


Article Figures & Data
Figures
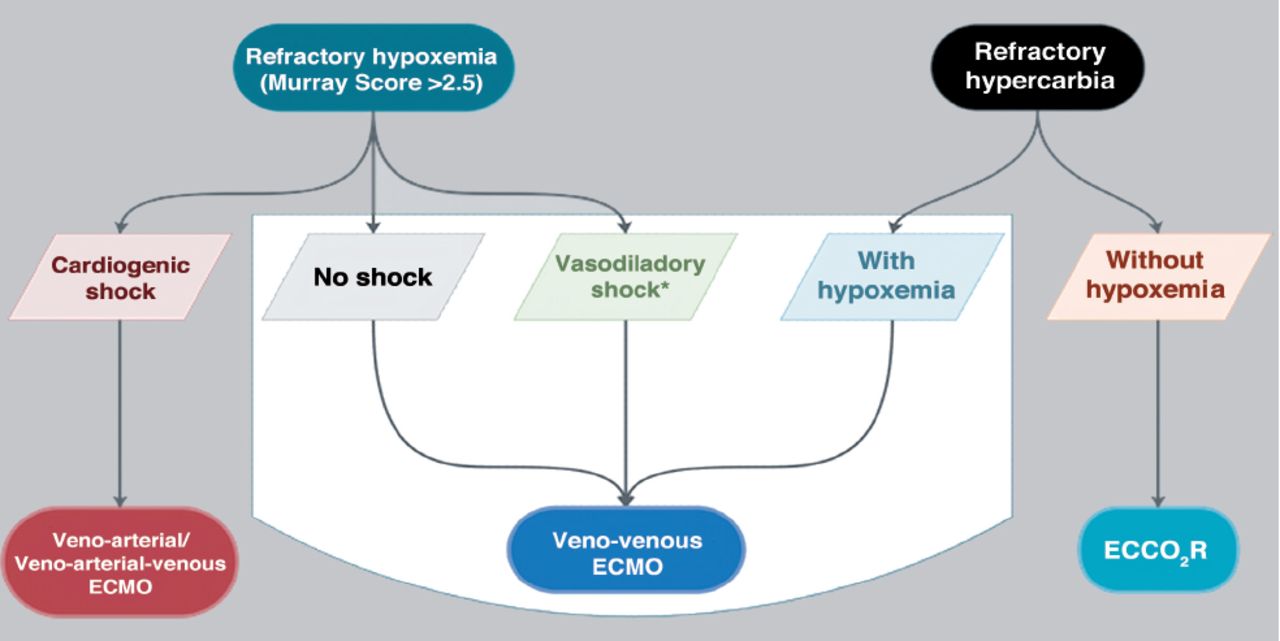
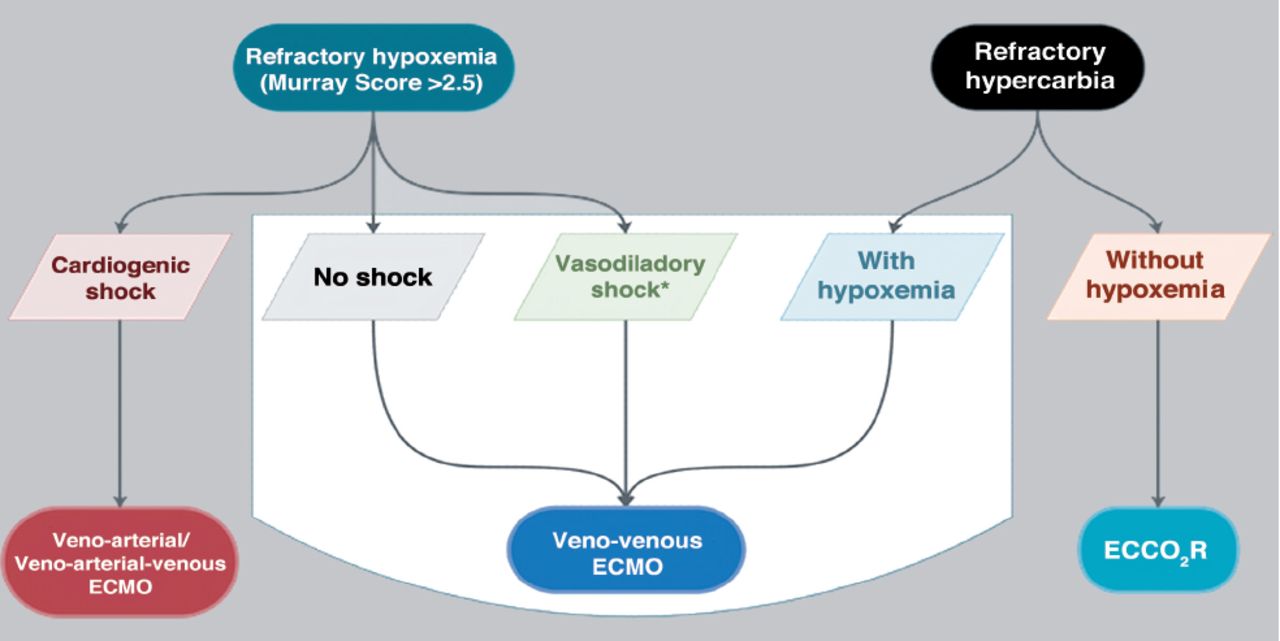
- Figure 1
- The extracorporeal strategies that can be used for supporting patients with ARDS. ECMO: extracorporeal