


Abstract
Objectives: To analyze the fit of different competing factor models (a one-factor model, 3 2-factor models, and 2 4-factor models) of the Leeds sleep evaluation questionnaire (LSEQ) in the data from a Jordanian student population.
Methods: A cross-sectional study was conducted on university students, with 2 sleep-related tools - the LSEQ and the sleep hygiene index (SHI). The students (n=166) at Jordan University of Science and Technology, Irbid, Jordan participated in this study from January-April, 2019. A total of 12 LSEQ models (6 models with all 10-items, and 6 models with one item deleted) were evaluated by using confirmatory factor analysis. The summary statistics of correlation coefficients, descriptive measures of item analysis, the model fit, and Cronbach’s alpha were determined.
Results: The findings show that a 4-factor correlated solution was a plausible model for the LSEQ with 9-items, compared to a one-factor, 2-factor, and other 4-factor variant models. The deletion of one item from the original LSEQ improved the data fit significantly in the studied population. Moreover, correlation analysis between the LSEQ and SHI confirmed the divergent validity of the LSEQ.
Conclusion: The results support the validity of a 4-factor structure of the LSEQ with 9-items with adequate internal consistency and divergent validity.
Psychometrically sound assessment instruments are required to reliably assess health-related constructs in both clinical practice and research contexts. The tool development and validation process encompass approaches including exploratory factor analyses (EFA) and confirmatory factor analysis (CFA).1 Exploratory factor analyses is considered to be a part of the early-stage process in scale development; while, CFA is used in the process of scale validation, namely, in the later stages of the process.1 Related key measurement indices referred to in this manuscript also include internal consistency and divergent validity. Internal consistency refers to the degree to which all questions of a tool reflect the overall underlying construct, whereas divergent validity or discriminant validity helps to establish construct validity by discriminating the construct of interest from other constructs.2
Leeds sleep evaluation questionnaire (LSEQ) is a tool to evaluate sleep quality, which consists of 10 questions related to different sleep aspects. These aspects fall into 4 categories: going for sleep (GTS), sleep quality (QOS), episodes of wake after falling sleep (AFS), and symptoms after final waking (BFW).3 The LSEQ is an easily administered tool and can be obtained online at no cost. Though the LSEQ was initially developed for the use in patients undergoing psychopharmacology, its usefulness has been confirmed in several other populations.3 Moreover, the LSEQ can be used in a variety of settings, including clinical research.4
Earlier classical factor analytical studies on the factor structure of the LSEQ have identified a 4-factor model to be a better fit for this tool.5 However, there have been other CFA studies on the LSEQ, in diverse populations, with a multitude of different and unique models explored in those studies.2 We therefore, identified all the CFA models previously reported in the literature as well as other possible hypothesized models and compared those models. The objective of this study is to identify the best fitting model for the data collected from a sample of Jordanian university students. We further aim to propose, based on the comparative CFA analysis, a unique version of the LSEQ for widespread use in populations with similar characteristics as in the present study. Further, reliability and divergent validity of this version of the LSEQ was also assessed.
Methods
Participants were students from Jordan University of Science and Technology (JUST), Ibrid, Jordan. A total of 166 students, identified through simple random sampling, participated in the study from January-April 2019. Male students comprised 2/5th (80.5%) of the participating young people (mean age: 20.25±1.35 years). Subjects with self-reported problems of memory were excluded from participation. All participants were given a summary of the aims and methodology of the study. A modified English versions of the LSEQ and sleep hygiene index (SHI) were administered by the instructor to all the participants, and all participants provided filled-in answers for the LSEQ, and the SHI. The approval of the methodology and the permission for this research work was granted by the institutional review board of King Abdullah University Hospital, JUST, Ibrid, Jordan. During this study, ethical principles for human research in compliance with the Helsinki Declaration were followed. Informed written consent to participate and publish was obtained from the participants.
