


Abstract
Objectives: To validate C-reactive protein (CRP), red cell distribution width (RDW), and neutrophil lymphocyte ratio (NLR) for both serious outcomes and length of hospital stay (LOS) among hospitalized coronavirus disease-19 (COVID-19) patients.
Methods: Laboratory data of adult COVID-19 patients (n=74) was collected in this retrospective cohort. Logistic regression was employed for risk factor evaluation and receiver operating curve was used for comparison of these risk factors for the prediction of serious outcome. Multiple regression was applied to determine the association between routine analytes and LOS.
Results: Higher levels of CRP (3 times), white blood cells (20%), and neutrophil counts (40%) were seen in the serious category. Odds ratio for CRP for the serious outcome was 1.052 (p=0.007) and RDW for the serious outcome was 1.218 (p=0.040) in unadjusted model and odds ratio for CRP for the serious outcome was 1.048 (p=0.024) and for RDW 1.286 (p=0.023) in adjusted model. In a multivariate regression analysis for the LOS of the unadjusted models consisting of NLR, monocyte lymphocyte ratio (MLR) and platelet lymphocyte ratio (PLR), the beta coefficients (BC) for the CRP were 0.006 (NLR), 0.005 (MLR) and 0.006 (PLR), whereas -0.029 (NLR), -0.034 (MLR) and -0.027 (PLR) were BCs for mean corpuscular hemoglobin concentration (MCHC). Additionally, in adjusted models, the BCs for MCHC were -0.044 (NLR), -0.047 (MLR) and -0.043 (PLR). However, the CRP was consistent with 0.004 (BC) in all models.
Conclusion: We observed that CRP is a better predictor than RDW and NLR for serious outcome among COVID-19 patients. Besides, CRP was positively, whereas MCHC was negatively associated with LOS.
- Coronavirus
- COVID-19
- C-reactive protein
- mean corpuscular hemoglobin concentration
- neutrophil-lymphocyte-ratio
- red cell distribution width
So far, the novel coronavirus disease-19 (COVID-19) pandemic had taken a toll of 102 million infections and a little over 2.2 million deaths.1 Most of these deaths in COVID-19 occurred because of respiratory complications but acute kidney and cardiac injury as well as other complications including multiple organ failure were also seen as a terminal event.2 Though the average death rate worldwide is around 2.2, it is significantly higher among people who had shown critical illness (or serious outcome).3 Cytokine storm due to exaggerated immune response and inflammation-mediated injuries are the underlying reason for the serious outcome, thus increasing mortality in the disease.4 In addition to higher mortality, prolonged length of hospital stay (LOS) was also observed among patients with serious outcomes.5 Increased LOS is an additional risk factor for hospital-acquired infections and can further complicate an existing condition.6 Several independent risk factors, namely, advanced age, male gender, genetic susceptibility, comorbidities, and few laboratory parameters came up for critical illness in some recent studies.7-11
Further, acute kidney injury (AKI) frequently complicates COVID-19 infection and 24 hours change in creatinine level (delta creatinine; Δ Cr) had shown usefulness in early detection of AKI as well as short- and long-term all-cause mortality in the past.2,12 Additionally, patients with high mean corpuscular hemoglobin concentration (MCHC) levels had shown good prognosis in acute cardiac injury including acute myocardial infarction.13 Since biomarkers for cardiac injury, namely, troponins and creatine kinase MB (CK-MB) are not routinely performed on every infective patient in healthcare institutions, quantification of MCHC can have prognostic value among COVID-19 patients, especially among the patients with the acute cardiac injury.
Of late, increase levels of c-reactive protein (CRP), leucocyte ratios such as neutrophil lymphocyte ratio (NLR), and hematological parameter, red cell distribution width (RDW) were shown to have a significant association with higher mortality among COVID-19 patients.9-11 Additionally, concerning LOS, despite of a limited number of studies, lymphopenia identified as a risk factor for the prolonged LOS.5 Nevertheless, all these parameters are related to infection and inflammation and convey very little regarding acute kidney or cardiac injury. Therefore, this retrospective study was designed to verify the potential utility of CRP, RDW, and NLR levels at the time of hospital admission in the identification of serious outcomes including their comparison for predictive potential, simultaneously, among COVID-19 patients. We also intend to evaluate risk factors among the routine laboratory parameters, including various leucocyte ratios, MCHC, and Δ Cr, for serious outcome in COVID-19 patients. Moreover, any association between LOS and these parameters, individually as well as in combination, were assessed.
