


Abstract
Objectives: To evaluate the efficacy of older people health passport’s use by older people and health workers in primary health care centers (PHCCs) in 5 regions of Kingdom of Saudi Arabia (KSA).
Methods: A quasi-experimental pre-post study was conducted to evaluate the health knowledge, attitudes and practices before and after the use of older people health passport. A cross-sectional study on the use of passport was carried out among older people and their healthcare staff (doctors, nurses, and health educators) in selected PHCCs in 5 regions (Al-Ahsa, Jazan, Qassim, Asir, and the Northern Borders) in KSA from August 2019 to February 2020.
Results: Statistically significant improvement (p<0.001) in mean total score for health knowledge, attitude and practice post-utilization of health passport was found. The relationship between knowledge and practice post-passport use is stronger as compared to before use. More than half of older people (66.5%) reported using the health passport during the past 3 months when a medical service was required, 66.7% used it regularly and 81.2% were motivated to continue using it. Among the healthcare workers, statistically significant difference (p=0.039) was reported between the groups with regard to the use of health passport saving time and effort with more health educators (86.5%) in agreement.
Conclusion: Health passport use improved the health knowledge, attitude, and practice among the older people. Participant’s impression regarding its use was positive since majority reported a favorable experience.
The global population is currently witnessing a dramatic increase in the geriatric age group with an estimated 962 million people in the age group 60 years and above in 2017. The estimated number of people aged 65 years or above is 703 million in 2019 and is predicted to grow from 12-22% within the next 3 decades.1-3 In the Kingdom of Saudi Arabia (KSA), the older people (60 years and over) accounted for 5.5% of the total population in 2017 and it is predicted to reach 7.9% by 2025.4,5
The older people are a vulnerable group because of their functional decline and other complex unmet healthcare needs that compound their illness severity, complications, and mortality.6 Concomitantly, there has been an upsurge in the prevalence of chronic conditions among them leading to considerable problems such as lower quality of life, re-hospitalizations, and an increase in the financial burden on the healthcare system.7 This has prompted an agenda in the sustainable development goals to reduce mortality due to non-communicable diseases by one-third by 2030 mainly through prevention, control, and treatment.8
Therefore, older people have to follow complicated medication regimes, deal with self-management, often lack high-quality communication to support their complex disease management journey, and are at risk for several patient safety concerns.9-12 Evidence suggests that gaps in communication and incomplete documentation are responsible for many preventable adverse events and readmissions among the elderly.13 Another challenge is the failure to receive timely medical information due to fragmented uncoordinated care across multiple healthcare providers.14
In view of these concerns related to geriatric healthcare, it is suggested to improve care coordination and that physicians have access to the same comprehensive medical information of the older patients.15 Additionally, applying patient-centered healthcare enables the patients’ proactive participation in their chronic disease management and has shown benefits related to better treatment compliance, recovery, health outcomes, and quality of life.16,17
A useful tool in this regard that can potentially connect the patient and provider and improve patient outcomes is a health passport which refers to a brief document that favors coordination between the various healthcare staff engaged with the care of the patient.18,19 It contains extensive information related to medical history, medication, support needed for a healthy diet, and physical activity.18 They allow self-management among patients to better control long-standing chronic diseases that can improve compliance for preventive measures.20,21 In emergency care settings, health passports are beneficial since they provide an overview of vital patient information and assists in appropriate management. Health passports can be easily updated to keep track of all changes related to the individual’s health.18,22 Worldwide, they have been used for a variety of patient groups such as patients with heart failure, for dental problems, glaucoma, intellectual or developmental disabilities, and diabetes management.18,19,23-25 In KSA, the Ministry of Health (MOH) launched mother and child health passport in 2011 to improve the health care for the pregnant mother and her born child till the age of 6.26
Notwithstanding these benefits, the adoption of health passports has several factors influencing their adoption at different healthcare levels.25,27,28 A study identified that strong hospital leadership and multi- hospital commitment to implement the passport use are the key facilitators in its adoption.18 The barriers recognized were recurrent staff turnover and lack of follow-up with the agencies to ensure continuous use.18 Other barriers related to the healthcare providers include lack of attending physician support and awareness regarding the use of passports, clinician workflow, and recognition of the value of behavioral change.29-31 On the patient level, their health literacy, patient ethnicity, failure to keep the passport up-to-date, and potential loss of passport have been identified as barriers that influenced adoption.27-29
In view of these challenges related to the adoption of health passports, it is worth evaluating the implementation of this tool in relevant healthcare settings to be able to gain a deeper insight into the challenges likely to be encountered in the future and modify the passport as per the specific requirements of the setting, target population and the stake holders involved.