membrane oxygenation (ECMO). ECCO2R: extracorporeal CO2 removal
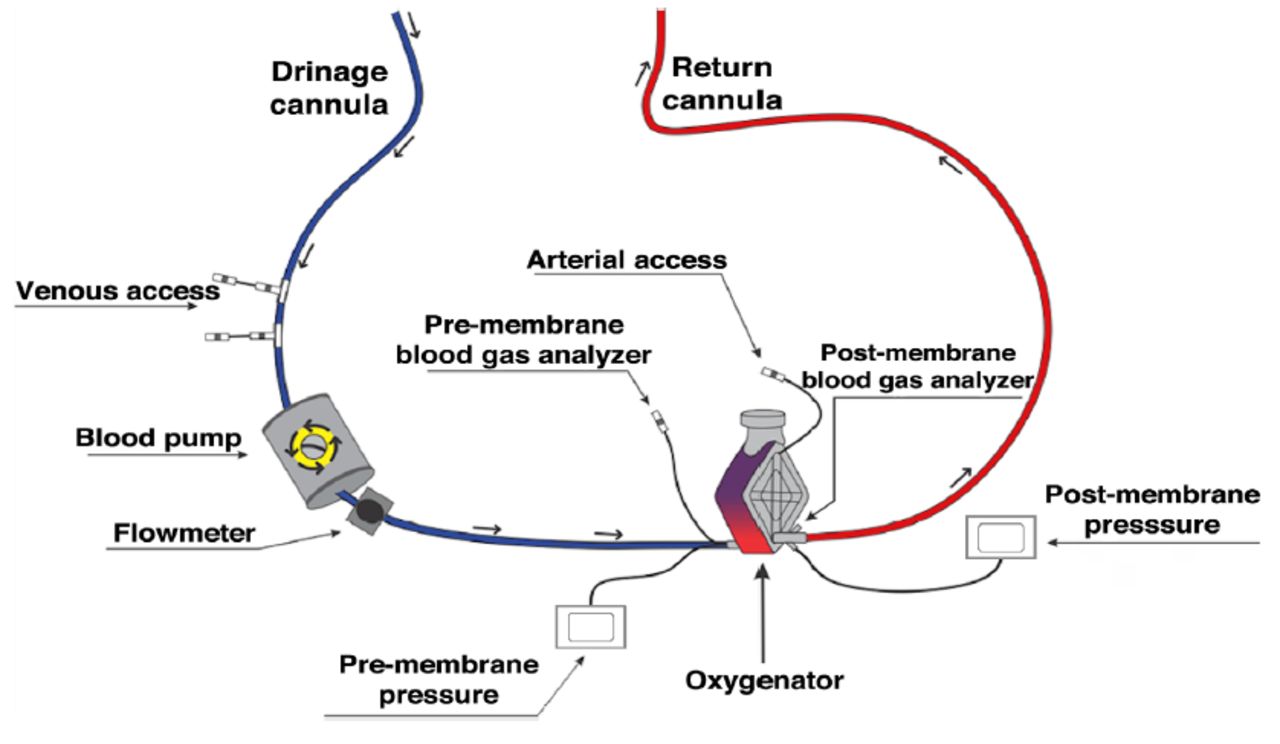
- Figure 2
- General demonstration of the standard components of an extracorporeal membrane oxygenation (ECMO) circuit.
