


Abstract
Objectives: To assess the presence of vitamin B12 deficiency among metformin users and associated factors in patients with type 2 diabetes mellitus.
Methods: An observational cross-sectional study was conducted with 307 diabetic patients in the primary health care centers at King Abdulaziz Medical City (KAMC), Riyadh, Saudi Arabia between October 2017 and January 2018. Face-to-face interviews were conducted with the participants, using a designed checklist.
Results: The prevalence of vitamin B12 deficiency was (3.6%) and the majority of the sample had borderline B12 levels (66.1%). The vitamin B12 deficiency and borderline levels were strongly associated with the dose of metformin. Patients taking doses of metformin more than 1000 mg had lower levels of vitamin B12. The use of multivitamin and vitamin B complex was assessed, and it was found that there was a marked decrease in the prevalence of vitamin B12 deficiency in patients using vitamin B complex containing more than 200 mcg vitamin B12.
Conclusion: Our findings show a low prevalence of vitamin B12 deficiency in type 2 diabetic patients taking metformin. The majority of the sample had borderline deficiency; therefore, additional investigation and management are required.
Diabetes mellitus (DM) is a widely prevalent disease managed in primary health care, and its prevalence has increased significantly in the past decade.1 It is considered a serious public health concern due to the multiple comorbidities and complications, including retinopathy, nephropathy, peripheral neuropathy, cardiovascular diseases, and the necessity for lifelong management.2 According to the American Diabetes Association (ADA), metformin is the initial drug of choice and the cornerstone for the control of type 2 diabetes due to its high efficacy in controlling macro-vascular complications.3 However, when used for prolonged periods, it may cause biochemical side effects such as vitamin B12 deficiency.4
Several international studies have assessed vitamin B12 deficiency among type 2 diabetic patients using metformin. The prevalence of metabolically confirmed B12 deficiency in type 2 diabetic population on metformin was between 4% and 41%.5,6 However, there is considerable variation in the studies regarding the factors influencing this association. In a 2017 study conducted in Peshawar, Pakistan, it was found that the use of multivitamins and vitamin B12 supplement could be protective against developing vitamin B12 deficiency.7 Another study from Lahore, Pakistan, conducted in 2019, reported that longer duration (more than 2 years) of metformin use was strongly associated with vitamin B12 deficiency.8
In Saudi Arabia and the Middle East, there are large number of cases of diabetes and its associated complications, but there is limited research regarding vitamin B12 deficiency related to the use of metformin. The aim of this study is to assess the presence of vitamin B12 deficiency among metformin users in patients with type 2 diabetes mellitus. The sample of patients were drawn from the primary health care centers at King Abdulaziz Medical City (KAMC), Riyadh, Saudi Arabia. The study also attempts to analyze the effect of supplementation on B12 levels.
Methods
From October 2017 to January 2018, a cross-sectional study was undertaken with type 2 diabetic patients at KAMC primary health care centers in Riyadh. Face-to-face interviews were conducted using a designed checklist to collect demographic data, patient condition, medication, diet, glycated hemoglobin, and vitamin B12 level. The inclusion criteria for this study were: participant had to be a type 2 diabetic patient between the ages of 18 and 80 years; taking an oral anti-diabetic medication, including metformin, for more than 3 months; and attending a KAMC primary health care center in Riyadh. The exclusion criteria included type 1 diabetic patients; patients on an insulin-only regimen; those having a chronic kidney disease defined by a creatinine level >3.0 mg/dl; patients suffering from chronic liver disease, Crohn’s disease, and thyroid disease; patients who had undergone gastric or bariatric surgery or ileum resection; pregnant women, severely ill patients who were unable to give consent, and mentally ill patients.
A convenience sampling method was used in this study. Patients with type 2 diabetes were notified about the study, and an informed consent was obtained from them. The sampling was carried out 3 days per week, and 5 to 7 patients were interviewed during a regular scheduled visit to the outpatient clinic. A blood sample was taken from each patient to measure the level of vitamin B12 and HbA1c within a month of the interview. There is multiple blood test usually used to aid the diagnosis of vitamin B12 deficiency are homocysteine, serum vitamin B12, and plasma methylmalonic acid.9 As these tests are not gold standard tests, it is difficult to establish a clear cutoff point as a diagnostic value. Serum cobalamin is the most frequently used test and considered the initial investigation for vitamin B12 deficiency. The serum vitamin B12 was measured using the ARCHITECT B12 assay. The reference value indicating vitamin B12 deficiency was <150 pg/mL, a value between 150 and 399 pg/mL was considered for borderline deficiency, and a value above 400 pg/mL was considered normal.9 The checklist for the interviews was designed and developed by the researcher after an extensive literature review. The checklist was validated by 2 family medicine consultants and translation validity was ensured using the forward and backward translation from English to Arabic.