This study aims to test the efficacy of older people health passport’s use by older people and health care providers in primary health care centers (PHCCs) in 5 regions of KSA, to examine the experience of the older people in using the health passport with regard to comprehension and ease of use as well as perceived impact of the passport on communication and planning for health care; to examine the experience, obstacles, and feedback from the involved health care staff; and to assess the impact of the passport on older people’s health knowledge, attitudes and changes in practice.
Methods
A mixed study design was adopted to evaluate the efficacy of the health passport targeting 3 different components: i) Beneficiaries (older people) - a pre-post quasi-experiment was also carried out to compare changes in health knowledge, attitudes and practices (screening tests, lifestyle including physical activities and healthy nutrition) before and after the use of health passport. ii) Healthcare providers - a cross-sectional survey was conducted among health care workers including medical doctors, nurses and health educators regarding their feedback (such as experiences, recommendations, challenges during the implementation phase and methods for improvement) at the end of 24 weeks of using the health passport. iii) Passport content - a cross-sectional study design using a questionnaire for the post-implementation phase was used to obtain information on the health status and risk factors, drug usage, and referral status recorded in the passport.
The ethical approval for this study was obtained by the Research Ethics Committee at the MOH and Regional Committee for Research Ethics in the following regions, Asir region (No. H-06-B-091), Qassim region (No. H-04-Q-001), Northern borders (No. H-09-A-51), KSA, based on the Declaration of Helsinki. Each patient was informed on the purpose and nature of the study, consent to participate was obtained by written agreement. The participants were informed regarding their voluntary participation and the right to withdraw from the study at any stage. The confidentiality of the data was ensured and access to personal data within data sets was restricted to the investigator and not disclosed. The culture of informants was respected throughout the data collection process.
The health passport was designed as an evidence-based health education and health promotion tool for older people aged 50-80 years. Therefore, as a health promotion tool, it was planned to start using it at the age of 50 years in order to improve the health quality of this age group before reaching 60 and over. It is important to start early use since changing attitudes and practices at a later age will take time and will help prepare the passport users to adapt to aging-related changes and needs. Before beginning its use, the main aim of the passport was explained and illustrated for the older people as a tool to follow-up with their health and related investigations. Moreover, it was explained that 2 stages of life would be targeted, before aging (50-59 years) and aging stage of life (60 to >80 years). Instructions were provided regarding how to use it and its importance, followed by the user’s personal data, main chronic health problems, current medications, and recommended screening tests at each age group. All data could be updated as the person gets older and continues to use the passport.
The passport was divided into annual divisions, starting from the age of 50 years, for each year, 2 opposite pages were specified. The contents consisted of 3 parts. The first part was for clinical information of the elderly; it includes the date, annual results of the assessments, and clinical evaluations. The second part was the health education section and consisted of a variety of messages for the elderly or his caregiver targeting the education needed at that period on healthy lifestyle (healthy diet and physical activity), how to deal with chronic diseases to which they could be at risk and the recommended screening tests needed at each age group, its benefits, and recommended vaccinations. In between pages of the years, more detailed health information supported by illustrating photos or figures was provided aligned with the age-targeted at that point. For example, before the age of 60 years, education was focused on preparation for aging and promotion of a healthy lifestyle and planning for retirement. From 60 years and above the education targets healthy aging, independency in performing daily activities in addition to information, and advice on common geriatric health problems. The last message was regarding the international day of the elderly. The third part was for the notes to enable the passport user or their caregiver to document their preferences, comments, or inquiries.
The study was carried out in a selected PHCCs that implemented the older people health care program and provided health services for older people in 5 selected regions in KSA (namely, Al-Ahsa, Jazan, Qassim, Asir, and the Northern Borders). This study was conducted during the period between August 2019 to February 2020. A multi-stage cluster sampling method was used, by random selection of 5 regions from the 20 health regions in KSA, then from each region, random selection of the PHCCs that implemented the health passport was carried out. The target population included all persons aged 50 years and above who attended the selected PHCCs during the study period and agreed to participate in the study. Polit et al,32 describe that, the guiding principle is data saturation, where sampling is to the extent that no new information is being discovered and redundancy is achieved, demonstrating a convergence of opinion.