Methods
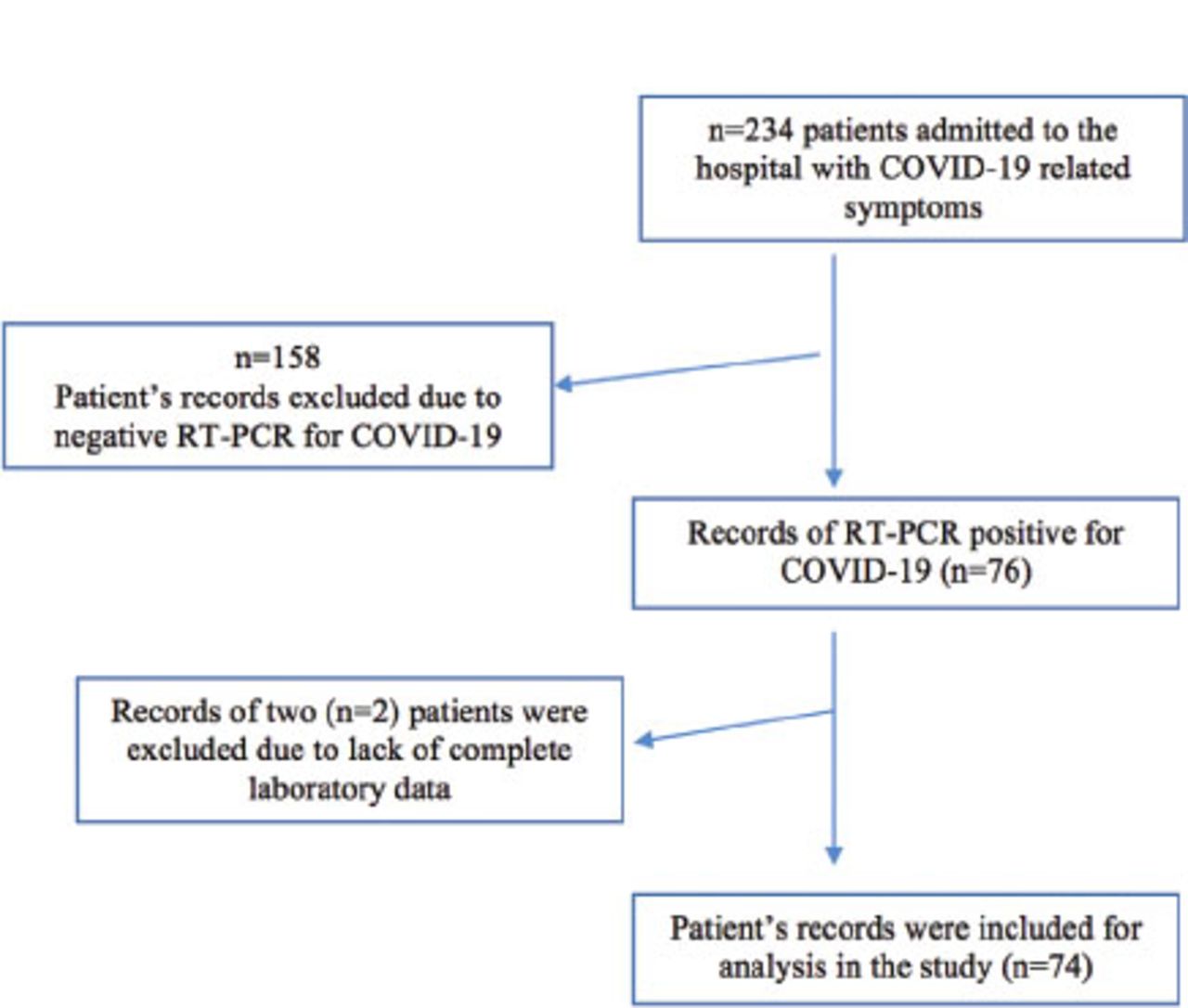
We performed a record-based historical cohort study in September 2020 in Jizan, Kingdom of Saudi Arabia (KSA). We retrieve laboratory data of COVID-19 patients from hospital’s electronic medical record systems from May to August 2020 of King Fahad Central Hospital, Jizan, KSA, following approval from the Ethics Committee (approval number: 2103). In this study, all patients were confirmed to have a positive diagnosis by real-time reverse transcriptase-polymerase chain reaction (RT-PCR) for COVID-19 infection. Data of 74 patients (39 males and 35 females), with age more than 18 years, having complete information regarding their routine laboratory investigation was collected. Laboratory results of various time points including at the time of admission, after 24 and 48 hours of admission as well as at the time of discharge/death were obtained from the system. The date of onset of the first symptom as well as the duration of hospitalization was also taken into account. Recovery was defined as patients having no symptoms of COVID-19 for at least 3 consecutive days. Any patient with any of the missing required information was excluded from the study. Patients were divided into 2 categories, namely serious (30 total; 16 males and 14 females) based on their admission in intensive care unit (ICU) and stable (44 total; 23 males and 21 females) according to their treatment in conventional care unit (isolation unit). There were 24 patients with comorbidity among stable and 9 patients with comorbidity among serious group including 4 deaths in the serious group. Biochemistry and complete blood count were carried out during their stay in the hospital using the Roche Cobas C501 and E60 for clinical and immunochemistry tests and Sysmex XN1000 for hematology tests. The following parameters were included in the study: absolute count of leucocytes (WBC), neutrophils, lymphocytes, platelets, and eosinophils, the concentration of CRP, RDW, mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), MCHC, serum creatinine (S. Cr), and hemoglobin level. The ratios were calculated (MLR, PLR