


CLINICAL PRACTICE GUIDELINES
The use of progesterone during pregnancy to prevent preterm birth
Alsulmi et al, address multiple current controversial areas regarding the prevention of preterm birth (PTB) to aid physicians with their clinical decision-making practice, including the use in multifetal gestation, different formulations, safety in pregnancy, dose and route of administration. Although strategies to increase the survival of premature infants have significantly improved in the past few decades, they have yet to be successful. Nine years ago, the use of progesterone in pregnancy was approved by the United States Food and Drug Administration for PTB prevention. The timing of therapy varied between studies and began as early as week 16 of gestation in women with a previous history of PTB. In some trials, treatment began between weeks 16-24 of pregnancy when an ultrasound scan diagnosed the short cervix. Other studies show no difference in the efficacy of progesterone therapy when initiated at 16-20 weeks compared to 20-26 weeks.64,65 Rebarber found in a retrospective analysis that early interruption of 17-OHPC therapy has been shown to increase spontaneous recurrent PTB risk.66 Therefore, continued treatment until 36-37 weeks of gestation is recommended.
see page 333
ORIGINAL ARTICLES
Combining bioinformatics and biological detection to identify novel biomarkers for diagnosis and prognosis of pulmonary tuberculosis
Zhao et al, identify the novel and promising indicators for pulmonary tuberculosis patients. The decrease rate of bacteria in patients with SLAMF8 or LILRB4 high expression was slower than that in patients with SLAMF8 or LILRB4 low expression. The mortality rate increased signidicantly in SLAMF8 or LILRB4 high expression group compared with SLAMF8 or LILRB4 low expression group. The study was carried out between June 2016 and June 2019. Three RNA sequencing or microarray datasets of tuberculosis infection were used to identify the potential genes showing a common expression trend.
see page 351

Heatmap analysis displaying the overlapped targets which were dis-regulated under tuberculosis infections among the Gene expression Omnibus public datasets GSE20050 (clinic), GSE57275 (in vivo), and GSE52819 (cultured cells based.
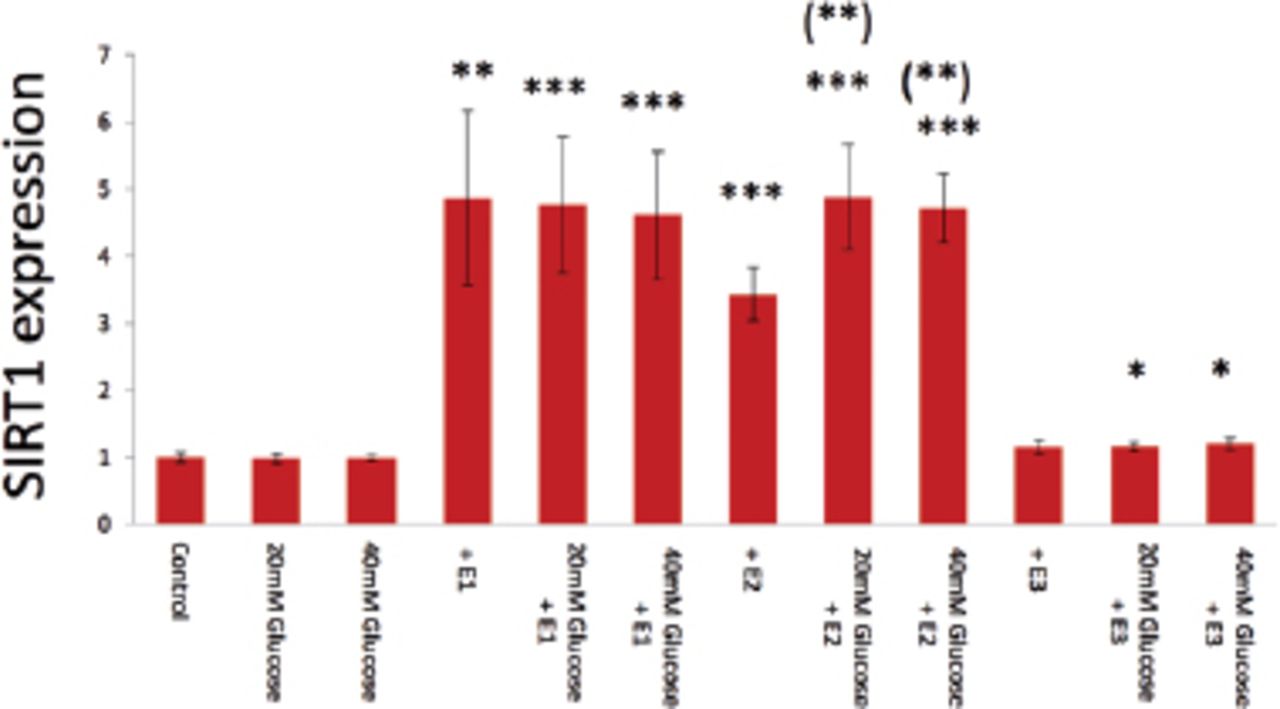
Effects of androgens and estrogens on sirtuin 1 gene expression in human aortic endothelial cells
Tsuchiya et al, investigate that dehydroepiandrostendione (DHEA), androstenedione, testosterone, estrone (E1), and estradiol (E2) definitely activate surtuin 1 (SIRT1) expression in human aortic endothelial cells (HAECs). A high glucose medium is potent to inhibit the basal gene expression; however, it could not reduce powerful androgen- and estrogen-induced SIRT1 expression in HAECs. Treatment with 20 mM or 40 mM glucose medium did not significantly inhibit E1- and E3-induced SIRT1 expression in control medium; however, both high glucose mediums significantly emphasized E2-induced SIRT1 expression in control medium (p=0.007, p=0.005, respectively).
see page 361