The sample size was calculated based on the target population (≥50 years) number which was 2,795,323,4 at 4% margin of error and 95% level of confidence, therefore the calculated sample size was 601 participants.33 The number of participants from each region was estimated according to the percentage (density) of the target age group in this region. The sample size was increased to approximately 50% above the calculated one, taking in account dropouts and to be more representative to the population. The study population included all people (aged 50 years and above) who attended the selected PHCCs and received and used the health passport during the study period, met the inclusion criteria, and agreed to participate in the study (n=1200). The inclusion criteria for participants were being PHCCs attendants (50 years and above), those who agreed to participate in the study and were able to communicate and answer the questions. The study excluded participants aged younger than 50 years, those who refused to participate in the study, and older people identified by staff to be patients whose physical, mental, or emotional capacity would prevent participation. The study population also consisted of health care providers (doctors, nurses, and health educators) who implemented the older people’s health passport study at the selected PHCCs and agreed to participate in the study (n=632).
The study was carried out in 2 phases. Phase 1 was conducted before receiving and using the health passport during which the pre-intervention questionnaire for the older persons was administered. Phase 2 was conducted after the passport was used by the older people for 24 weeks and then the post-intervention questionnaire was administered.
For the older people, 2 face-to-face interviewer administered semi-structured paper based questionnaires were used to collect the data from the participants. The pre-intervention questionnaire was administered before receiving and using the passport and consisted of 27 questions: 12 questions related to sociodemographic data, 9 questions to assess related knowledge and attitude towards health passport, 2 questions to assess knowledge on comprehensive geriatric assessment, 4 questions on early screening and lifestyle. The post-intervention questionnaire was administered after using the passport and consisted of 20 items: 7 questions related to use of the health passport in relation to the duration of use, comprehension, time spent in recording data and regularity of use, and 13 questions to assess their attitude and health knowledge after using the health passport.
For the healthcare providers, one self-administered questionnaire was used to explore their attitudes, believes, and challenges towards using the older people’s health passport. The Cronbach’s alpha for the questionnaire before using the health passport was 0.766, Cronbach’s alpha for the questionnaire after using the health passport was 0.796, and Cronbach’s alpha for the questionnaire of medical staff was 0.813 which reflect acceptable and good reliability (Appendix 1-3).
Statistical analysis
Data was analyzed by using the Statistical Package for Social Sciences version 22 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean±standard deviation (SD) and categorical variables were expressed as percentages. T-test and one-way ANOVA were used for continuous variables. The Cronbach’s alpha was used to assess the reliability of the questionnaire. Univariate logistic regression was used to assess the associated factors with a low level of the overall score for attitude, knowledge, and practice before and after using the health passport. A p-value<0.05 was considered significant.
Results
A total of 1200 patients and 632 healthcare workers were approached and invited to participate and all consented to take part. Out of these, 174 (14%) patient forms were excluded due to missing/invalid data. Thus, the final patient sample for analysis consisted of 1026 filled questionnaires.
The gender distribution in the sample study was approximately 50.5% male and 49.5% female. Majority of participants (41.5%) belonged to the age group 60-69 years. Most of them belonged to the region of Jazan (38.5%), followed by Asir (24.8%), Al-Ahsa (16.8%), Qassim (12.7%), and finally the lowest percentage from the Northern border (7.3%). Regarding the education level, approximately 47.6% of the respondents were illiterate. Occupation status of the respondents revealed that 40.2% were retired and 30.1% were unemployed. Furthermore, 87.8% reported to have caregivers at home and almost all of them were family members 98.2% (n=866). The summary of the characteristics is shown in Table 1.
- Sociodemographic characteristics of the participants (N=1026).
Among the healthcare workers (n=632) that participated in this study, nearly half of them were medical doctors (46.4%) and the other half were registered nurses (47.8%). A small minority (5.9%) of them were health educators. Almost half of the healthcare workers (45.9%) that responded belonged to the region of Jazan, followed by Asir (26.8%), Northern border (14.6%), and Qassim (10.8%). Very few healthcare workers (2%) belonged to Al-Ahsa region.
Experience of utilizing health passport by older people
An assessment regarding the use of the health passport among the participants revealed that 54.8% had obtained it for a duration of 2-3 months and approximately 98.1% of the participants mentioned that the contents were explained to them by the healthcare worker. Over half (66.5%) have used the passport when they required a medical service during the past 3 months, of which 66.7% used it regularly. A majority of the participants (81.5%) reported the time taken to fill information in the passport to be suitable. Likewise, nearly all the participants (93.5%) found the health information the passport to be clear and understandable. History of performing screening tests was reported by 83% of the respondents. The majority of the participants (81.2%) said they were motivated to continue the use of health passports regularly and would advise others to use it (90.5%, Table 2).