and NLR) by dividing their absolute counts with lymphocytes. Delta creatinine (Δ Cr) was obtained by subtracting (Cr24 - Cr0) creatinine level at the time of admission (Cr0) from creatinine level after 24 hours of admission (Cr24). Percent delta creatinine (% Δ Cr) calculated ([Cr24 - Cr0]/Cr0) by dividing delta creatinine with creatinine level at the time of admission (Figure 1).
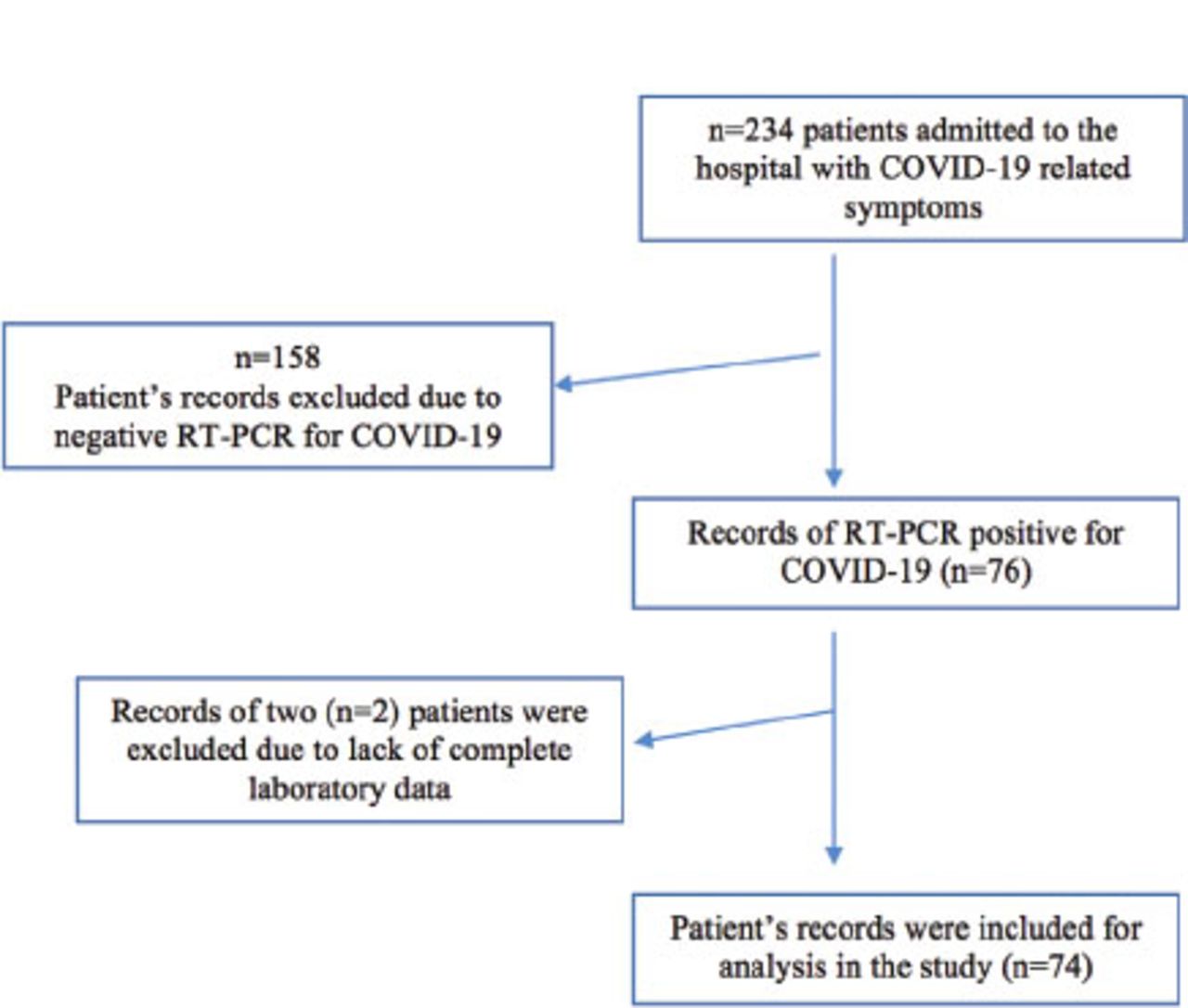
- STROBE chart. COVID-19: coronavirus disease-19, RT-PCR: real-time reverse transcriptase-polymerase chain reaction
Statistical analysis
Values expressed as either mean, standard deviation (SD), or median, range. To compare means or groups, Mann-Whitney, Chi-square, analysis of variance (ANOVA), and t-test, were employed for the differences among groups. Binary logistic regression was used for the evaluation of the risk of serious outcomes among COVID-19 subjects. Association of analytes with the LOS among COVID-19 patients was assessed by linear regression. For multivariable logistic regression analysis, unadjusted and age-, gender- and comorbidity-adjusted (AGC) models were used. In LOS multivariable analysis, models were designed with due consideration to avoid collinearity and only variance inflation factor (VIF) values between 1.0-1.3 were used for any specific analyte. Like logistic regression models, unadjusted (1A for NLR, 1B for MLR, and 1C for PLR) and AGC-adjusted (2A, 2B, and 2C) models were used in LOS multivariable analysis. The receiver operating characteristic (ROC) curve was used for area under curve (AUC) for CRP, RDW, CRP/MCHC ratio, and other parameters. Only values obtained in the ROC curve of CRP and RDW are presented in result due to similar observation and values of AUC in CRP and CRP/MCHC ratio and non-significance in other analytes. All analyses were performed using the Statistical Package for Social Sciences, Version 21 for Windows and Microsoft Excel (IBM Corp., Armonk, NY, USA). Odds ratios (OR) with their 95% confidence intervals (CI) and unstandardized beta coefficient (BC) were expressed and p-values <0.05 were considered significant.
Results
