


Abstract
Objectives: To measure the Saudi population’s sleep quality during the lockdown of COVID-19.
Methods: An internet-based questionnaire that was performed during the lockdown of the COVID-19 pandemic among the Saudi population over 2 weeks from April 1 to April 15, 2020. We used the instant messaging application WhatsApp and Twitter to reach the targeted population. Saudi citizens and non-Saudi residents who can read and understand the questionnaire were recruited. Data were analyzed using Stata and SPSS.
Results: A total of 790 responses were included. The majority of participants were the Saudi population 735 (92.9%). The prevalence of insomnia and poor sleep quality were 54.4% and 55.5%, respectively. Saudi citizenship was associated with longer sleep duration (p=0.031). Female gender and being married were associated with worse global PSQI, sleep quality, sleep distribution, sleep latency, and daytime dysfunction.
Conclusion: Our findings showed that during the COVID-19 pandemic, the Saudi population had a high prevalence of insomnia and poor sleep quality. Routine monitoring of the psychological impact of life-threatening outbreaks and the adoption of effective early mental health actions should be considered.
In December 2019, the world witnessed the first case of Coronavirus disease 2019 (COVID-19), which began to spread rapidly through Wuhan, Hubei Province, and other provinces in China, then the rest of the world.1-3 Four months later, Saudi Arabia’s government had announced the first case of the COVID-19.4 The Saudi government has undertaken many notable measures to limit the outbreak, including forming a high-level committee incorporating prominent government institutions, the halt of the issuance of tourist visas for all purposes, the immediate suspension of domestic and international air travel.5 Besides, the government has imposed a 2-week quarantine period for returning travelers from countries with high infection rates, banned mass gatherings for all purposes, enforced complete or partial lockdowns in different areas, closed and disinfected the 2 holy mosques, and increased public awareness and education.6 These measures are expected to impact the psyche of the Saudi population negatively. Outbreaks are well known to affect human psychological well-being significantly.7 Therefore, many cases of depression, anxiety, panic attacks, sleep disorders, and posttraumatic stress disorder symptoms have been observed during and after serious outbreaks and pandemics, such as COVID-19.8
Sleep disorders or inadequate sleep contribute to epileptic seizures, depression, accidents, heart disease, diabetes, and poor life quality.9 Therefore, many studies have paid great attention to sleep and sleep disorders during the COVID-19 outbreak.10-13 Huang and Zhao assessed sleep quality in china (n=603) using the Pittsburgh Sleep Quality Index (PSQI) and showed that during the lockdown, the Chinese population had suffered from poor sleep quality.14 Furthermore, Yu et al15 showed that most of the Hong Kong population reported that their sleep had deteriorated following the outbreak of COVID-19. Despite the aforementioned evidence, data regarding the association between the COVID-19 lockdown and the sleep disorders of Meddle East countries’ general population, especially Saudi Arabia, are scanty. Thus, our study aimed to assess sleep quality among the Saudi population during the COVID-19 pandemic.
Methods
This was a cross-sectional, internet-based questionnaire that was performed according to the Helsinki Declaration principles and was conducted among the Saudi population during the lockdown of COVID-19. The STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) checklist was followed during reporting this study.16 The survey was carried out in Saudi Arabia over 2 weeks, from April 1, 2020, to April 15, 2020. During the data collection period, the Saudi Government had taken a number of strict measures to overcome the COVID-19 transmission, including imposing a full lockdown.17-19 Saudi citizens and non-Saudi residents who can read and understand the questionnaire were recruited using convenience sampling. We have used WhatsApp and Twitter instant messaging to reach our target population.
Sample size calculation
We have used G*Power 3.1 software to estimate the sample size based on the estimated insomnia prevalence (17%), and a 3% error margin was applied. In the 95% confidence interval, an estimated sample of 492 was suggested. A total of 790 respondents returned their responses to the internet-based questionnaire over the 2-week period of the study. Before participating in the study, all participants gave their written informed consent.
We collected the following data from the included participants: i(The Pittsburgh Sleep Quality Index (PSQI): The PSQI is an important method for measuring sleep quality and sleep habits in older adults. By measuring 7 domains, it differentiates between ” and “good” sleep: daytime dysfunction, sleep medication usage, sleep disturbances, habitual sleep efficiency, sleep duration, sleep latency, and sleep quality over the last month.20 All 7 domains can range between 0 and 3. The global score can range from 0 to 21, with a cutoff point of 5, which means that a global score of 5 or more indicates poor sleep quality. This study used the validated and translated version (Arabic) developed by Suleiman et al.21 ii) Athens Sleep Questionnaire (ASQ): We used the Arabic version of ASQ, which was validated previously. The questionnaire consists of 8 questions about the following parameters: 1) Sleepiness during the day; 2) Functioning (physical and mental} during the day; 3) Sense of well-being during the day; 4) Overall quality of sleep; 5) Total sleep duration; 6) Sleep induction; 7) Awakenings during the night; 8) Final awakening earlier than desired. Each question is evaluated with 4 scores from 0 to 3, where 0 means good/satisfactory or no problems, and 3 means serious problem or very unsatisfactory. This score’s cutoff point is 6; patients who have more than 6 are considered to have clinical insomnia.