- Assessment of older participants experience during the use of the health passport.
Healthcare staff feedback and experience
Table 3 indicates the experience, obstacles and feedback of the healthcare staff according to their profession. More health educators (86.5%) agreed that utilization of health passport saved their time and effort as compared to doctors (75.6%) and nurses (69.3%) and the difference between the 3 professional groups was statistically significant (p=0.039). Regarding the agreement to continue using the health passports for older persons, 89.2% of health educators, 84.9% doctors, and 76.7% of nurses agreed (p=0.018). In terms of the suitability of time taken to use the health passport, 78.4% educators, 69.8% doctors, and 67.3% nurses found the time suitable, although the difference between the groups is not significant. A majority of the participants in all the 3 groups agreed that the passport helped in overcoming communication issues between the patient, their family and the health team, facilitated communication regarding daily treatment plans as well as future treatment plans; the difference between groups being non-significant.
- Healthcare staff feedback and experience.
Impact of passport on older people’s health knowledge, attitudes and practice
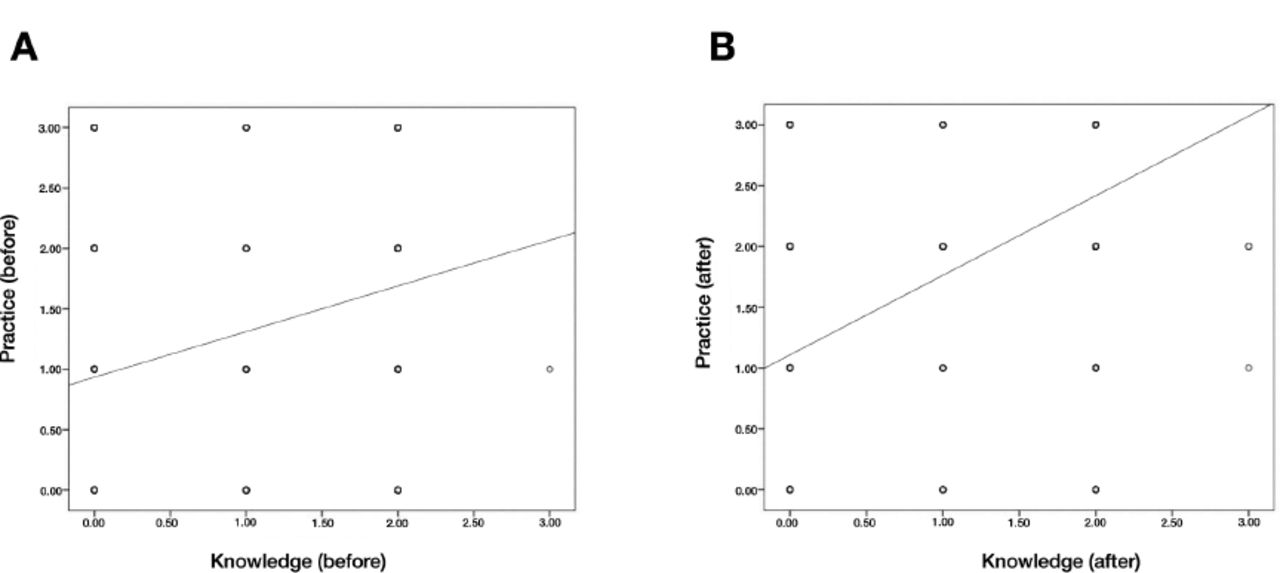
A comparison of the mean total score for attitude, knowledge and practice before and after the utilization of health passport revealed a statistically significant improvement (p<0.001) in all 3 aspects (Table 4). From Figure 1, it is clear that the relationship between knowledge and practice after using the health passport is stronger than the relationship between knowledge and practice before using the health passport where Pearson correlation coefficient (r) increased after using the health passport.
- Mean total score for attitude, knowledge, and practice before and after using the health passport.

- Relationship between knowledge and practice A) before using the health passport (r=0.299, p<0.001) and B) after using the health passport (r=0.466, p<0.001).
In relation to the demographic characteristics, a statistically significant improvement in cumulative mean score for attitude, knowledge and practice before and after the use of health passport was seen in both genders, all age groups, regions, educational levels and occupations (Table 5).
- Mean overall score for attitude, knowledge, and practice by demographic characteristics of the participants.