Levels of various routine laboratory analytes along with their ranges as well as mean and SD of age (50.4±17.2 years) of the patients of COVID-19 are depicted in Table 1. Higher levels of acute-phase reactants, namely, CRP, and WBC are frequently accompanied during viral infections and their level of increase usually correlate with the severity of the infection. As expected, almost 3 times higher CRP values and a 20% increase in WBC counts were observed at the time of hospital admission among serious patients when compared with stable ones with significant male gender predilection in both the groups. Likewise, higher values of RDW (13%) and neutrophils (40%) were seen among severe COVID-19 patients in comparison to stable patients. On the other hand, lymphocyte counts (20%), and hemoglobin (Hb) level (~5%) were found to be lower in serious patients. The ratios, namely, NLR, MLR, and PLR were significantly higher among male patients in serious patient group when compared with females. Additionally, higher ratios were seen among serious subjects as compared to stable one (Table 2). To recognize an association between the serious outcome of COVID-19 infection and routine laboratory parameters as well as their ratios, binary logistic regression analysis was applied as shown in Table 3. In univariate analysis, RDW with OR: 1.053 and CRP with OR: 1.252, significantly predicted serious outcome in COVID-19 patients. On the other hand, leucocyte ratios (NLR, MLR, and PLR), Δ Cr, and MCHC failed to do so. Additionally, to ascertain the possibility of the influence of these analytes in LOS among COVID-19 patients, linear regression was done. Various analytes positively predicted longer LOS, notably CRP, NLR, PLR, and MLR, while the Δ Cr and MCHC predicted negatively. In multivariable logistic regression analysis, 2 models were used namely, unadjusted and adjusted consist of CRP and RDW. In unadjusted CRP OR: 1.052 (p=0.007) and RDW OR: 1.218 (p=0.040) as well as adjusted model CRP OR: 1.048 (p=0.024) and RDW OR: 1.286 (p=0.023), as shown in Table 4, both CRP and RDW significantly predicted serious outcome with comparable potentials.
