


Abstract
Objectives: To review the outcomes, success rate, and safety of women undergoing labor induction following a cesarean section.
Methods: This study is a retrospective review of all patients who had previous cesarean sections and were induced with prostaglandin (PGE2) or for various indications. This study was carried out at King Saud Medical City, Riyadh, Saudi Arabia between 2014 and 2019. Inclusion criteria were pregnant women with previous one lower segment cesarean section, singleton cephalic fetus, normal placenta, and passed 18 months or more from previous cesarean section.
Results: Records of 145 women were reviewed in the study, and the success rate of induction of labor was 59.3% (95% CI: 50.8-67.4%). The rate of uterine rupture was 1.4% and maternal complication was 4.8%. The induction success rate is higher in women who had previous successful vaginal delivery than those who had no previous vaginal delivery.
Conclusions: Labor induction can be considered safe in carefully selected cases owing to its good chance of success and no significant increase in maternal or fetal mortality and morbidity.
Induction of labor (IOL) is a standard obstetric procedure.1 The literature has extensively studied the mother and fetus’s efficacy and safety.2-5 However, IOL following a previous cesarean section (CS) remains controversial, particularly given its association with uterine rupture with reported rates of uterine rupture as high as 1.4%.6-8 The Royal College of Obstetricians and Gynaecologists (RCOG) recommends an IOL following a CS for most women after 37 weeks of gestation with the cephalic presentation, regardless of with or without a history vaginal delivery; furthermore, IOL following CS was reported to have a higher chance of success in women with previous vaginal delivery, regardless of whether the vaginal delivery was before or after the CS.9-10 Given the controversy on that matter and the potential benefits of IOL following CS, such as lower maternal morbidity, shorter postpartum period, and lowered risk of complications in a subsequent pregnancy due to abnormal placentation,11,12 it is worthwhile to explore and study the different techniques and protocols used for IOL following a CS. However, this topic also remains a grey zone, as no one protocol is recommended or reported to be superior over the others. The American College of Obstetricians and Gynecologists (ACOG) practice bulletin on the topic provides insight into the reasons for this unsettlement regarding the limited number of available evidence, with numerous limitations.13 The recent Cochrane systematic review concluded scarce evidence from randomized clinical trials to recommend IOL’s best method in women with previous CS.14 This study will present our hospital experience with IOL for women with previous CS, utilizing our institutionally approved protocol regarding maternal and fetal outcomes complications. It will also compare the subgroups of successful and failed IOLs.
Methods
This retrospective observational study was conducted at King Saud Medical City (KSMC), Riyadh, Saudi Arabia. King Saud Medical City is a tertiary referral center within the central (first) health care cluster. The study was approved by the local institutional review board (IRB) [H1R1-30-Jan19-01] with a waiver of consent owing to its retrospective design.
The study entailed a chart review of all pregnant women admitted between 2014 and 2019 to extract the enrolled subjects’ data according to the following inclusion criteria: pregnant women with previous one lower segment CS, singleton cephalic fetus, normal placenta, and passed 18 months or more from previous CS. Exclusion criteria include pregnant women with more than one lower segment CS, women who had a history of classical CS or previous myomectomy, multiple gestations, less than 18 months from previous CS, non cephalic fetuses, placenta previa and patients who refused induction labor.
Patients admitted for delivery and had previous one CS patients and received pharmacological IOL. Therefore, subjects were included in the analysis regardless of vaginal deliveries before or after the previous CS. Data of enrolled subjects were de-identified and recorded on a spreadsheet prepared by the study personnel. We recorded age, gestational age upon admission, parity, previous vaginal deliveries, reason of IOL, maximum dose of prostin received, duration of IOL until labor, the outcome of IOL either successful vaginal delivery or CS, maternal complication including placental abruption, rupture uterus, perineal laceration, postpartum hemorrhage or maternal death. Fetal complications including shoulder dystocia, fetal hypoxia, or intrauterine fetal death (IUFD).