Statistical analysis
Responses were collected using an online Google form. To analyze the data, we used the Statistical Package of Social Science (SPSS) for Windows, version 22 (IBM Corp., Armonk, N.Y., USA) and Stata 14.0. To summarize respondents’ demographic data, descriptive statistics presented as mean and standard deviation (SD), or number and percentage (%) were used. In accordance with clinically prescribed cutoff points, the respondents’ PSQI and ASQ scores were coded into binary data. Mann-Whitney and Kruskal-Wallis tests were used to compare the means of independent groups. In order to examine the relation between PSQI and ASQ scores and demographic features, a Chi-square test was used. Odds ratio (OR) of the binary logistic regression was applied to assess sleep quality correlations with a 95% confidence intervals (95% CI). If less than 0.05, the p-value was considered significant.
Results
A total of 790 responses were included. The majority of participants were the Saudi population (n=735; 92.9%). Two-thirds of the participants were employed. A total of 27.5% were healthcare workers, 45.1% were enterprise or institution workers, and 27.5% were teachers or students. The characteristics of the included participants are summarized in Table 1.
PSQI.
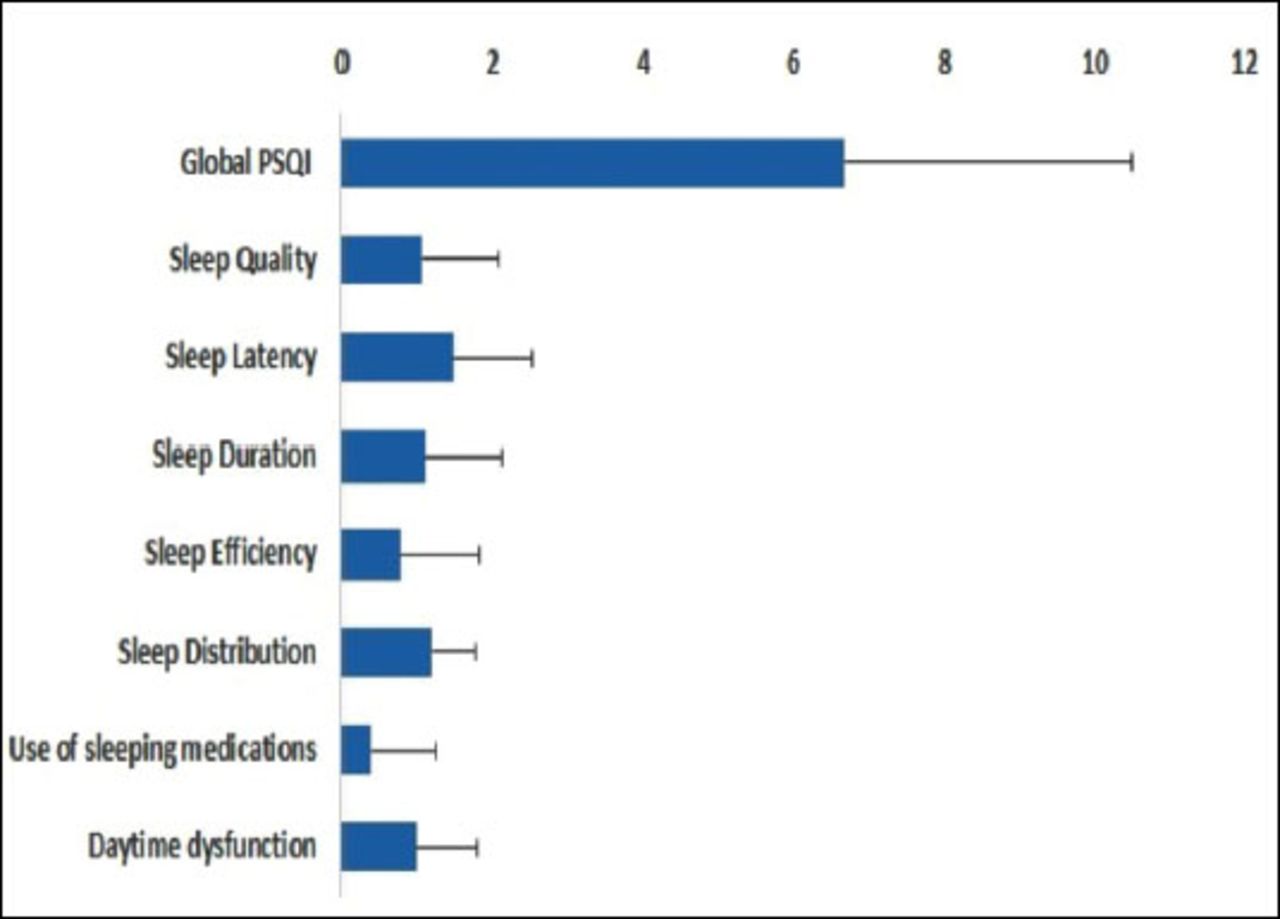
The overall Global PSQI was 6.67±3.82 for all participants; 350 (44.4%) had good sleep quality, and 438 (55.5%) had poor sleep quality. Two patients were excluded from the analysis of PSQI, as they did not report full information in terms of the sleep parameters. Figure 1 shows the mean value of sleep parameters, including sleep, latency, duration, efficiency, distribution, use of sleeping medications, and daytime dysfunction.