Glucose (20-40 mM) inhibition of E1-, E2-, and E3-induced SIRT1 expression in real-time PCR analysis.
CASE REPORT
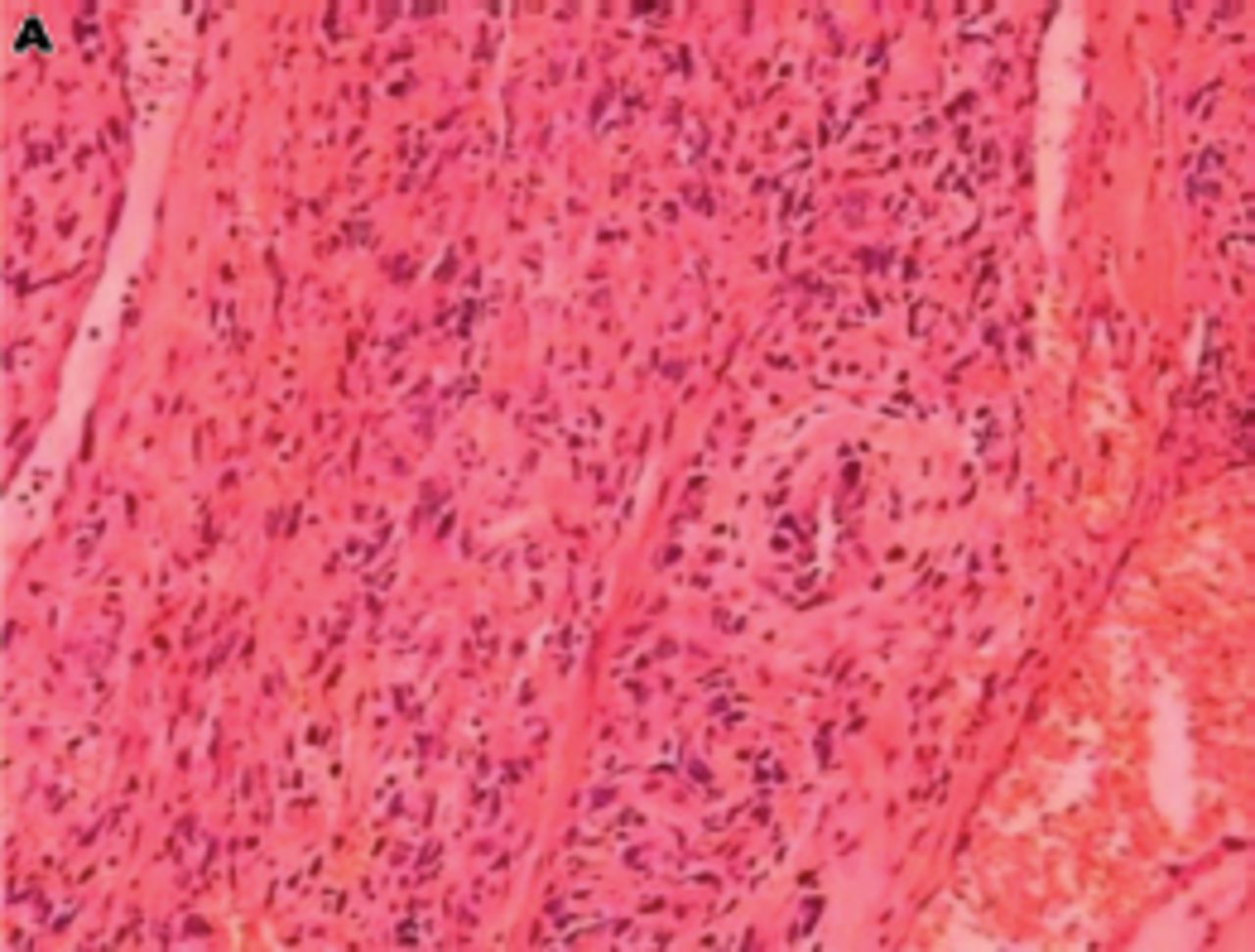
Primary pulmonary arterial sarcoma treated with endostar injection and radiotherapy
Xu et al presented a case of primary pulmonary arterial sarcoma (PPAS) treated with endostar injection and radiotherapy and discuss the diagnosis, clinical characteristics and pathology of PPAS. The patient complained of cough, sputum, fever, and chest pain with hemoptysis. Numerous nodules were seen in the computed tomography scan. The nodules shrunk after 5 courses of endostatin and one course of radiotherapy, as seen by computerized tomography scan. Current treatment is limited and includes surgery. Hence, endostatin injection combined with other therapy may be an alternative treatment.
see page 421

Tumor was composed of atypia ber-like spindle cells, HE×100.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.