Induction of labor protocol
Our hospital adopted the following protocol of IOL with previous CS: counselling was provided and obtaining written informed consent from the patient, including a detailed explanation of risks and benefits. Insertion of dinoprostone (prostaglandin E2 [Prostin E2TM, Pfizer, Kent, United Kingdom]) vaginal tablet in the posterior fornix. The dose of dinoprostone Prostin E2 was 1.5 mg, repeated every 8 hours, for a maximum of 18 mg. Syntocinon augmentation is at the discretion of the treating physician.
Statistical analysis
Categorical variables were summarized as number (percentage), whereas continuous variables were summarized as mean ± standard deviation (SD). Furthermore, a comparison of categorical data was performed using Chi-square or Fisher’s exact tests as appropriate, while the comparison of continuous data using student t-test or Mann Whitney tests as appropriate, all statistical tests were 2-tailed and considered statistically significant with p-values <0.05, without correction for multiple testing. A commercially available software package was used in the analysis (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP.)
Results
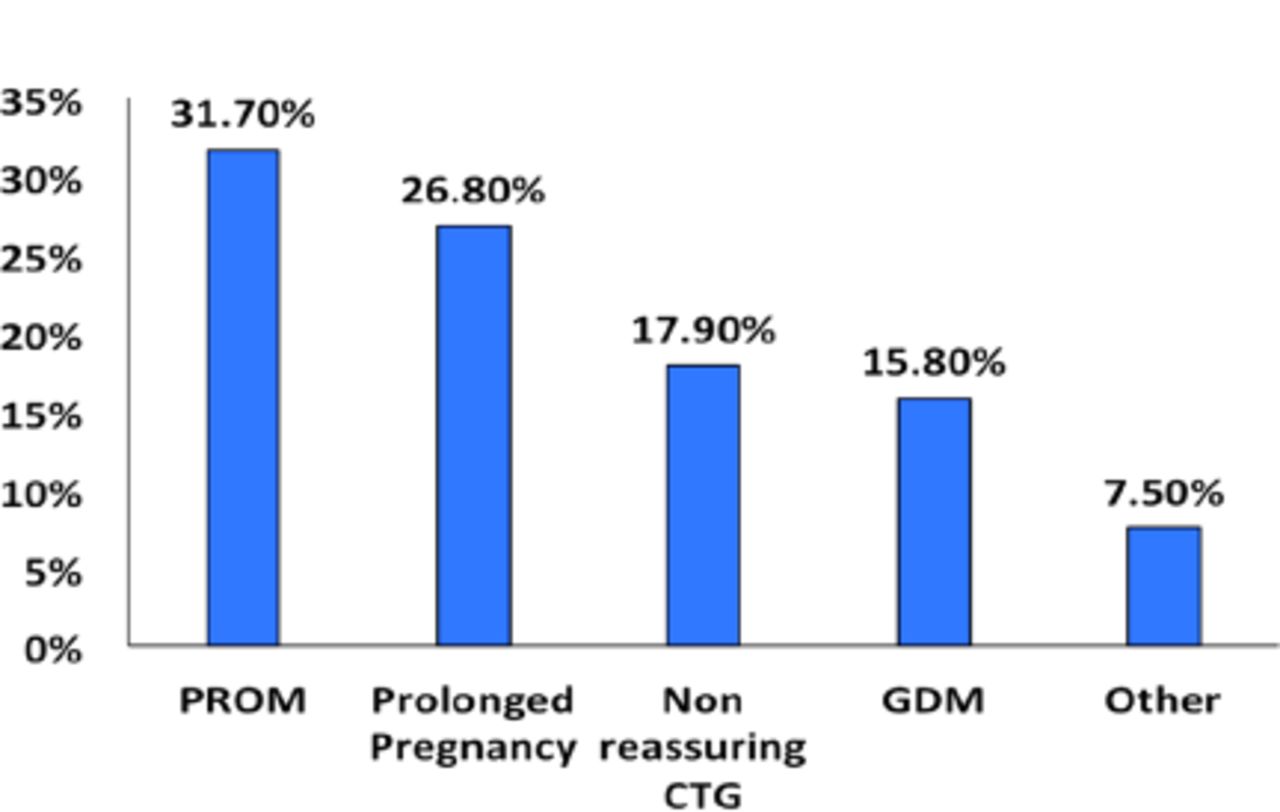
Chart review between 2014 and 2019 identified 145 patients who were eligible for the inclusion criteria of this study. The mean age of all included patients was 26.1 ± 6 years, and the gestational age was 40.6 ± 3.3 weeks; among all patients, 64 (44.1%) were para one with previous CS, while 81 (55.9%) as shown in Table 1. The participants were admitted for IOL due to various causes, among which premature rupture of membranes (PROM) was the most common (31.7%), followed by other reasons, as shown in Figure 1. The mean dose of Prostin for all patients was 4 ± 2.2 mg, and Syntocinon augmented labor induction in 13 (9%) cases.