- Pittsburgh sleep quality index score in Saudi population.
Association of demographic characteristics and PSQI
The association between demographic characteristics and PSQI is shown in Table 2. Our analysis demonstrated that female gender was correlated with worse global PSQI (p=0.004), sleep quality (p=0.004), sleep latency (p<0.001), sleep efficiency (p=0.012), sleep distribution (p<0.001), and daytime dysfunction (p<0.001). In terms of sleep duration, the male gender was worse than the female gender (p<0.001). Single participants were associated with significant (p<0.001) better global PSQI, sleep quality, shorter sleep latency, and less daytime dysfunction than married participants. Saudi participants were associated with better sleep duration compared to the non-Saudi population (p=0.031). In terms of employment status, non-employees were associated with worse sleep efficiency (p=0.034). Participants with primary education were associated with worse sleep efficiency compared to secondary education (p=0.019) and university education (p=0.004). Our analysis showed no significant difference between participants with/ without insomnia and PSQI.
- Demographic characteristics.
Logistic regression
Table 3 presents the main findings of the logistic regression analysis. Marital status can be used as an independent predictor of poor sleep quality.
Athens sleep questionnaire (ASQ)
The prevalence of insomnia was 430 (54.4%). Compared to non-Saudi participants, Saudi participants were linked to a greater prevalence of insomnia (45.5% versus 55%), with no significant difference (p=0.172). There was no considerable relationship between insomnia and participants’ age (p=0.800), gender (p=0.947), education (p=0.827), and employment (p=0.692). Regarding marital status, the prevalence of insomnia was 61.3% in the single participants and 50.4% in the married participants. Moreover, our analysis failed to find any significant correlation between insomnia and the parameters of PSQI, as presented in Table 4.
Discussion.
Our study investigated the association between the COVID-19 lockdown and the sleep quality of the Saudi population. Our findings showed that about 55.5% of the included participants had poor sleep quality. Moreover, we observed that females and married participants were associated with worse global PSQI, daytime dysfunction, sleep quality, sleep distribution, and sleep latency. However, the prevalence of overall poor sleep and insomnia was lower in married participants compared to others, indicating that they have less prevalence with worse scores. Furthermore, employment status and education level were linked with poor sleep quality.
- Association of demographic, clinical characteristics, insomnia (ASQ), and Pittsburgh Sleep Quality Index (PSQI).
- Logistic regression of poor sleep quality.
Huang and Zhao reported a much lower prevalence of poor sleep quality (18.2%) in 7,236 self-selected Chinese volunteers.14 They assessed the sleep quality using the same questionnaire used in this study (PSQI); however, they used a higher cutoff point (>7), leading to underestimation of the sleep quality of their population. This study used (>5) as a cutoff point to differentiate between poor and good sleep quality. This cutoff point (>5) was tested by Buysse et al,22 who developed the PSQI questionnaire, and it showed 89.6% sensitivity and 86.5% specificity in differentiation between good and poor sleepers. Huang and Zhao had no substantial connection between the quality of sleep and the participants’ age (p=0.446), which was confirmed by our findings.14 On the other hand, they found that the Healthcare workers are the only group who had a significant positive regression (OR 1.48, 95% CI: 1.15, 1.95) with sleep quality. They estimated that in healthcare workers, the prevalence of sleep problems was about 25%, which could be attributed to the longer working period, making them more vulnerable to psychological distress. This difference between our and their findings can be attributed to the study time; their study was performed in early February, where the COVID-19 was at the peak in China, leading to a substantial burden on the healthcare workers.
