy, complications, and utilization of resources that could be otherwise utilized as surge capacity for critical care services. Decreasing occupancy in this multicenter study deserves further engagement of the healthcare leaders and families to maximize the utilization of resources.
A long-stay patient (LSP) in the intensive care unit (ICU) refers to a patient who survived the acute critical illness yet could not be discharged from intense monitoring or support. The time definition for long-stay varies in the literature. For instance, the definition of LSP in pediatric intensive care units (PICU) ranges from 13 to 56 days.1-6 Using a definition of a length of stay above the 95th percentile, some researchers proposed the definition of LSP as an ICU stay beyond 12-14 days.7
With the increase in the global cost of critical care, access to specialized acute care resources, and the availability of ICU beds has become an ongoing challenge. Thus, the patient required prolonged intensive care stay beyond the average length of stay even after adjustment for admission diagnosis and severity. In addition to the significant use of healthcare resources,8,9 Long-stay patients represent a significant proportion of ICU occupancy rates that will compromise the availability of critical care beds for other acute critically ill patients, especially during crises, such as COVID-19 global pandemic.5
Different approaches could be attempted to improve resource utilization in PICUs, given the unavoidable presence of LSP. However, there are discrepancies in the published data on pediatric LSP globally, with limited data about some regions with rapidly growing pediatric critical care services. This study aimed to gain more insight into the PICUs LSPs in such a growing population. As no previous publication on the subject was found in the medical literature through a PubMed search, we performed this 2-point cross-sectional study, 5 years apart, to describe the characteristics of LSPs and identify the magnitude of a long stay.
Methods
In this 2-point cross-sectional study, we approached all public PICUs, and pediatric surgical cardiac intensive care units (SCICUs) in Riyadh, Saudi Arabia, where it is estimated that 25% of the Saudi population lives while the remaining 75% are distributed over other cities.10 The inclusion criteria were all tertiary care, non-private hospitals in Riyadh. Private PICUs were excluded because they provide long-term facility services for some PICU patients. The literature proposes a wide range of definitions for LSP ranging from 13 to 56 days.1-6 We defined a long stay to be a stay of ≥21 days in the unit at the time of data collection. The research team used a structured case report to collect data on the medical condition of each LSP, including the source of admission, length of stay, diagnoses, comorbidities, complications, and the use of medical resources. Furthermore, the research team collected data related to the participating units using a questionnaire that was administered via a direct interview with the unit directors. The questionnaire was in English, paper-based, and was developed after reviewing the literature on LSP in the ICU setup, followed by 2 rounds of focus group meetings. The questionnaire addressed each unit’s resources, including bed capacity, bed occupancy rate, staffing, medical resources, the application of a “Do Not Resuscitate” policy, and the referral protocols of the hospital. Then it was piloted and tested for clarity and consistency. A pilot study was conducted in the pediatric and adult ICU at King Khaled University Hospital in Riyadh to validate the questionnaire among 2 intensivists. The questionnaire is provided as a supplemented file (Appendix 1).
We aimed to include all 11 public PICUs and pediatric SCICUs in Riyadh. Institutional Review Board approval was obtained before conducting the study (approval #13/3793/IRB), which waived the individual patient’s consent due to the de-identification of the data.
An appointment to visit each unit was set within 7 days before the interview by using a standard request form to obtain consent from the units’ heads. The data related to LSP characteristics were collected from electronic medical records by the units’ heads, then provided to the research team. All data, including patients and participating hospitals, were de-identified for privacy and confidentiality. Data collection started the first time in April 2014; then, a follow up for the LSP numbers and bed capacity of each PICU/CSICU was completed 5 years later in August 2019.
Statistical analysis
The means and standard deviations were used to describe continuous variables and frequency and percentages were applied to describe categorical variables. The histograms and the statistical Kolmogrove-Smirnov test of Normality were used to assess the Statistical Normality assumption of continuous variables Multiple response dichotomy analysis was used to describe the multiple response questions, and the bivariate Chi-squared was used to test the associations between categorically measured variables, the non-parametric Mann–Whitney (U) test of independent groups was used to assess the statistical significance of the differences on length of stay between the levels of the categorically measured variables, the median length of stay was reported due to the presence of distributional differences on mean LOS across the levels of some categorically measured variables. The IBM SPSS Statistics for Windows, version 21 (IBM Corp., Armonk, N.Y., USA) was used for the data analysis and the statistical significance level was considered at the 0.050 level.