- Average age and levels of routine laboratory analytes of covid-19 patients at the time of admission (N=74).
- Levels of routine laboratory analytes, leucocyte ratios, and delta creatinine (Δ Cr) among stable and serious COVID-19 patients.
- Univariate analysis: binary logistic for serious outcome in COVID-19 infection and linear regression for length of hospital stay.
- Multivariable logistic regression for serious outcome in COVID-19 patients in adjusted and unadjusted models.
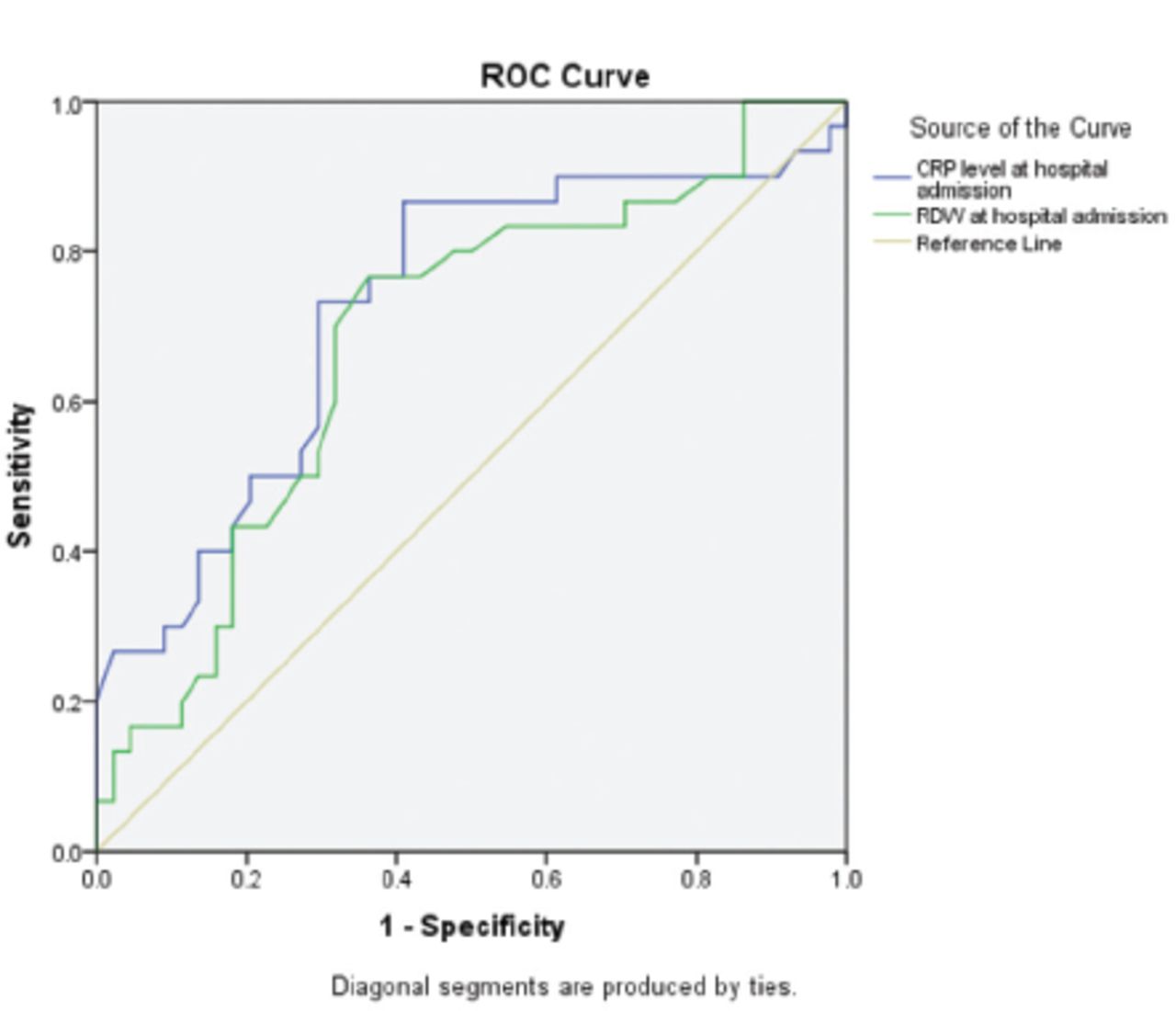
To compare the predictive potential of RDW and CRP in the serious outcomes of COVID-19 infection, ROC curve was used (Figure 2). Area under curve was similar for both CRP (OR: 0.726, range: [0.603-0.848]; p=0.001) and RDW (OR: 0.684, range: [0.559-0.809]; p=0.008) with marginally larger AUC for CRP.