Participants were included after written informed consent. The study and the informed consent form were approved by the Institutional Review Board (IRB) of King Abdullah International Medical Research Center (KAIMRC) according to the principles of Helsinki Declaration.
Data management and analysis plan
The data were analyzed using the Statistical Package for Social Sciences program, version 23 (IBM Corp., Armonk, N.Y., USA). The categorical variables are expressed in frequency and percentage. A Chi-square was used to assess differences between the categorical variables. Continuous variables were expressed with a mean and standard division. A p<0.05 was considered statistically significant.
Results
Three hundred and seven patients were enrolled in the study. The age of the patients ranged from 20 to 79 years, with a mean of 58.69±11.1 years. The majority (n=191; 62.2%) were females and 169 (55%) had been diagnosed with type 2 diabetes for less than 10 years while 138 (45%) had been diabetic for more than 10 years. In the majority (60.9%) of cases, the diabetes was uncontrolled with a mean of 8.5±1.68. Approximately 187 (60.9%) were using ≥1000 mg of metformin and 120 (39%) <1000 mg of metformin. The mean duration of metformin use was 9.53±5.853 years. The vast majority were nonsmokers (93.2%) and nonalcoholics (99.7%) and none were vegetarians (Table 1).
- Characteristics and demographic data of diabetic patients on metformin (N=307).
- Association between vitamin B12 levels and use of a supplement (N=307).
Eleven (3.6%) was vitamin B12 deficient (<150 pg/mL), and 203 (66.1%) had borderline deficiency (150-399 pg/mL). Approximately 93 of the samples (30.3%) had normal vitamin B12 levels (≥400 pg/mL). Only 11.4% of the patients were taking multivitamins, and many of these patients (41.2%) had been taking it for more than 2 years. More than half (62.2%) were taking a vitamin B supplement, and 46.4% were taking it for more than 2 years.
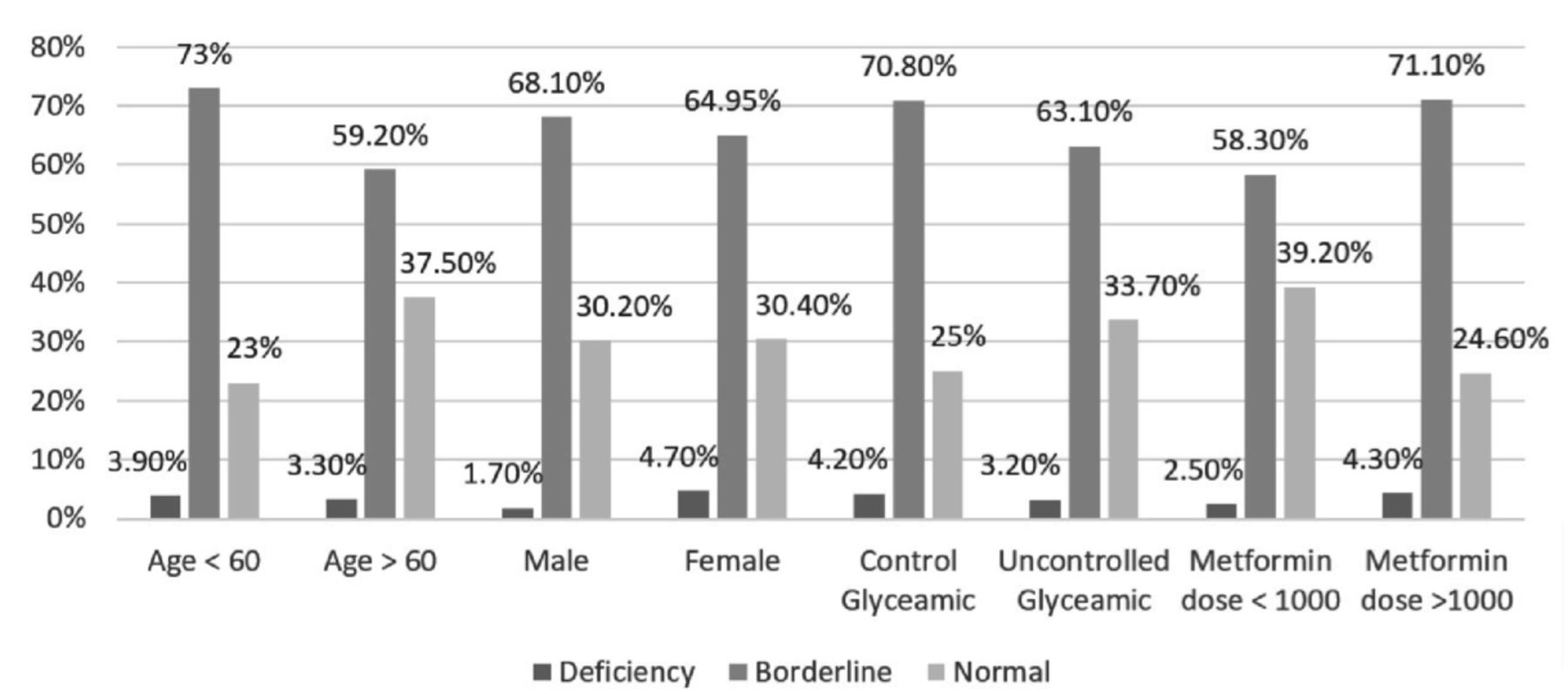
As shown in Figure 1, the group that was taking >1000 mg metformin had higher proportions of vitamin B12 borderline (71%) and deficiency levels (4.3%), compared to 58.3% and 2.5% in the group taking <1000 mg metformin, which was statistically significant (p=0.023). Higher levels of vitamin B12 deficiency occurred in the group <60 years (n=6; 3.9%) compared to ≥60 years and older (n=5; 3.3%). However, the borderline deficiency was higher in the group 60 years and older (n=111; 73%), which was statistically significant (p=0.011).