Leeds sleep evaluation questionnaire
The LSEQ is a 10-item questionnaire to assess the quality of sleep, with each item scored on a 100 mm visual analog scale.6 These 10 items are designed to test 4 sleep quality related constructs including the QOS, episodes of AFS, and symptoms BFW.3 The LSEQ is commonly scored with 0 indicating a description of poor sleep quality than usual and 100 indicating better sleep quality than usual. For the present study, a modified scoring criteria utilizing an ordinal scale (5-point; 0-4), with 0 implying the worst outcome and 4 indicating the best outcome was used. This modified criteria was chosen based on the respondent’s familiarity with Likert type ordinal response options. A similar adaptation in the LSEQ scoring criteria was published previously.2 A comprehensive review of the sleep quality evaluation tools, including the LSEQ, has summarized that the LSEQ demonstrates high test-retest reliability.4
Sleep hygiene index
The SHI was used in the present study to assess the divergent validity of the LSEQ. The SHI is a tool designed primarily to assess sleep hygiene, and it consists of 13 self-reported items.7 The SHI assesses the respondent’s behavior to sleep hygiene. The items of SHI were developed from criteria to identify poor sleep hygiene practices.8 Each SHI item is scored either 0 (no) or one (yes), and scores of all the 13 individual items are added linearly to generate a total score (range: 0-13). Higher SHI scores indicate poorer sleep hygiene behavior. It is one of the most widely used measures of sleep hygiene. The scale has shown favorable psychometric characteristics in both clinical and non-clinical samples.7,9
The factor structure of hypothesized models
One of the earliest and widely cited factor analytical studies of the LSEQ by Parrot and Hindmarch revealed 4 factors that pertained to sleep latency (items 1, 2, 3), sleep quality (items 4, 5), episodes of wake after falling sleep (items 6, 7) and symptoms after final waking (items 8, 9, 10).5 However, the fitness of this 4-factor model was questioned in subsequent investigations, and other competing models have been explored.2 Hence, to determine the best fitting model in the study population, we identified and tested 6 models of the LSEQ namely, a one-factor, correlated (a 2-factor and a 4-factor), 2-factor uncorrelated, and higher-order (a second-order 2-factor, and second-order 4-factor).
Statistical analysis
Statistical Package for Social Sciences for windows, Version 23.0 (IBM Corp., Armonk, NY, USA) was used to perform the statistical analysis. Various statistical measures were employed to determine that the LSEQ score had a suitable distribution for factor analysis in this population of Jordanian students. This included the results of the Kaiser-Meyer-Olkin test of sampling adequacy (0.76), Bartlett’s test of sphericity (p<0.001), a determinant score of 0.04, and the diagonal elements of the anti-image correlation matrix (0.60-0.88).1 Moreover, 13 out of 45, approximately one-third of the correlation coefficients between the LSEQ items were above 0.3 and significant.
A maximum likelihood (ML) estimation with Bollen-Stine bootstrap (n=500 simulated samples) was used to perform CFA. Bootstrapping was employed to manage multivariate normality issues. Maximum likelihood estimation was previously shown to be reasonable with the ordinal variable of 4 or more categories.10 Confirmatory factor analysis was used to get standardized factor loading values for each item of the LSEQ. A comparative CFA was performed on 6 previously described models of the LSEQ tool (Table 1). It is desirable to employ various types of fit indices belonging to different classes; therefore, we used 7 fit indices belonging to 4 classes.11 A p-value of ≥0.95 for goodness of fit index (GFI) and comparative fit index (CFI) implied an excellent fit for the model. A p-value of ≤0.08 for the root mean square error of approximation (RMSEA) was taken to show excellent fit.12,13 A p-value of ≤0.05 for root mean square residual (RMR) suggested adequate fit, while Chi-square/df (χ2/df) value of 3.0 or less implied excellent fit for the model.12,13
Fit statistics of the Leeds sleep evaluation questionnaire (LSEQ) in Jordanian university students.
The internal consistency of the LSEQ in the study population was determined by the Cronbach alpha test. Spearman’s correlation was used to evaluate internal homogeneity and the divergent validity of the LSEQ tool in the Jordanian university students.