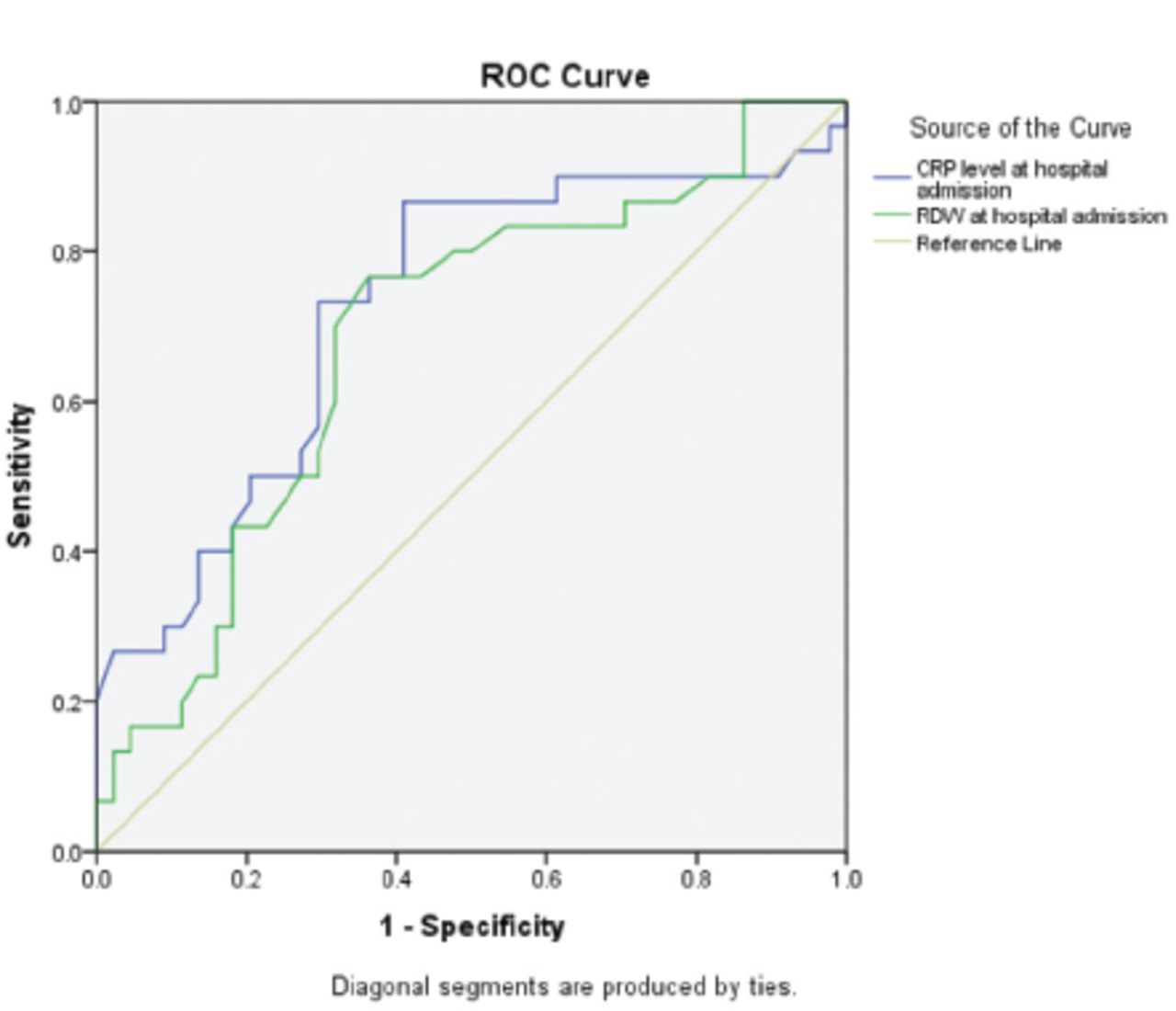
- Receiver operating characteristic (ROC) curve depicting area under curve (AUC) for c-reactive protein (CRP) and red cell distribution width (RDW). Serious outcome (intensive care unit [ICU] admission) is the dependent variable.