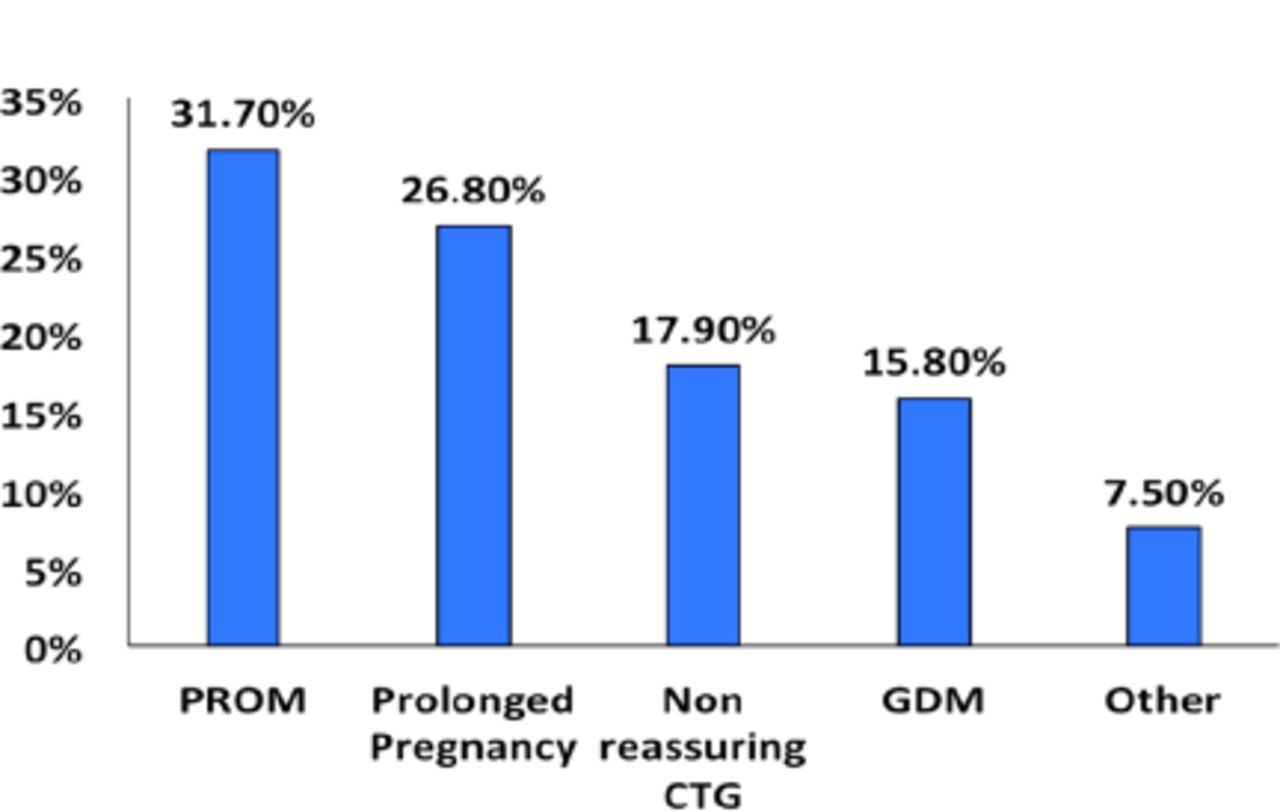
- Indications for Induction of labor. PROM: premature rupture of membranes, prolong: prolonged pregnancy beyond 41 weeks, GDM: gestational diabetes mellitus
- Comparison of successful and failed induction of labor (IOL) subgroups.