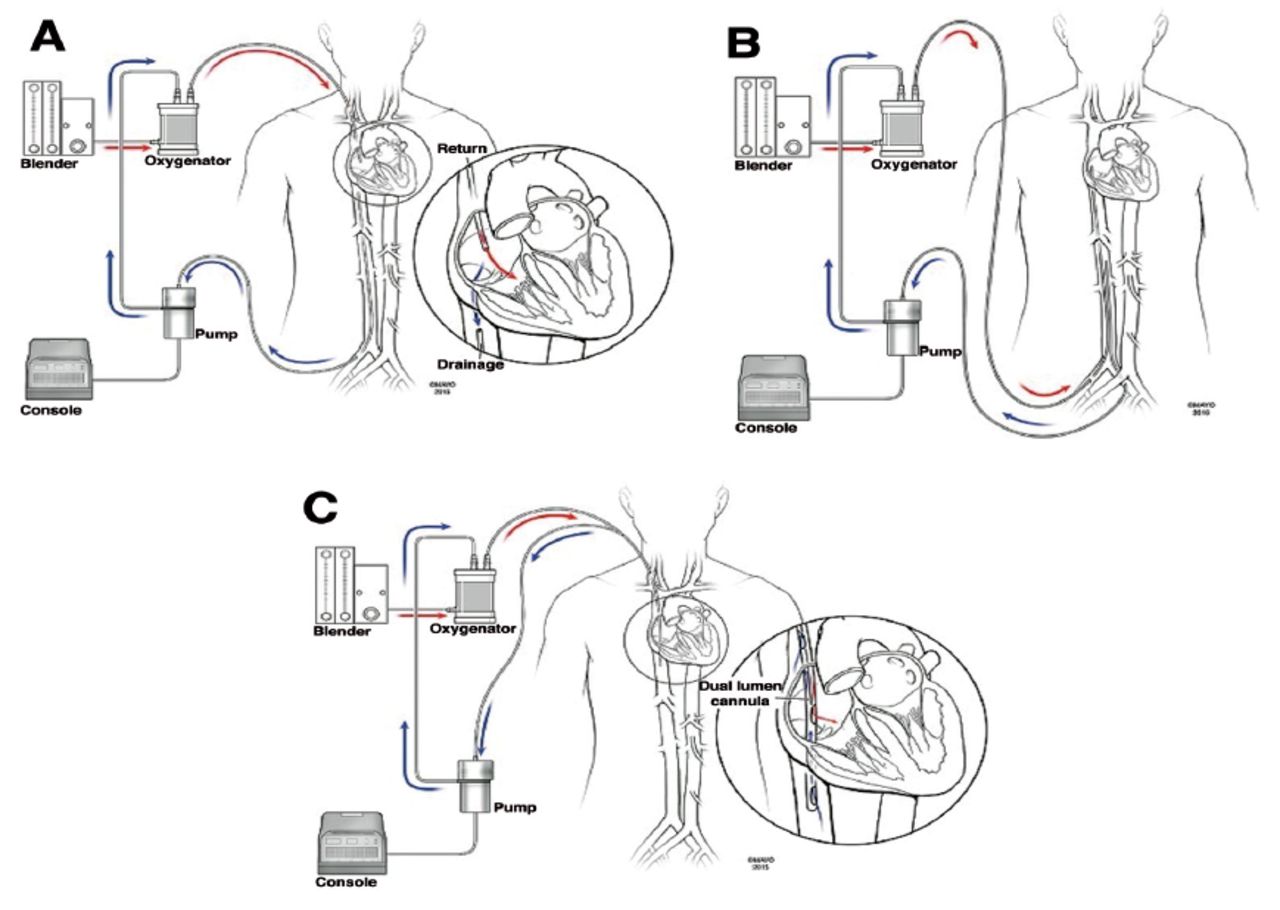
- Figure 3
- Common venvenous(VV) extracorporeal membrane oxygenation (ECMO) configurations. A) Conventional VV ECMO, fem–IJ configuration. B) Fem–fem VV ECMO. C) Single cannula with dual ports, one for drainage and another for return that directs oxygenated blood toward the tricuspid valve.
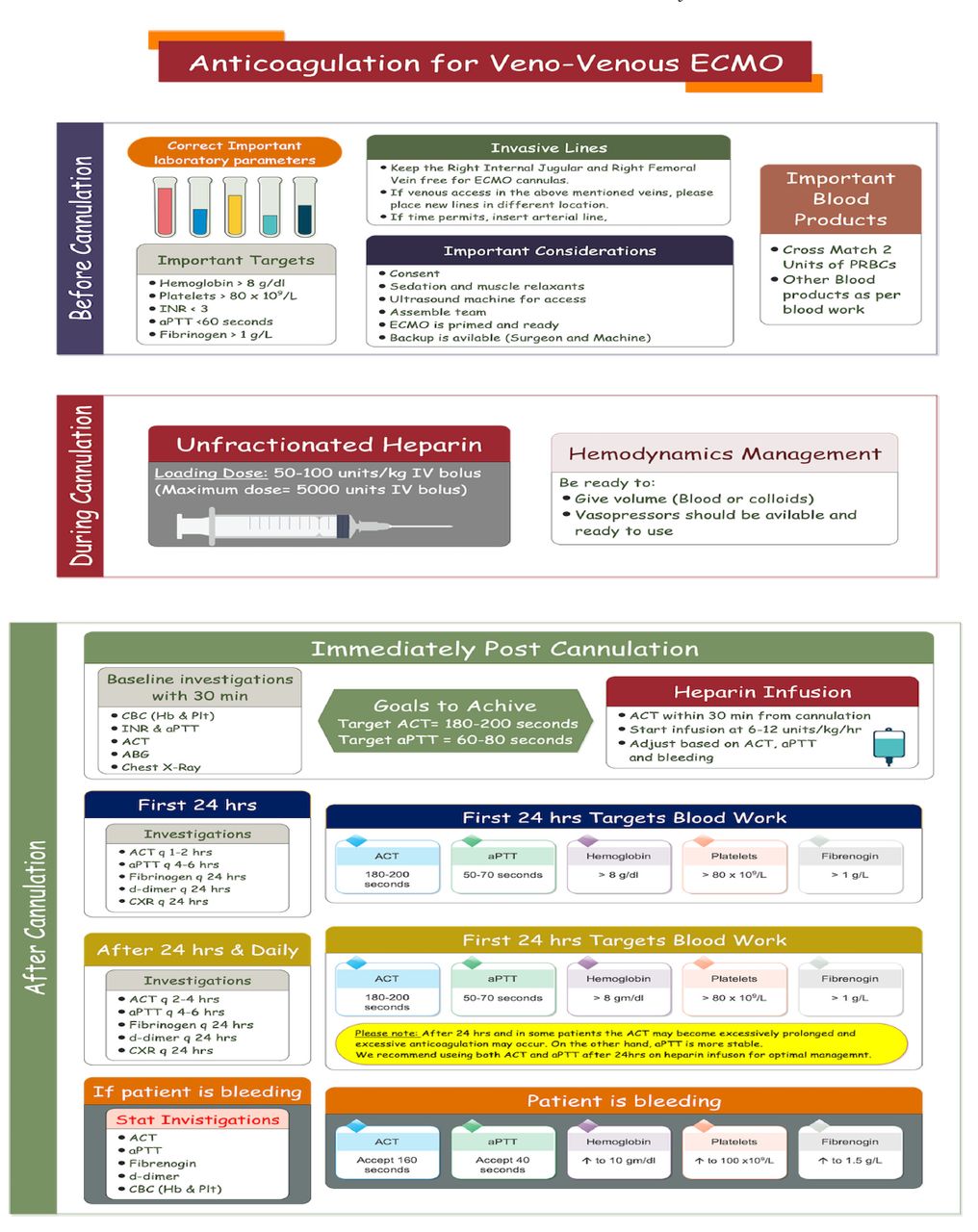
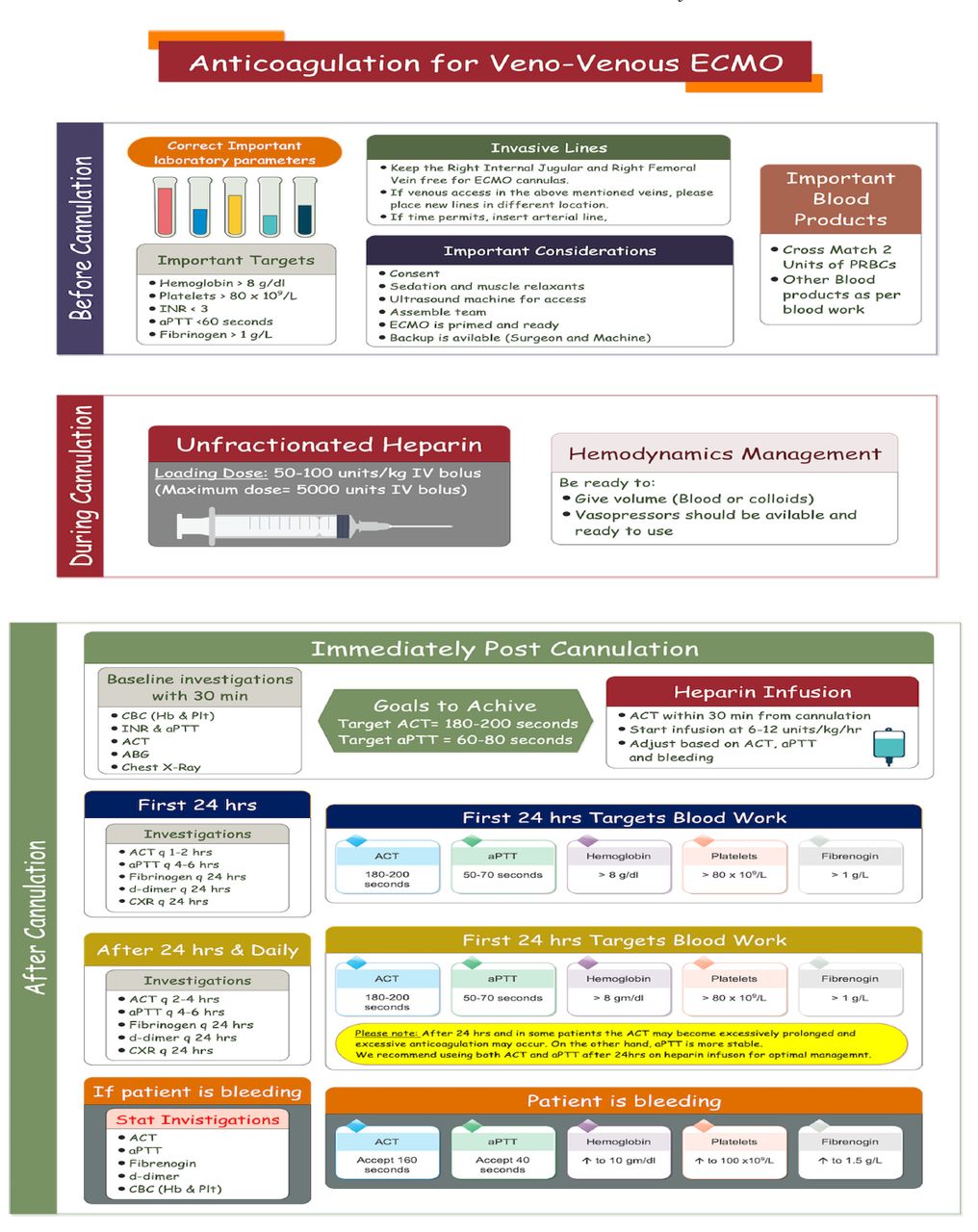
- Figure 4