In multiple regression (MR) for LOS, 6 models (1A, 1B, and 1C; 2A, 2B, and 2C) were designed. The reason for giving preference to % Δ Cr over Δ Cr in making of models for MR is due to lack of absolute values in % Δ Cr. In all unadjusted models (1A, 1B, and 1C), CRP turns out to be the strongest positive predictor, whereas % Δ Cr and MCHC remained negative predictor, significantly. However, in the adjusted models (2A, 2B and 2C), NLR and PLR become non-significant. In addition, CRP (BC: 0.004 in all models, p=0.003 in 2A and 2C, whereas in 2B it is p=0.004) continued to be the positive predictor of LOS. Further, the BC for MCHC (-0.044 [2A; p=0.007], -0.047 [2B; p=0.003] and -0.043 [2C; p=0.009]) remained as a negative predictor for LOS. In addition, % Δ Cr shows negative associative with LOS only in model 2B (MLR; Table 5).
- Multiple regression analysis for length of hospital stay (LOS) in various unadjusted and adjusted models.
Discussion
A wide range of research has proven predictive potentials of routinely analyzed laboratory biomarkers in disparate clinical setup. High NLR was observed as an independent predictor of risk stratification and post discharge mortality in acute coronary syndrome.14,15 Similarly, in a cohort of intracerebral hemorrhage (ICH), high NLR predict neurological deterioration within 7 days of ICH better than total WBC counts or absolute neutrophil counts.16 Additionally, NLR calculated at the time of admission predicted symptomatic hemorrhagic transformation, a life-threatening condition, in patients of acute ischemic stroke.17 Likewise, CRP measured at the time of hospital admission and after 72 hours can predict short- and long-term complication following cerebral hemorrhage.18 Higher PLR, a marker of atherosclerotic inflammation, met with adverse outcome and death in acute ischemic stroke following intravenous thrombolysis.19 Both lymphocytopenia and NLR had shown better predictive value for bacteremia in emergency care than WBC count or CRP.20
We investigated the association of routine laboratory parameters with serious outcome and LOS among COVID-19 patients. This study not only provides a comprehensive analysis of predictive values of routine laboratory tests but also offer validation of previously reported risk factors for a serious consequence in the disease. In addition, by discerning any association between these common analytes and LOS, this study had shown another dimension for the putative utility of simple and common analytes in the prior prediction of LOS and associated cost to healthcare institutions. In our study, a total of 74 COVID-19 patients were included, of these 74, 44 (59.5%) patients were mild to moderate with stable conditions, whereas 30 (40.5%) were with the serious outcome. Some of the findings in this retrospective study conform to previous reports. Particularly, high values of neutrophil count, WBC count, RDW, CRP, NLR, PLR, MLR and low lymphocyte count were seen among serious patients.2,9,11,21-23
Several researchers reported high NLR, RDW, and CRP levels as a risk factor for the serious outcome or low survival rate in COVID-19 infections.5,9-11,21 Comparably, we came across similar findings in our study that higher CRP, as well as RDW level at the time of hospital admission, is significantly associated with an increased serious outcome among COVID-19 patients. Interestingly, contrary to the previous reports, we failed to observe any significant association between higher NLR with the serious outcome.11,24 It could be due to 2 reasons, firstly, most of the previous studies were intended to find out the association between mortality and NLR, however, some had looked for the serious outcome and not survival.11,24 Secondly, the decrease in lymphocytes, resulting in a rise of NLR, is a late phenomenon or at least a rise in CRP happens to be chronologically early in the disease.25,26 The later point is supported in our study where NLR calculated after 48 hours of admission was significantly associated with serious outcome (NLR48, OR: 1.107, range: [1.015-1.208], p=0.022); CRP48, OR: 1.025, range: [1.002-1.049], p=0.034) in univariate analysis, though no significant relationship was observed in multivariable analysis. Further, after age, gender, and comorbidity adjustment to minimize the potential confounding impact of these variables in multivariable logistic regression, the OR for CRP and RDW remained significant with a slight increase of 5% in RDW and no change in CRP. Moreover, the comparison of predictive values of CRP and NLR, as well as NLR and RDW, were reported in 2 independent studies. However, any such comparison of RDW and CRP is lacking.22,24 Additionally, both studies had detected NLR as a better predictor than either CRP or RDW. On the contrary, our study had provided evidence that CRP level can predict the serious outcome at least 48 hours before NLR, especially at a time when NLR failed to provide any valuable information. Additionally, recently, Xu et al,27 had mentioned CRP as a better predictor than NLR for mortality in COVID-19 infection. Therefore, we had performed such a comparison by employing ROC curve to compare RDW and CRP in the prediction of serious outcome in COVID-19 infection. C-reactive protein come up with p=0.726 AUC and RDW come up with p=0.684 AUC, thus CRP turns out to be a better predictor than RDW. However, the difference is subtle. Taken together, these findings confirm the higher predictive efficiency of CRP over both RDW and NLR.