More importantly, the success rate of labor induction was 59.3% (95% CI: 50.8% - 67.4%). Among the 86 patients with successful IOL, 30 (34.9%) were para 1, while 56 (65.1%) were multiparous.
The subgroup analysis of patients with successful versus failed IOL indicates that both groups were of similar age and gestational age at the time of hospital admission. However, the successful IOL group included significantly more multiparous women than the failed IOL group (65% versus 42.4%, 95% CI of difference = 5.11% - 38.8%; p=0.01). Similarly, the successful IOL group utilized a significantly lower mean dose of Prostin than the failed IOL group (3.2 ± 0.2 versus 5.3 ± 0.3 mg, 95% CI of difference = 2.02-2.18; p<0.001). On the other hand, both groups showed no statistical differences in maternal and fetal complications (Table 1).
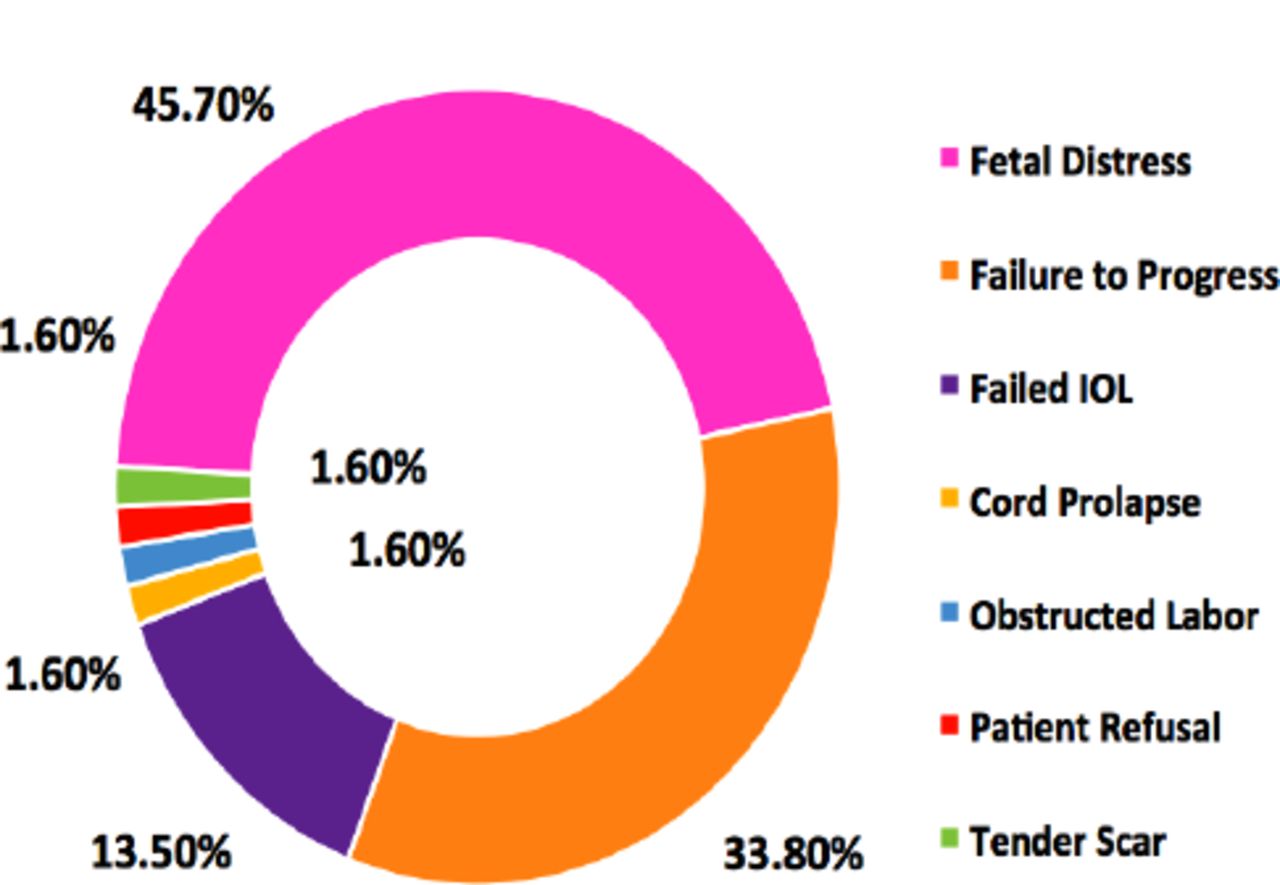
Further analyzed the subgroup of failed IOL for indications of CS, the most common indication was fetal distress, occurring in 45.8% of the cases, while refusal to continue IOL were infrequent indications and equally distributed with a percentage of about 1.7% as shown in Figure 2.