Results
There were 8 PICUs and 3 pediatric SCICUs that met the inclusion criteria at the time of data collection in April 2014. Of the 11 PICU/CSICU units approached, 10 (90%) agreed to participate in the survey (Table 1). The prevalence of LSP in all the surveyed hospitals decreased from 32% (48/150) in 2014 to 23.4% (35/149) in 2019, resulting in an 8.6% decrease in prevalence (Figure 1). At an individual level, each unit varied in its improvement, from 5% up until a 33% decrease in LSP prevalence. An outlier was one hospital unit that had complete resolution of LSP (with no LSP cases in 2019, from 2 cases and a prevalence of 28.6% in 2014). Inversely, one CSICU had almost doubled in its unit LSP cases (from 25% to 45%).
Demographics of long-stay patients in the surveyed pediatric intensive care units (PICU) and pediatric surgical cardiac intensive care units (SCICU) in 2014.

Pediatric intensive care units (PICU) versus pediatric surgical cardiac intensive care units (SCICU) changes in the long stay bed occupancy (2014-2019) *p= 0.0112
These units had a total capacity of 155 beds. Forty-eight patients stayed ≥21 days, occupying approximately 31% of the total bed capacity of all the surveyed units. The length of PICU/SCICU stay ranged from 22 days to 13.5 years, and the median length of stay was 113.5 days. The median age of the patients was 316 days, and 68.1% were boys. Of all LSP, 72.9% were in PICUs, and the rest were in pediatric SCICUs. According to the source of admission, 31.3% were admitted from the emergency department, 27.1% from the ward, 25% were referred from another hospital, and the remaining 16.6% were admitted after surgical procedures.
We categorized the LSP into 2 subgroups: moderate LSP who stayed less than one year (n=31) and extreme LSP who stayed one year or more (n=17). A comparison between these 2 subgroups is shown in Table 1.
The most prevalent admitting cause and primary diagnoses among LSP are shown in Table 2. While the most prevalent admitting cause was respiratory disease (31%), the most common primary diagnosis was a neuromuscular disease (45.8%) followed by congenital heart disease (12.5%). In other words, the majority of LSP were patients who were known to have neuromuscular or cardiac disease and were admitted with respiratory compromise.
Admission cause and primary diagnosis at the intensive care unit admission.
Table 3 shows the complications and resource utilization by LSP over the preceding 3 weeks before the survey time. Ventilator-associated pneumonia (VAP) was the most common healthcare-associated infection (HCAI) in all surveyed LSP, occurring in 37.5% of patients. Central line-associated bloodstream infection (CLABSI) occurred in 22.9% of patients, and it occurred more often in the moderate LSP group. Catheter-associated urinary tract infection (CAUTI) occurred in 14.6% of patients, and this was more prevalent in extreme LSP. The most commonly utilized resources were mechanical ventilation, including non-invasive ventilation (93.8%), followed by antibiotic use (60.4%), blood product transfusions (35.4%), inotropes, and total parenteral nutrition (22.9% each), and renal replacement therapy (8.3%).
Complications and resource usage by long-stay patients (LSP)in the 3 weeks preceding the study.