Results
Table 2 presents the results of the preliminary item analysis. As shown in the skewness and kurtosis results, univariate normality issues were identified for most of the item scores, as well as the LSEQ total score. To address this issue, ML estimation with Bollen-Stine bootstrap (for n=500 simulated samples) was used to run CFA.
Descriptive statistics and divergent validity of the Leeds sleep evaluation questionnaire (LSEQ) in Jordanian university students.
Comparative CFA
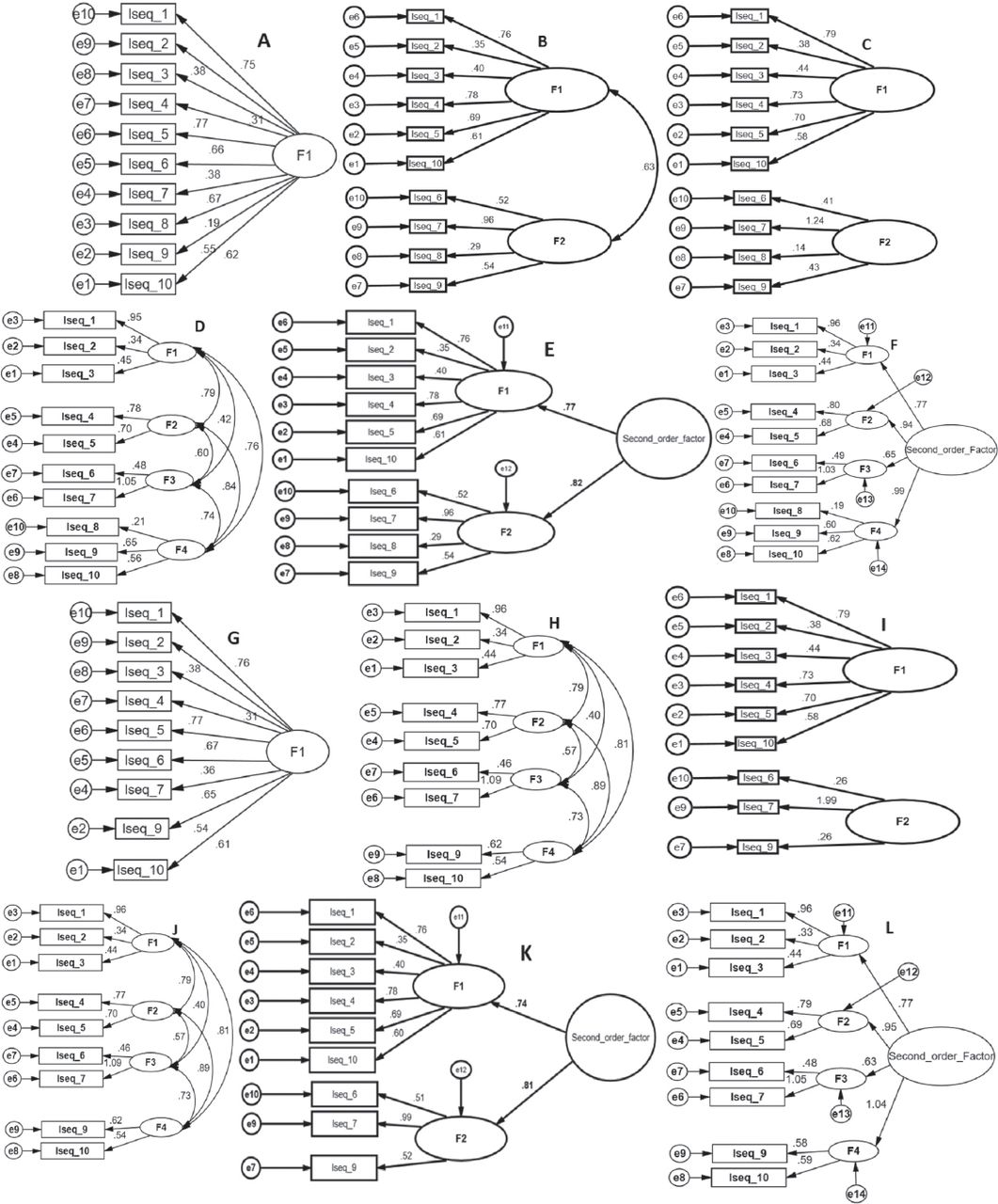
Fit statistics of the LSEQ models were tested, firstly with all 10 LSEQ items included, and next with one item (Item 8) deleted. A summary of the fit indices for all the tested models is presented in Table 1 & Figure 1.