- Anticoagulation on veno-venous extracorporeal membrane oxygenation. INR: International Normalized Ratio, aPTT: activated partial thromboplastin time, ACT: activated clotting time, CBC: complete blood count
- Figure 5
- Management of veno-venous ECMO and the ventilator PEEP: peek end expiratory pressure, Pplat: plateau pressure, ECMO: extracorporeal membrane oxygenation, ARDS: acute respiratory distress syndrome, FiO2: oxygenation, IBM: ideal body mass, IBW: ideal body weight, H20: water, RR: respiratory rate, PaO2: partial pressure of oxygen
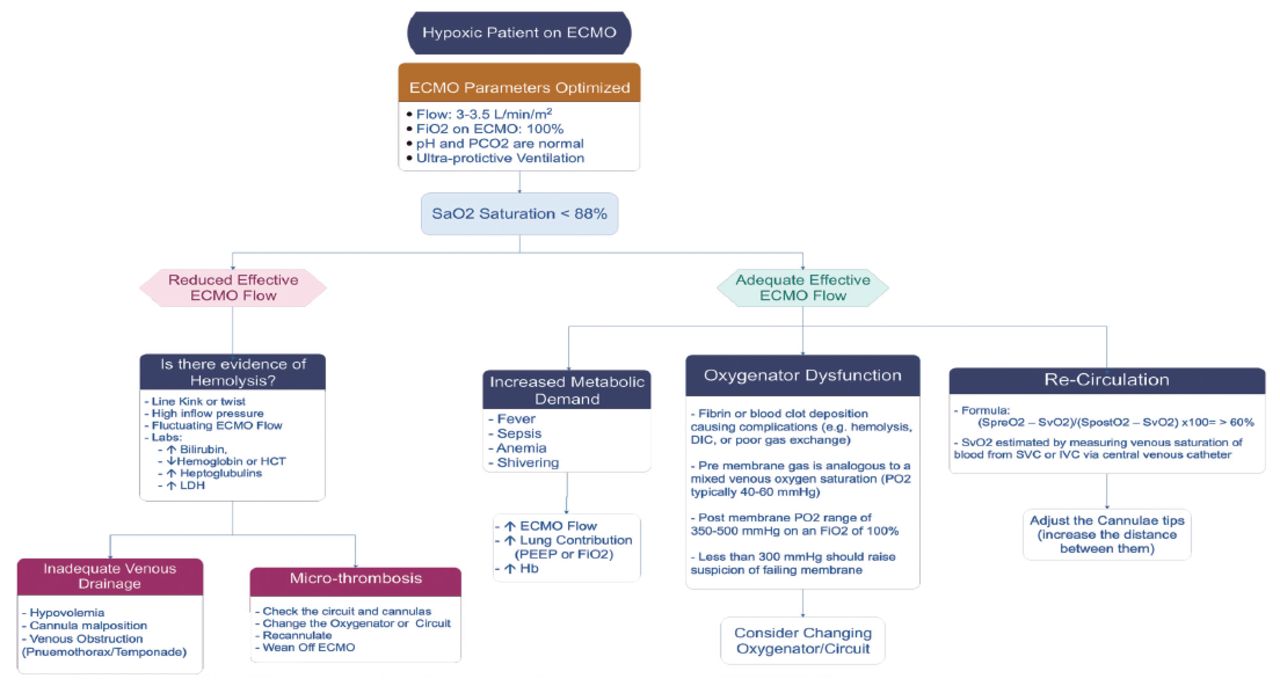
- Figure 6
- Low O2 saturation on ECMO. LDH: lactate dehydrogenase, ECMO: extracorporeal membrane oxygenation, PEEP: peek end expiratory pressure, IV: FiO2: fraction of inspired oxygen, Hb: hemoglobin, PO2: partial pressure of oxygen, DIC: disseminated intravascular coagulation, SVC: superior vena cava, IV: intravenous