Discussion
An evaluation of older people’s health passport implementation across 5 regions within KSA was carried out to test the efficacy of health passports use by older people and health care providers.
This study demonstrated that the majority (81.2%) of the participants expected to continue using the health passport and recommend it to others (90.5%). This revealed a positive experience with respect to the health passport ease of use and comprehension among the older patients. This result ties well with a previous study wherein a favorable experience with using a health passport was attributed to ease of use and utility.18 Moreover, high acceptance can be further speculated based on an earlier study that cited low clinician engagement with the health passport as a barrier to successful use.34 Conversely, in the present study since nearly all the participants (98.1%) agreed that the healthcare worker helped them understand the contents of the passport; this implies that the healthcare team was actively involved in implementing the health passports and this could be considered as a facilitating factor that enhanced the experience of the patients.
Regarding the experience of the healthcare team, the study illustrated that in general, an overall positive experience was reported in terms of overcoming communication issues with older people and facilitating future treatment plans. However, a significant difference between the healthcare groups was found particularly in relation to continuity of use with more health educators in favor of continuing use as compared to doctors and the least being nurses. Since excessive workload of the providers has been documented as a barrier for adoption, we presume this to be the reason for lower intention to continue use among the nurses.25 On the other hand, other studies reported a similar finding among the doctors, as clinician disengagement has been often cited as a factor that impedes the adoption of health passports.18,30,35 Thus, the experience of the nurses must be carefully considered in the design and implementation of the health passport.
Broadly speaking, a statistically significant improvement in the mean total score for knowledge related to geriatric assessment, attitude, and practice was found post-implementation of health passport. An increase in knowledge has been reported in previous studies, for instance, Badran et al24 evaluated the adoption of the glaucoma patient passport in the United Kingdom using a mixed-methods study suggested the role of health passports in improving the knowledge of patients pertaining to glaucoma care. Similarly, another mixed-methods evaluation of a uveitis patient passport by Bailie et al,34 revealed an increase in knowledge related to the condition among that 93% of the participants. In contrast, no impact of a patient-held glaucoma personal record was reported by Forbes et al,36 in their single-center randomized control trial.
The improvement in attitude post-intervention may be explained in relation to the theory of reasoned action which suggests the role of behavioral beliefs such as perceived usefulness in shaping the attitude.37 Thus, we assume the overall high perceived usefulness of the passport reported by the participants particularly with regard to its utility in communicating with the healthcare team and family, planning for future health, and undergoing screening tests for detecting diseases early may have led to the increase in attitude scores. In addition, the impact on attitude may also be reasoned from the stand point of knowledge enhancement related to geriatric health that may facilitate self-management, among the participants.38 Post-intervention high practice scores may be justified on account of the improvement in knowledge regarding geriatric health and a positive attitude towards the health passport after use.39
Our findings provide useful information that can be considered in the future design and implementation of health passports by considering the perspective of diverse stakeholders including different healthcare provider groups and patients across 5 different regions in KSA.
The initial interest in the passport was promising since the results suggest that majority of the participants including patients and healthcare providers reported an overall favorable experience. The health passport tool also showed a significant improvement in older people’s health knowledge, attitudes, and practice.
Study limitations
The present study includes the possible interviewer bias in reporting since the study participants were largely illiterate. A larger sample size is preferred in order to increase the validity and generalizability of the study. Additionally, the duration of using the passport in this study was 6 months, it is better to be one year or more in order to measure the impact of the health passport on the health of the participants accurately.
In conclusion, it appears that older people health passport is potentially an effective tool to raise awareness and knowledge, enhance positive health attitudes, and improve health practices and communication between older people and health care providers.
Future research on older people’s health passport is recommended to be applied on a larger scale to other regions in KSA and should be supported to include all levels of care and not just primary health care. We further recommend the development of the electronic version of the health passport to be considered in the future to facilitate and expand its use.
Acknowledgment
The authors gratefully acknowledge all the study participants and the healthcare staff that implemented the older people health passport in all the regions involved in this study. We would like to thank iResearch for English language editing.
Appendices
- Reliability analysis of the questionnaire before using the health passport.
- Reliability analysis of the questionnaire after using the health passport.
- Reliability analysis of the questionnaire of medical staff.
Footnotes
Disclosure. This study was funded by the Ministry of Health, Riyadh, Kingdom of Saudi Arabia, as a part of the total fund provided for the Older People Healthcare Program in 2019.
- Received June 23, 2021.
- Accepted August 12, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.