We found similar, to previously reported, finding concerning prolonged LOS in our study with a higher average duration of stay among patients with a serious outcome (20.77±13.0 days), as compared to a stable one (14.93±12.43 days).5 In multivariate analysis for risk factor identification for LOS, CRP remained as the most significant positive predictor following AGC adjustment. On the other hand, MCHC turn out to be the most significant negative predictor in AGC-adjusted models. Our finding, association of higher CRP levels and prolonged LOS, contradicts with prior report, where the authors identified lymphopenia, but not CRP level as a predictor for lengthening of hospital stay.5 The authors did not mention that CRP levels and lymphopenia, considered for analysis, were measured at what time point of the patient’s hospital stay. As mentioned above, the rise in CRP is an earlier event than lymphopenia. The disagreement might be due to the lymphocyte counts and CRP values recorded at a later point of time than our study.25
The association between MCHC and LOS is a novel finding in this study. Previously, high MCHC levels had shown to have a better outcome in acute coronary events but any such association is obscure in COVID-19 infection.13,28 Nevertheless, Pan et al,29 had quantified MCHC levels in COVID-19 as well as community-acquired pneumonia among hospitalized patients and observed higher levels of MCHC among the former group. On the other hand, in our case the relationship was determined between serious and stable patients, and interestingly, we noticed similar values in both the groups with an insignificantly lower (5%) Hb levels in serious patients. Recently, 2 separate studies demonstrated structural damage and morphological alteration of erythrocytes in serious COVID-19 patients.30,31 However, further studies are needed to identify the diagnostic or prognostic utility of MCHC in COVID-19.
The most important finding in our study is that higher levels of CRP is a significant predictor for a prolonged stay in the hospital as well as a serious outcome among COVID-19 patients. C-reactive protein is a known acute-phase reactant and has a crucial role in the clearance of the infection by influencing various mechanisms notably enhanced phagocytosis and complement system activation. Moreover, previously, CRP levels were correlated with the extent of renal and cardiac injuries.32,33 Similarly, Wang,10 had observed a significant positive correlation between early CRP level in COVID-19 patients and their lung lesions. Consequently, risk stratification for potentially serious cases at the time of hospital admission by measuring CRP levels, a simple routine laboratory test, provides an opportunity for aggressive intervention in due time and may save many lives.
Study limitations
Though we had provided sufficient evidence to support our conclusion, it is a single-center study including patients of Arab ethnicity only. Due to the nature of the study, namely, retrospective, we were unable to unravel the mechanism of association between MCHC and LOS. The data included in this study is taken from hospitalized patients only; however, most COVID-19 patients have advised of home isolation due to their trivial illness.
In conclusion, we observed that routine laboratory parameters can be of prognostic significance in COVID-19, especially for serious outcome and LOS. We report high CRP levels as an independent risk factor for both serious outcome as well as a prolonged hospital stay. Furthermore, MCHC turns out to be a negative predictor for the LOS.
Acknowledgment
The authors gratefully acknowledge scribendi (www.scribendi.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 31, 2021.
- Accepted September 1, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.