- Association between demographic and clinical characteristics and Insomnia (ASQ).
In Italy, Marelli et al23 conducted a cross-sectional study to determine the COVID-19 lockdown effect on university students and administration staff. They demonstrated that 73.3% and 60.2% of the university students and administration staff had poor sleep quality, respectively. In agreement with our study, they showed that the impact was greater in females than in males (p=0.001). Therefore, they recommended that health authorities should offer psychological supports to females and students. It was reported that sleep habits have changed during lockdowns because of social isolation and changes in social rhythms such as work-and daily work.24 In young people (namely, students), social isolation can lead to a growing number of anxious and depressing symptoms in the presence of loneliness, vulnerability, and emergency worry. According to Huang and Zhao, these issues’ potential cause might be related to the “hypochondriac concerns.” They feared the outbreak would be difficult to contain.14 A recent systematic review showed that healthcare workers and female gender were at an elevated risk of depression, anxiety, poor sleep quality, and psychological distress.25 Regarding insomnia, our study demonstrated an increased prevalence of insomnia (54.4%) among the general Saudi population. However, we could not identify the associations of this high prevalence. In China, Li et al,26 reported an increased prevalence of insomnia 33.7%. They suggested that insomnia may be associated with economic-related stress, social distance restrictions, travel restrictions, daily life changes, mental illness, and female gender. In our study, we could not find any significant difference between both genders in terms of insomnia. In the Greek population, Voitsidis et al reported a 37.6% prevalence of insomnia, assessed by the AIS. Moreover, they showed that insomnia was more prominent in females and people in urban areas.27 Similar to our findings, Idrissi et al28 demonstrated that the Moroccan population was associated with a high prevalence of daytime sleepiness (9.9%) and insomnia (56%). The COVID-19 pandemic was accompanied by a high risk of infection, fears of infection, insufficient supplies, financial loss, inadequate information, excess information from mass media, negative emotional patients, and lack of communication with their families.29,30 They also supported the findings of Voitsidis et al regarding the increased prevalence of insomnia in females and people in urban areas.27
In Bahrain, Jahrami et al31 reported that 75% of the frontline healthcare workers were poor sleepers. In non-frontline healthcare workers, 76% were also poor sleepers. They also found that the female gender is an independent predictor of poor sleep quality. A recent study in Saudi Arabia by Al-Musharaf32 aimed to assess the pandemic’s impact on a group of healthy young Saudi females. She reported different parameters such as emotional eating scale, anxiety, depression, and preserved stress scale. She also reported that the overall PSQI score for the entire population was significantly impacted by stress, anxiety, and depression; however, she did not report the mean value of the score or the prevalence of sleep quality.32 Alnofaiey et al33 highlighted that the prevalence of sleep disorders in Saudi doctors was 43.9%, with a higher prevalence in doctors with 31-40 years.
The current study has some weaknesses.
First, the cross-sectional design hindered our ability to create any causal inferences. Second, we could not perform an interview-based questionnaire that reduces the over or under-estimation resulting from self-reporting; however, we used an internet-based questionnaire approach to prevent potential infections due to the outbreak. Third, we could not assess participants’ sleep quality before the disease due to the outbreak’s unanticipated occurrence.
In conclusion, we highlighted the substantial deterioration in the Saudis’ sleep health during the COVID-19 outbreak. The prevalence of insomnia and overall poor sleep was lower in married participants, compared to others. However, the PSQI score showed that, despite the lower prevalence, they have the worse scores in terms of global PSQI, sleep quality, sleep distribution, sleep latency, and daytime dysfunction. Any change in sleep quality may affect individuals’ mood and productivity; consequently, contentious monitoring of the psychological effects of life-threatening outbreaks and the implementation of appropriate early mental health measures should become routine. Future research should focus on the direct causal relationship between the COVID-19 pandemic and sleep disorders after considering the independent predictors that may influence this relationship.
Acknowledgment.
Authors would like to thank SevoClin CRO (www.sevoclin.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. Adel S. Alharbi is a member of the Editorial Team, and was therefore excluded from any final editorial decisions regarding this paper.
- Received November 17, 2020.
- Accepted March 11, 2021.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Prevalence of sleep problems and habits among children in Saudi Arabia: A cross-sectional study
- Sleep quality, daytime sleepiness, and insomnia in patient with epilepsy: A single center experience from Saudi Arabia
- Effects of the COVID-19 pandemic on sleep health among Middle Eastern and North African (MENA) populations: a systematic review of the literature