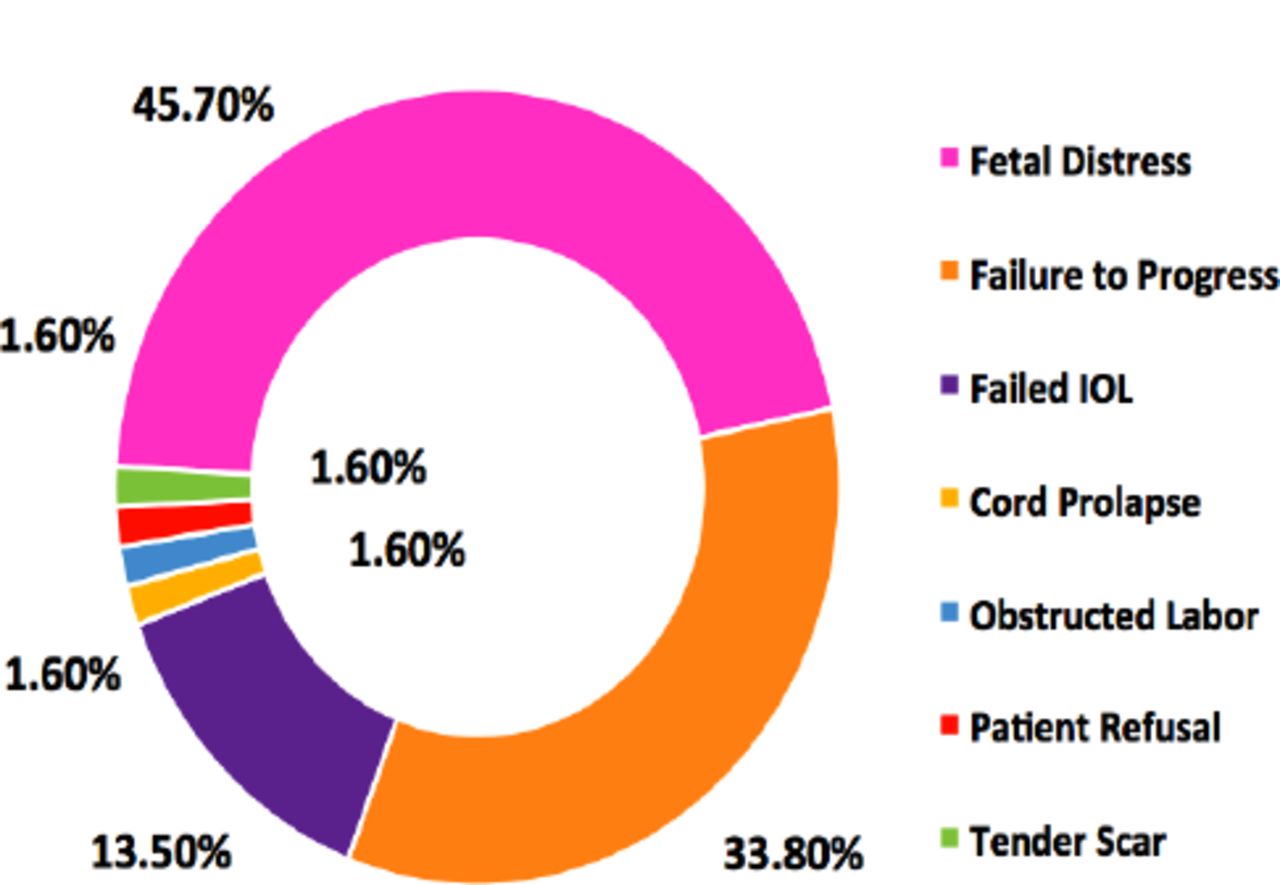
- Indications of CS in failed IOL subgroup. CS: caesarean section, IOL: induction of labor
Discussion
The maternity hospital at KSMC has 127 beds, and the average delivery rate over the past 6 years was approximately 6,000 per year; the CS rate ranges from 30-35 %, according to KSMC statistics. Most of the delivery in KSMC is for unbooked mothers, which represents approximately 70% of all deliveries. This study shows that women who were undergoing IOL following a previous CS revealed several key findings, the most important of which is the success rate of labor induction in the study population, the success rate in our study was 59.3%; this seems to be within the range of different reports on the same topic. In a larger study,14 the vaginal delivery rate for women with previous CS after IOL with the same induction agent as our study was 64.1%. In a more recent study,6 the group induced by prostaglandins had a vaginal delivery rate of 57.1%. Also, another study found that previous successful vaginal delivery had a higher successful IOL than women who did not (96% versus 84.9%; p<0.001).9 However, their more detailed analysis suggests that this association is only present when the vaginal delivery occurs between the previous CS and the induced labor, but not when it precedes it. The same result was reported in a large cohort study,15 where the rate of vaginal delivery in induced labor was 83.3% for women with a prior vaginal delivery compared to 51% only for women without induction.
In fact, in the current study, we involved either those who had a successful vaginal birth after CS (VBAC) before or those who had not. Our data suggest that IOL following a previous CS is safe both for the mother and fetus; the most critical expected complication (uterine rupture) occurred at a low rate of 1.4% in the whole cohort; others have also reported similarly low rates of uterine rupture ranging from as low as 0.4% up to 1.6%10,15,16 with variability between women with and without previous successful vaginal delivery. The overall morbidity rises with each CS, specifically for placenta previa, placenta accreta, and hysterectomy. The risk of labor induction in those with previous CS is mere regarding the scar dehiscence or rupture. Other studies showed an overall incidence of uterine rupture following labor induction varying from 0.2% to 0.9%.17