- Relation between patient’s characteristics and vitamin B12 levels.
The reference value indicating vitamin B12 deficiency was <150 pg/mL, a value between 150 and 399 pg/mL was considered for borderline deficiency, and a value of above 400 pg/mL was considered normal.
For the group that was taking both metformin and vitamin B complex, almost half (45%) had normal vitamin B12 levels, 45.1% borderline levels, and 0.9% were deficient. The association was statistically significant (p=0.0).
Discussion
In the current study, the prevalence of vitamin B12 deficiency in diabetic patients taking metformin was 3.6%. This finding is similar to two studies carried out in Pakistan and Saudi Arabia, at 4% and 9.4%, respectively.5,10 However, this study is in contrast to a study conducted in South South Nigeria, where the prevalence was 40%.6 Possible reasons for the variations in vitamin B12 levels globally are the cutoff levels used in the studies, diverse cultural and religious beliefs, as well as dietary habits, which play a significant role in vitamin B12 levels. The majority (66.1%) of the sample in this study had borderline B12 levels. This is higher than what was reported (59%) by the study in South South Nigeria.6 Patients with borderline deficiency need additional evaluation to identify the group who are vitamin B12 deficient. The use of homocysteine and methylmalonic acid tests can increase the sensitivity of vitamin B12 deficiency detection;11 however, the tests were not available at our facility.
The vitamin B12 deficiency and borderline levels were not affected by the duration of metformin use but were strongly associated with the dose of metformin. Patients taking higher doses of metformin, >1000 mg, had lower levels of vitamin B12. These results are consistent with several studies where the metformin dose was the strongest predicator of vitamin B12 deficiency, as each increase in metformin dose increases the risk of vitamin B12 deficiency.10,12
The use of any supplement containing vitamin B12 was also assessed in this study, and a marked decrease was noted in the prevalence of vitamin B12 deficiency in patients using vitamin B complex with >200 mcg vitamin B12. However, a multivitamin with 6 mcg vitamin B12 did not change the prevalence of borderline or full-fledged vitamin B12 deficiencies. Moreover, some studies reported that using any dose of vitamin B12 supplement will improve the vitamin B12 levels.7,13,14
In addition, the current study did not find a correlation between diabetes control and vitamin B12 deficiency, using the HbA1c levels as the predictor of diabetes control. The same result has been reported in existing literature, and this could be because the effect on the vitamin B12 levels is due to the metformin and not the diabetes itself.5,10
An assessment of the risk factors that may affect vitamin B12 levels showed that the deficiency occurred less in older patients. The reason could be the use of supplements by older patients, compared to younger diabetic patients. In addition, no gender difference was noticed in the study, which is similar to study from Bangladesh.15
Study limitations
First, our study was confined to patients from a single hospital at KAMC in Riyadh, and specifically to the primary health care centers, which make it difficult to generalize the results on Saudi Arabia as a whole. Another limitation of our study is that we used cross-sectional study, and it may not be the best way to establish a causal relationship between vitamin B12 levels and patient factors. Third, homocysteine and methylmalonic acid tests, which play an important role in proper identification of patients with true vitamin B12 deficiency, were not performed in this study for patients who exhibited borderline deficiency.
In conclusion, the prevalence of vitamin B12 deficiency in diabetic patients on metformin found to be low in this study. The majority of patients had borderline B12 deficiency, necessitating further investigation and management. The metformin dose was the strongest factor contributing to this deficiency, and it was seen that taking a vitamin B12 supplements prevents the development of vitamin B12 deficiency. Further studies are required to assess vitamin B12 levels in relation to metformin to represent the entire Saudi Arabia population and measure serum homocysteine and methylmalonic acid levels along with vitamin B12 level for better diagnosis and management.
Acknowledgment
We would to like to thank (Scribendi) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 11, 2020.
- Accepted December 30, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.