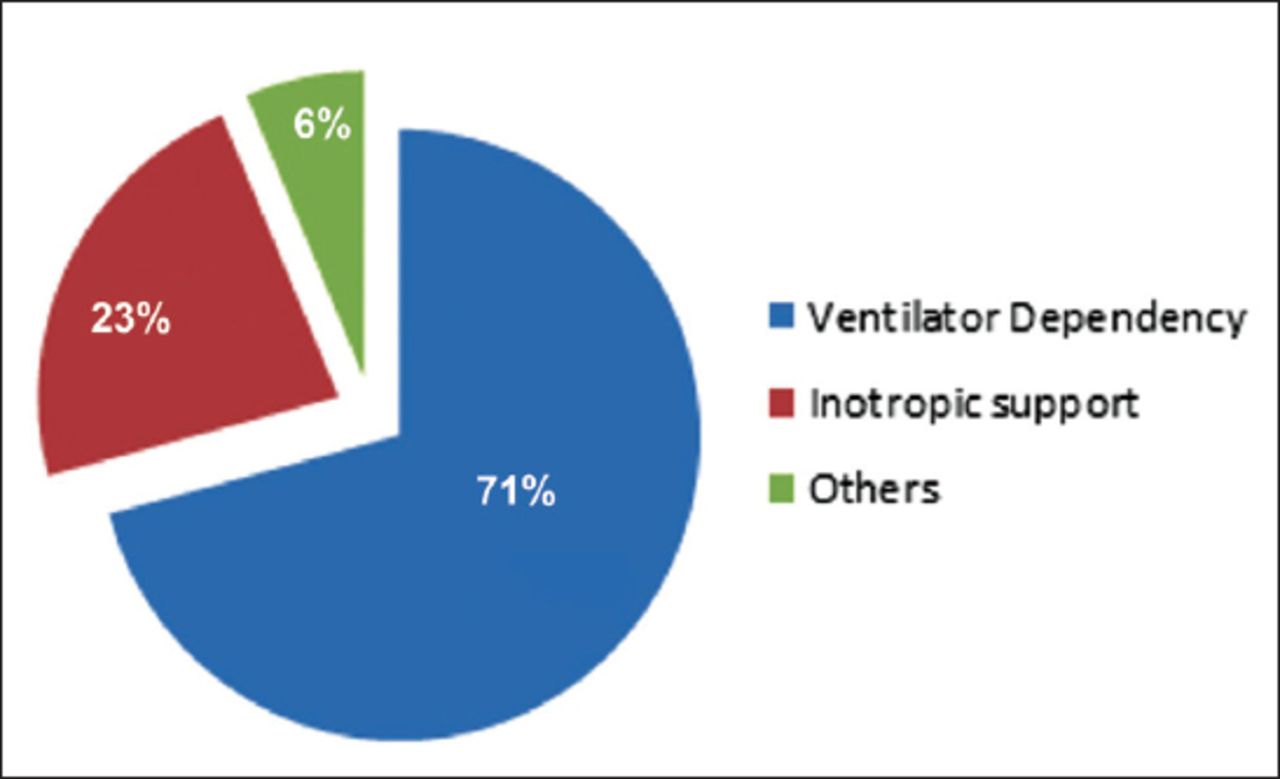
The most common reasons for the long stay in this study were medical reasons (51.1%), a lack of family resources such as home ventilator equipment (26.5%), and a lack of referral to long-term care facilities (22.4%). Ventilator dependency was the most common medical reason for a long stay in the unit (70.8%), followed by the need for inotropic support (22.9%). In contrast, tracheostomy care, fluctuating blood sugar levels, and the need for frequent suctioning of respiratory secretions accounted for the last 6.3% (Figure 2).