Confirmatory factor analysis of the Leeds sleep evaluation questionnaire (LSEQ) in Jordanian university students. Items of the LSEQ (LSEQ-1 to LSEQ-10): A) 1-Factor model, B) 2-Factor correlated model, C) 2-Factor uncorrelated model, D) 4-Factor correlated model, E) 2-F second-order, F) 4-F second order, G) 1-Factor model without item-8, H) 2-Factor correlated model without item-8, I) 2-Factor uncorrelated model without item-8, J) 4-Factor correlated model without item-8, K) 2-F second-order without item-8, and L) 4-F second order without item-8.
Fit statistics for models with 10 LSEQ items are presented in Table 1.
Fit statistics for models without item-8 are summarized in Table 1 & Figure 1. The results of the CFA on these models are presented in Table 1.
The fit values indicated that the 4-factor correlated model with item-8 deleted showed a proper fit for the data obtained for the present study. Model D and Model J (Table 1 & Figure 1) represent the 4-factor correlated model with and without item 8, respectively. The choice of item deletion was based not only on the low factor loadings (0.21), but also on the improvements achieved in fit statistics if item-8 was deleted. As shown, a direct comparison of these 2 models indicated a dramatic change in fit indices values when item-8 was deleted. The notable differences between the 2 models included a ∆GFI: 0.03, an ∆IFI: 0.052, and ∆CFI: 0.052 (Table 1). A dramatic change of χ2 value was also noted (χ2=99.900 in model D to χ2=63.155 in model J). Furthermore, as shown in Figure 1, in none of the models from A to F, factor loadings for item 8 were more than 0.32.
Internal consistency
The LSEQ internal consistency was found to be adequate with a Cronbach’s alpha value of 0.81. The results of the internal homogeneity assessment of the LSEQ using the correlation between total score and item score is shown in Table 2. The p-values ranged from 0.37-0.82, and were significant at p<0.01, indicating moderate to a strong relationship.
Divergent construct validity
The LSEQ scale total score had a weak and significant correlation with the SHI total score (r=0.26, p<0.05), indicating the divergent validity of the tool. Correlations between individual LSEQ items and the SHI score also showed no to a weak relationship.
Discussion
The present study was designed to evaluate and compare the LSEQ factor models in our sample data, utilizing a comparative CFA analysis. Both published factor models, as well as models hypothesized using a conceptual framework of the LSEQ, were utilized to determine the extent to which our sample data support these models. This study utilized a comparative CFA framework in the LSEQ for the said objective in the study population. Overall, the results of the present study indicated that a 4-factor correlated model with one of the original LSEQ items (item-8) deleted was a plausible model.
Sample size adequacy
We have evaluated the sample size adequacy using several of the available measures and confirmed that these are satisfied by the LSEQ data in the study population. The relevance of this is to be noted as our study followed the standard practice of determining and establishing the data suitability assumptions of performing factor analysis.