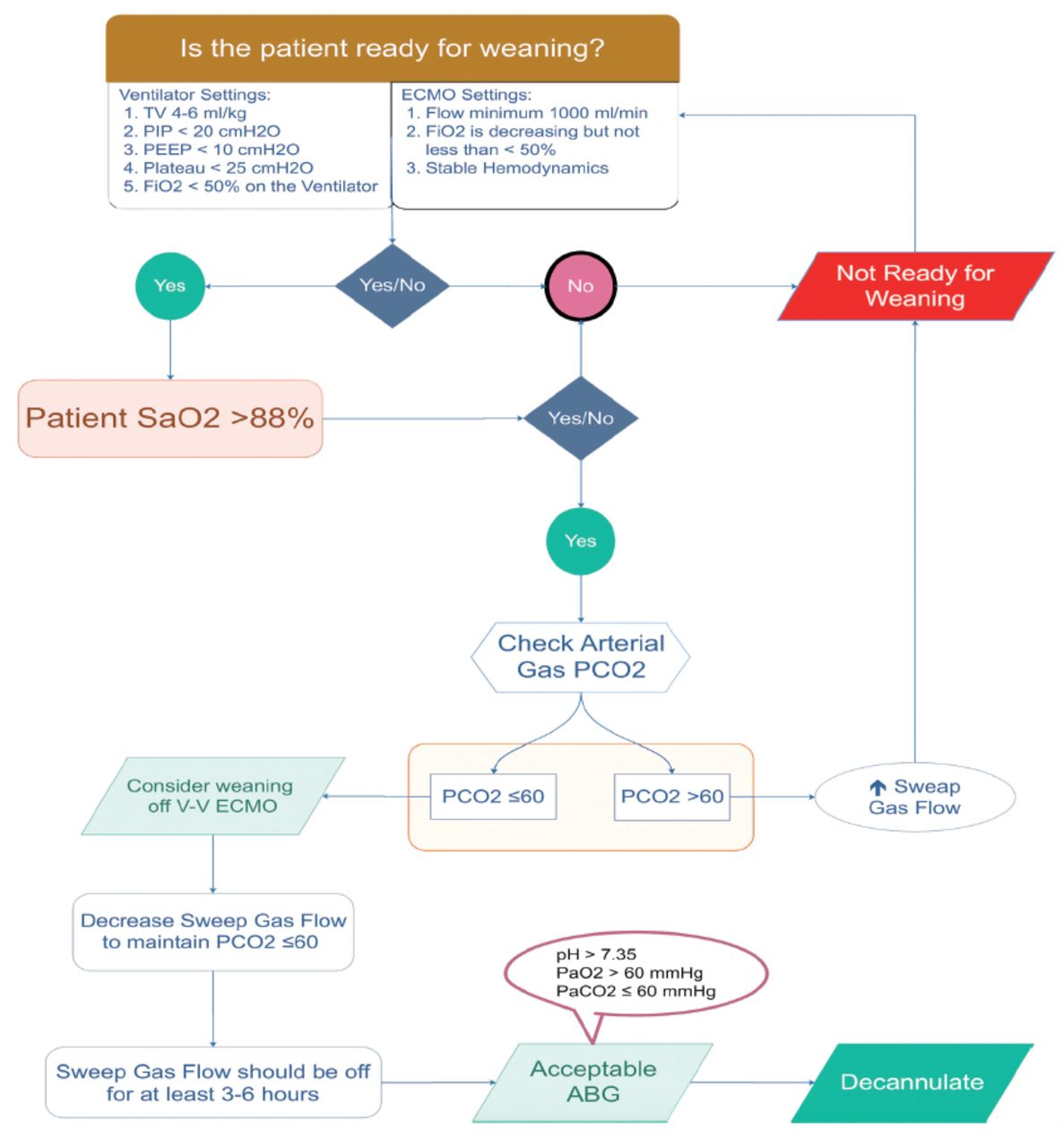
- Figure 7
- Assessment of patient readiness for weaning off veno-venous ECMO PEEP: peek end expiratory pressure, Pplat: plateau pressure, ECMO: extracorporeal membrane oxygenation, ARDS: Acute Respiratory Distress Syndrome, FiO2: oxygenation, ABG: arterial blood gasses
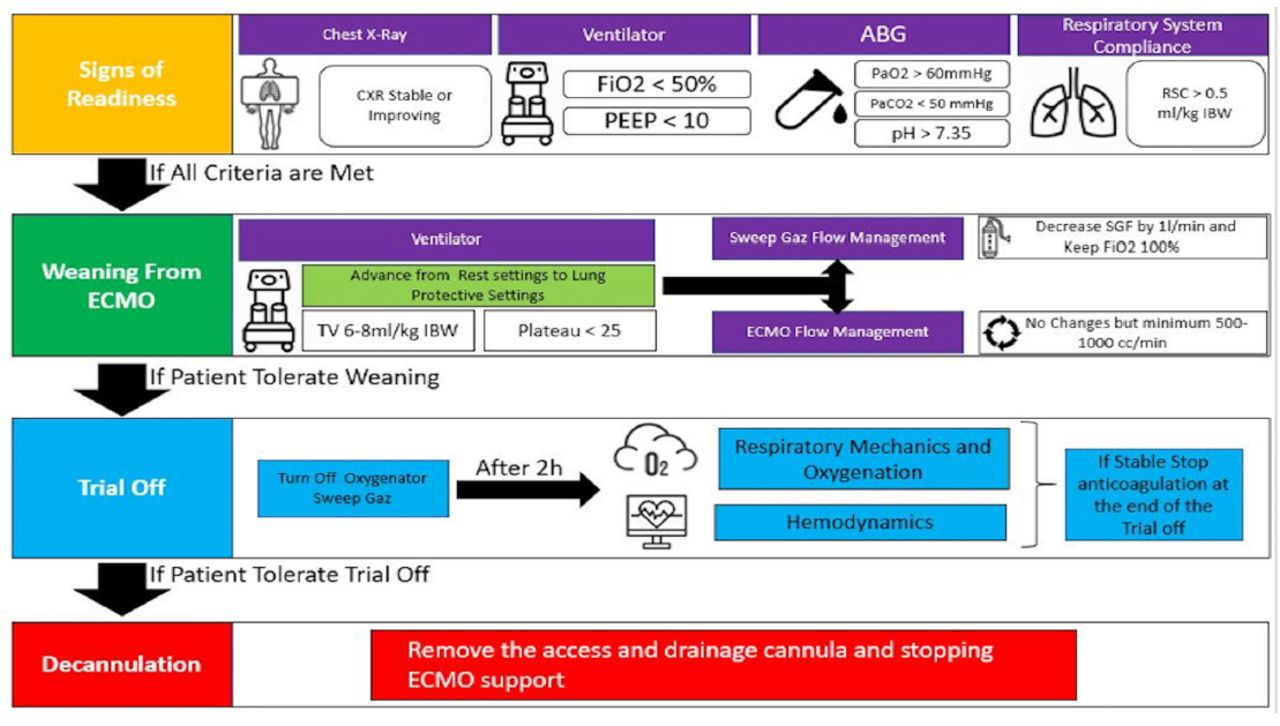
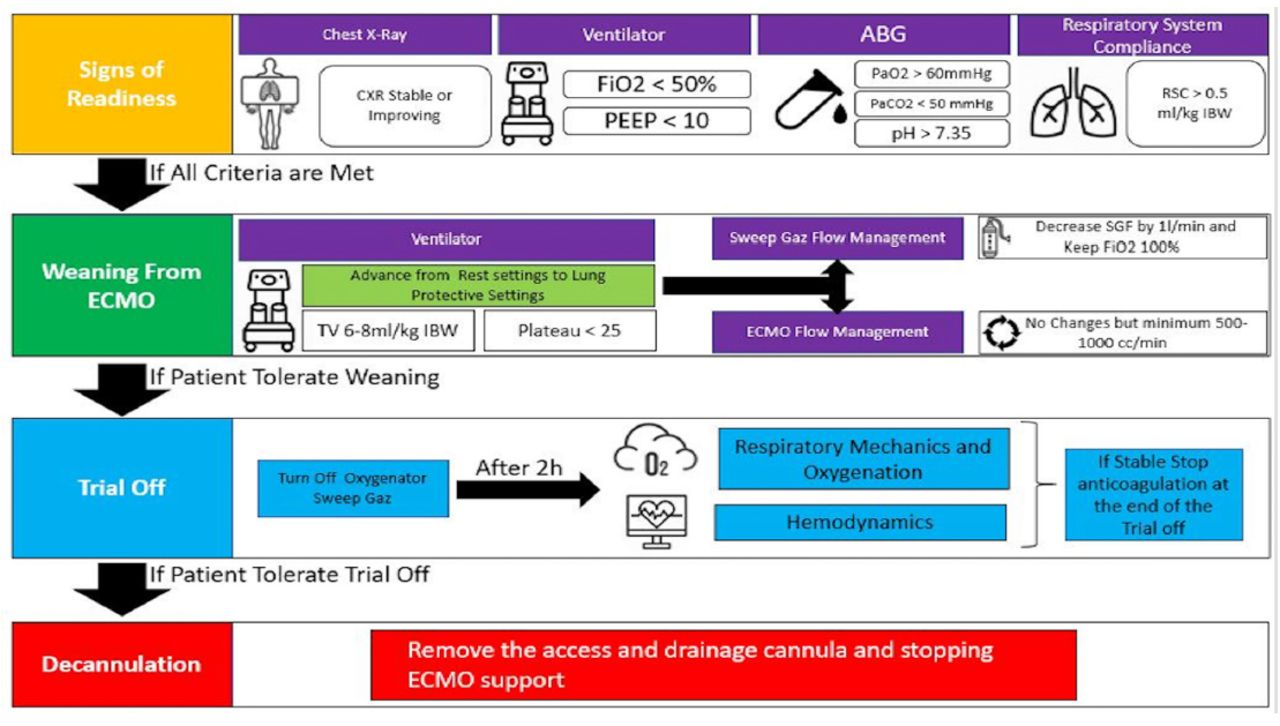
- Figure 8
- Process of liberation from veno-venous ECMO. peek end expiratory, Pplat: plateau pressure, ECMO: extracorporeal membrane oxygenation, ARDS: Acute Respiratory Distress Syndrome, FiO2: oxygenation, IBW: ideal body weight, RSC; respiratory system compliance, H: hours, ABG: arterial blood gasses, CXR: chest x-ray, PEEP: peek end expiratory pressure
- Figure A1
- Variable flow on veno-venous extracorporeal membrane oxygenation (ECMO).