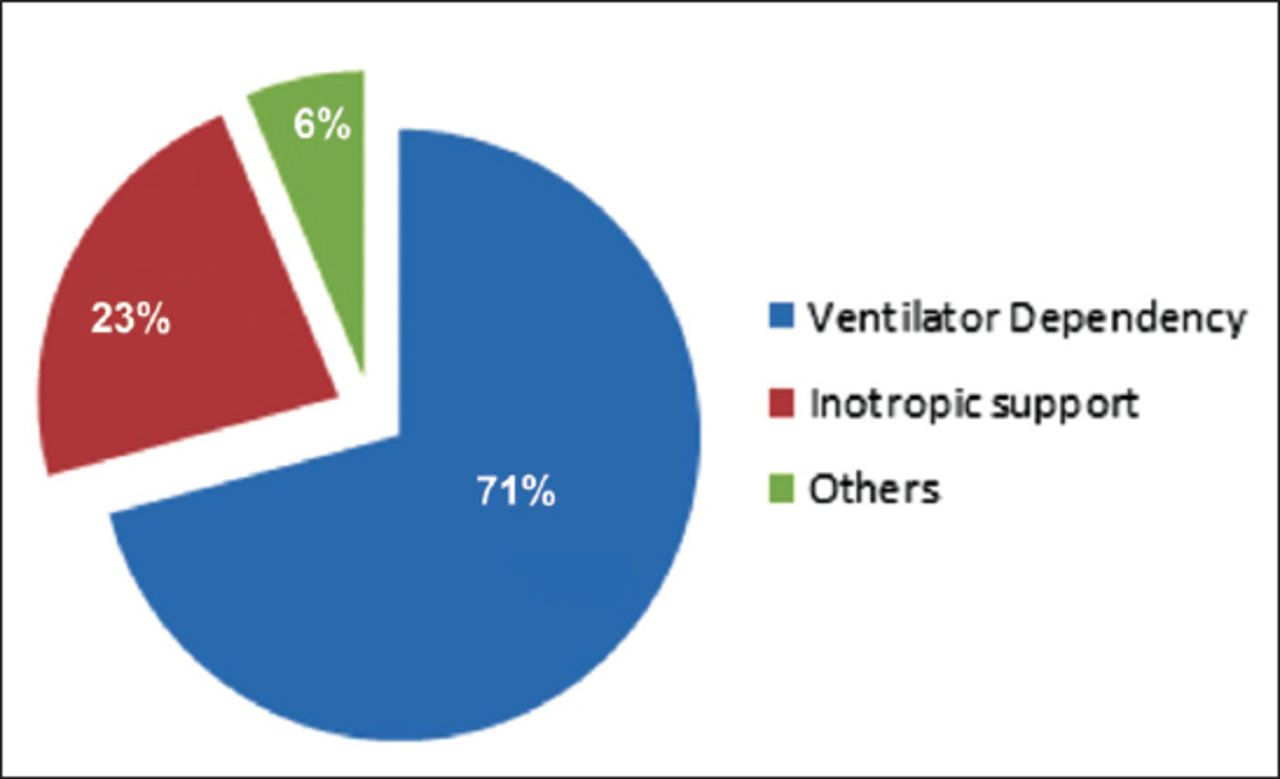
Medical reasons for the long stay in the pediatric intensive care units (PICU)/pediatric surgical cardiac intensive care units (SCICU) . Others: tracheostomy care, fluctuating blood sugar levels, and the need for frequent suctioning of respiratory secretions.
Our results showed that 50% of patients had daily visits from their families, while 22.9% were visited every other day to weekly, while the families rarely visited the remaining 27.1%. Noteworthy, 6 (60%) of the surveyed PICUs/CSICUs had a referral to other hospitals for long-term mechanical ventilation (MV), and 4 of these centers also had home ventilation programs.
Discussion
Pediatric intensive care units increasingly admit children with acute critical illnesses on top of chronic comorbidities, whose complex medical conditions eventually lead to prolonged PICU stays. Exploring and understanding long stay predisposing factors can help health care providers and institutions to manage LSPs and appropriately deal with their problems.11
In our 2014 cohort, children who stayed ≥21 days occupied about one-third of the PICU and pediatric SCICUs beds, but this has decreased over the previous 5 years to around one fourth. This is still relatively higher than the decreases in bed occupancy reported in previously published studies. Namachivayam et al reported that over 20 years, 233 LSPs needed 269 long-stay PICU admissions, accounting for 1% of all PICU admissions, and utilized 18.5% of occupied bed days.6 Their bed occupancy of LSPs almost tripled from 8% in 1989 to 21% in 2008 (p=0.001).6 Thus, it is vital to understand the LSPs’ characteristics to optimize new resource utilization. Exploring this issue in the pediatric critical care setting may be more relevant in the growing population, such as that of Saudi Arabia, where children represent 37.2% of the population as compared to 20% in the United States.12 As the pediatric critical care support progressed over the years, care in many high-income nations proceeded from treating mostly curable acute, life-threatening conditions to providing technologically advanced life-support and advanced care for patients with complex medical conditions.13 The need for mechanical ventilation and intravenous vasoactive drugs are important risk factors for an extended stay.5,6,9
A possible explanation for such a high number of LSP among PICUs might be attributed to the significant advancement and availability of critical care services over the past years with more life-sustaining treatments and interventions that might lead to LSP. We could not compare our current findings to those of previous reports owing to the lack of published data about this category of patients and limited database registry among different institutes for this specific problem, but comparing the 2014-2019 trends in the same PICUs/CSICUs showed a significant reduction of long-stay among PICUs’ patients, while the CSICUs continued to have high burden due to long stay, though this was inconstant among the included CSICUs. This could be attributed to more complex cases being admitted to the CSICU, as was observed in other settings.14
Another factor that might affect the ultimate outcome of LSPs is a conflict in the decision-making process regarding patient care either between the medical team and families (team-family conflict), among medical team members themselves (intra-team conflict) or within the family (intra-family conflict).15