Comparative confirmatory factor analysis
Only a few published studies evaluated the factor models of the LSEQ scale, and few of the studies have compared the fit indices of different competitive models using CFA.2 Some of the previous studies used only EFA to designate factors associated with LSEQ.5 In the present study, a total of 12 LSEQ models (6 models with all 10-items, and 6 models with one item deleted) were compared. The results indicated that a 4-factor correlated model was a plausible solution where all the tested fit indices improved compared to other competing models assessed. This result is in corroboration with the previously published studies reporting the plausibility of the 4-factor model.2,5 The similarities of the factor structure demonstrated in the current study and previous studies highlight that dimensionality of the LSEQ is relatively stable across populations. This is unlike other sleep evaluation tools such as the Pittsburgh sleep quality index and insomnia severity index, where the factor structure was reported to be multidimensional and varies between studied populations.14,15 Hence, the LSEQ may be suggested as a relatively better and stable construct for sleep quality evaluation globally.
However, it should be noted that, in the present study, further improvement in fit indices was achieved significantly, when the LSEQ item-8 was deleted. The item was how do you feel when you wake up (tired/alert) with response options from 0-4. The models where this item was included also lead to low factor loadings. Hence, the findings of the study support a 4-factor correlated model of the LSEQ with item-8 deleted.
Preliminary item analysis, internal consistency, and homogeneity
The internal consistency of the LSEQ in this study population was very good. Previous studies on the estimation of internal consistency and homogeneity also yielded similar results.2,16 Kim et al,16 found a higher value for Cronbach’s alpha (0.95) in Korean adults. Manzar et al,2 also found a slightly higher value for Cronbach’s alpha (0.84) in Ethiopian university students. The estimated value of the Cronbach’s alpha if item deleted, and item-total correlation coefficients in this study, indicate that the item scores of the LSEQ, had favorable ability to discriminate between low and high scorers.17,18
The correlation coefficients between the individual item scores and the total score of the LSEQ were moderate to strong; this favors the internal homogeneity of the LSEQ in the tested population. Internal consistency estimation helps in recognizing the homogeneity of items, or the magnitude to which the questions of a test quantify the same construct.19 The items of the LSEQ measures construct related to various characteristics of sleep quality. In this study, we have reported the internal consistency and item homogeneity of the LSEQ in an Asian university going student population.
Divergent validity
We tested the divergent validity of the LSEQ against the SHI.7 The bivariate correlations between the LSEQ and SHI scores were either non-significant or significant but weak, thereby confirming the divergent validity of the LSEQ.7 The LSEQ assesses the quality of sleep, and the SHI appraises sleep hygiene behaviors, these 2 tools assess 2 different components of sleep, which are slightly related constructs.7 This is one of the few studies to report the divergent validity of the LSEQ in any population. The LSEQ is a tool that effectively measures the construct of sleep quality, and it demonstrated an ability to discriminate against another construct,namely, SHI-a sleep hygiene measure.7
Study limitation
The limitations of the present study primarily included a narrow age group of the sample; hence, limiting the generalizability of the results. Further, the sample size was relatively smaller and was drawn from a pool of university students. Future research in multiple centers and with larger sample sizes is worth considering to investigate the factorial validity of the LSEQ. Such studies may help investigate measurement in variance of the factorial structure of the LSEQ with respect to time and sociodemographic characteristics.
In conclusion, the comparative CFA illustrated that a 4-factor correlated solution was a plausible model compared to a one-factor, 2-factor, and other 4-factor variant models. Moreover, the deletion of item-8 in the LSEQ improved the data fit significantly in a population of Jordanian university students. However, these results may not be generalizable to other populations, and future researches in diverse populations are required to test the impact of the deletion of item-8 in a 4-factor correlated solution. Future studies may also be required to test the related psychometric characteristics relevant to the clinical application of the LSEQ tool.
Acknowledgment
The authors would like to thank the Deanship of Scientific Research at Majmaah University, Majmaah, Kingdom of Saudi Arabia for supporting this work under Project Number No (RGP-2019-40). The authors gratefully acknowledge the participants for completing this study. Authors thank Editage services (https://www.editage.com) for English language editing.
Footnotes
Disclosure. This study was funded by the Deanship of Scientific Research at Majmaah University, Majmaah, Kingdom of Saudi Arabia, under project number (RGP-2019-40).
- Received March 20, 2020.
- Accepted June 3, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.