No trials were performed for labor induction with PGE2 vaginal tablets in a woman with previous CS. However, observational studies indicate an increased risk of uterine rupture, mainly when prostaglandins were used. Syntocinon augmentation can be used in selected cases, but it may increase the risk of rupture the uterus; one study shows that labor augmentation can be used after a previous CS even though oxytocin itself was found to be an independent risk factor for uterine rupture.18
This study showed that uterine rupture occurred in 2 patients (1.4%). Some reports suggested an increased risk of uterine rupture in patients undergoing TOLAC after PGE2 insertion.19,20 However, meta-analysis showed no association between prostaglandin and rupture uterus.21,22 The mean age of our participants was 26±6 years and was associated with 59.4% success rate. Reports showed that maternal age >35 years was associated with decreased chances of successful TOLAC.23,24 No maternal death was reported among participants. However, neonatal hypoxia occurred in one newborn and 2 IUFD due to multiple congenital anomalies. This study shows 1.4%, many other studies show encouraging results. Hence, it is reasonable to conclude that labor induction can be considered in carefully selected women with a previous CS. Due to the rise in CS in recent years, there were attempts to reduce the number of repeat CS, and IOL was considered in selected women with previous CS. This is particularly useful in places where people are opting for a large family. There is an increased incidence of complications like adherent placenta, adhesions, and injuries to vital structures associated with multiple CS, increasing maternal morbidity and mortality. The limitation of this study is a retrospective study, one center experience, and it includes patients who had successful vaginal birth after CS or not. A further randomized controlled trial is recommended.
In conclusions, IOL following a CS is safe for both the mother and fetus. It would harbor a higher chance of success if the woman had a successful vaginal delivery before the IOL trial at hand.
Acknowledgment
We want to thank Dr. Mufreh Asiri for his endless and kind support, guidance, motivation, and role in the manuscript drafting according to the journal style. Many thanks to the research center at King Saud Medical City, Riyadh, Saudi Arabia for the great support and facilitating statistical analysis.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 9, 2021.
- Accepted August 25, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.