Our finding that the primary diagnosis at admission was neuromuscular disease in almost half of the LSPs (45.8%) is in contrast to what was reported by González-Cortés et al5 where 75.9% of their LSPs were admitted for heart disease (surgical correction, heart transplantation, or heart failure as the most frequently reported causes of LSPs). This difference could be attributed to the high prevalence of neurogenetic diseases in Saudi Arabia due to consanguineous marriage, the involvement of children in motor car accidents with significant post-traumatic neurological sequelae, and relatively high prevalence of severe central nervous system infections that is commonly associated with chronic neurological sequelae.
The high rate of reported VAP and CLABSI among patients in the current study is in line with the findings of other studies that reported a significantly high incidence of nosocomial infection (96.3%) among LSPs.5 Namachivayam et al. also reported that more than two-thirds of children who stay in the PICU for ≥28 days had unfavorable health outcome (moderate disability, severe disability, or death).6
It has been reported that LSPs in the PICU require large proportions of resources, and the utilization of it considerably increases with time.6 A prolonged PICU stay is one direct measure of the usage of health resources. The PICU effect for mean length of stay (LOS) provides a marker of resource use, while the standardized mortality ratio (SMR) serves as an indicator of intensive care clinical performance, which when analyzed together illustrates efficiency.16,17 A higher number of LSPs in a PICU with a high SMR is considered inefficient, while a high LSPs in a PICU with a low SMR is considered effective but at the expense of high use resources.17 Significant utilization of healthcare resources was also reported in the literature, such as conventional mechanical ventilation (97.6%), blood product transfusions (90.2%), the requirement for intravenous vasoactive drugs (86.7%), and the need for extracorporeal membrane oxygenation (ECMO) in 22.9%.5 Another study found that among 3,483 PICU admissions, almost half of the patients had a complex chronic condition, with higher utilization of mechanical ventilation, central venous catheter, and arterial line monitoring.14
Other contributing factors to higher resource utilization are the frequent ICU-related complications that are associated with LSPs. Nosocomial infections are an important health problem even in children who stay more than 3 days in the PICU. Carcillo et al18 found that increasing age, cardiac arrest, or lymphopenia predisposed long-stay PICU patients to nosocomial infections. Furthermore, it has been reported that resistant bacterial infections can result in significantly increased LOS in the ICU, which increases the economic burden of treating those patients and increases the load on health care providers.19
Meeting the needs of families of critically ill children is increasingly recognized as an essential factor in the child’s outcome and the family’s interactions.20 Geoghegan et al20 found that LSPs families will likely become more familiar with the PICU environment and more knowledgeable about their child’s medical condition; therefore, there are more opportunities to provide parents with suitable resources to facilitate care for some of these LSPs at their homes. It was also reported that structured family meetings could be a practical approach to provide the required information and needed support for families of LSPs.21
Prolonged ICU stays can be challenging to families of children in many respects. Families of these children are prone to stress and exhaustion. Involving parents in the direct care of their child can help to normalize their experience and maintain the bonds between them and their child. Moreover, with more extended stays, there is an increasing chance of conflicts with the treatment team. Good physician communication is essential to avoid those conflicts and decrease the parents’ stress.20 Assigning one of the intensivists to be a primary physician for those patients and the key person to communicate with the family can help to address this issue.
Mechanical ventilation support represents the leading cause of LSPs in the PICU; hence, offering pediatric home mechanical ventilation (HMV) could be a solution for these children and their families. The decrease in LSP prevalence in our cohort may be partially due to available referrals to long term MV or HMV. Paulides et al reported a significant increase in the application of HMV in children, increasing from 8 children in their cohort in 1979-1988 to 122 in the 1999-2008 period. This mostly included the youngest age group (0-5 years old) with invasive HMV and was associated with a significant increase in the usage of PICU beds.22 This rapidly rising trend of HMV use in children with chronic respiratory deserves to be addresses early during the PICU course. A recent literature review showed that a protocolized family support intervention to improve communication between the ICU staff and families, and having a shared decision-making, reduced ICU LOS in critically ill patients without increasing the mortality.23 The ICU bed capacity can be rapidly overwhelmed during acute critical illnesses that constitute endemics or pandemics. Soon after completing the second phase of this study at the end of 2019, the global healthcare system was alarmed when coronavirus disease 2019 (COVID-19) emerged in Wuhan city and rapidly spread throughout China, then swiftly announced as a pandemic, as declared by WHO on March 12, 2020.24 With the estimated 5% ICU admission rate from China and up to 12% of the total positive cases in Italy, the high number of critically ill patients rapidly exceeds the adult ICU bed capacities.25,26 In Lombardy, Italy, the pre-crisis total ICU bed capacity was around 720 beds, with 85-90% bed occupancy rates during the winter months. One of the top priorities was to increase surge ICU capacity, with the health care on the ICU beds and available personnel, canceling nonurgent procedures, and providing additional 200 ICU beds to cope with the crisis. While the severity of COVID-19 is much less in the pediatric age group, many PICU beds could be utilized to increase the surge capacity in each hospital and healthcare setting.27 This gives further emphasis that LSPs are better transferred to long term healthcare facilities, which could improve the ICU bed availability during a crisis.
This multicenter, 2-point cross-sectional study analyzed LSPs in the tertiary PICUs in a capital city. Although the prevalence of LSPs was decreasing over the last 5 years, findings of the current study have major implications for the critical care setting in a rapidly progressing health care system in the COVD-19 crisis. Noteworthy, the paradoxical increase of LSPs in one SCICU deserves more attention. Future studies that examine the interaction between LSPs and ICU surge capacity may enhance the healthcare system flexibility to better deal with the outbreak crisis.
Study limitations
One limitation of our study is that the individual patients’ characteristics and outcomes were beyond the scope of this study as the main aim was to report the 2-point prevalence of LSP and related healthcare system factors. Therefore, the patients’ details were not explored in 2019. This has disabled potential comparative analysis of the risk factors’ changes related to patients over this period, and future studies could investigate this further.
In conclusion, long-stay patients in PICUs and pediatric SCICUs constitute a challenge for rapidly progressing health care systems and the higher demand for more critical care beds, especially during a pandemic and crises. Long stay is associated with significant critical care bed occupancy, complications, and utilization of resources that could be otherwise utilized as surge capacity for critical care services. Decreasing occupancy rates in this multicenter cohort deserve further engagement of the healthcare leaders and families to improve utilization of resources and make more beds available during a crisis for other critically ill patients.
Acknowledgment
The authors wish to acknowledge the efforts of Dr. Mohammed Almuaddi and the participating PICU/SCICU leaders for their valuable support. This research has been financially supported by Prince Abdullah Ben Khalid Celiac Disease Research Chair, under the Vice Deanship of Research Chairs, King Saud University, Riyadh, Kingdom of Saudi Arabia. We would like to thank the professional editors at Editage, a division of Cactus Communications. (https://www.editage.com/) for English language editing, and http://hodhodata.com/ for their Statistical Data Analysis.
Appendix: Data collection sheet for the long-stay patients in the pediatric intensive care units
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This study was financially supported by the Prince Abdullah Ben Khalid Celiac Disease Research Chair, under the Vice Deanship of Research Chairs, King Saud University, Riyadh, Kingdom of Saudi Arabia.
- Received July 19, 2019.
- Accepted September 29, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.