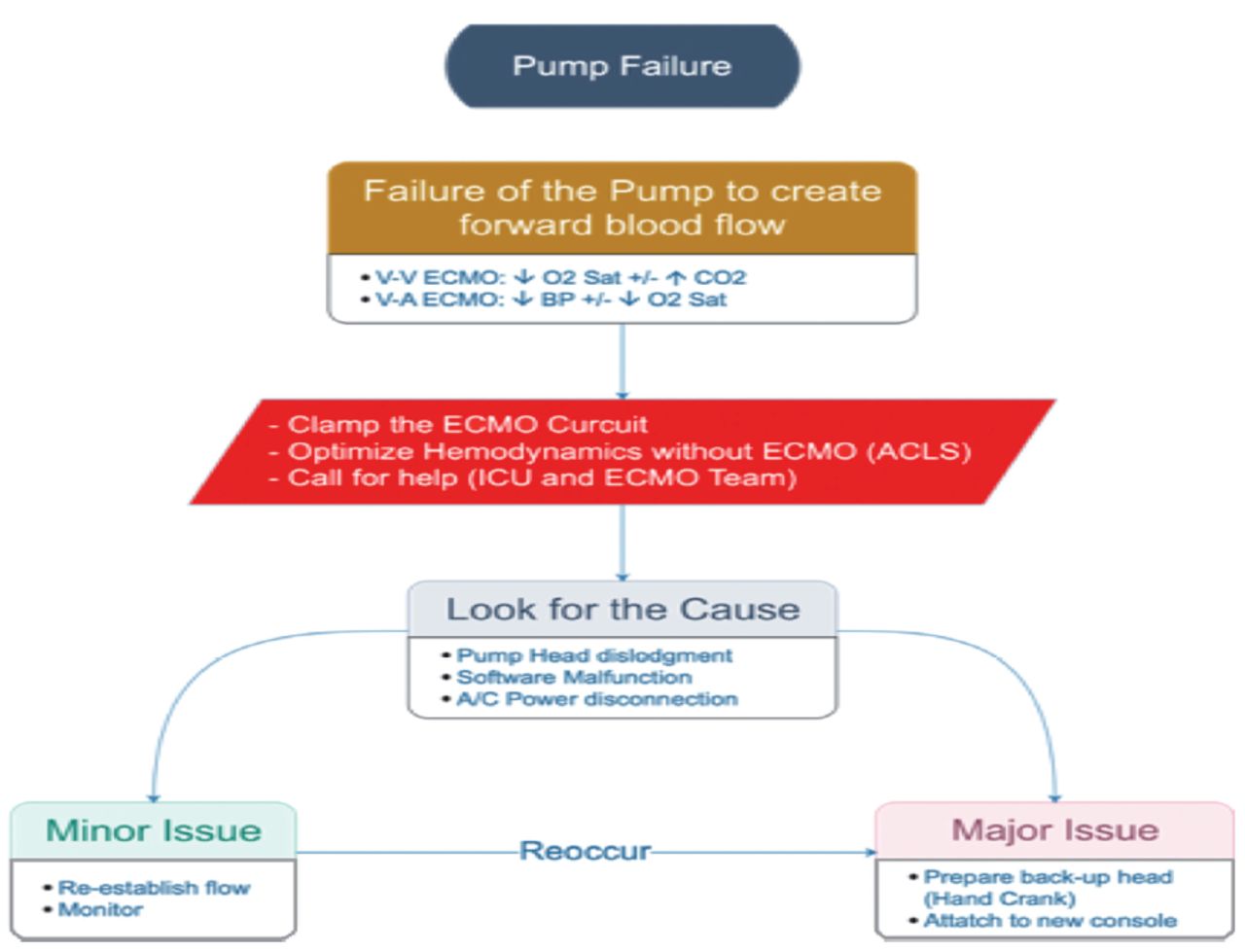
- Figure A2
- Pump failure. VV: veno-venous, VA: veno-arterial, ECMO: extracorporeal membrane oxygenation, ICU: intensive care unit, ACLS: advanced cardiac life support
- Figure A3
- Circuit rupture. VV: veno-venous, VA: veno-arterial, ECMO: extracorporeal membrane oxygenation, ICU: intensive care unit, ACLS: advanced cardiac life support
- Figure A4
- Accidental decannulation VV: veno-venous, VA: veno-arterial, ECMO: extracorporeal membrane oxygenation, ICU: intensive care unit, ACLS: advanced cardiac life support
- Figure A5
- Accidental decannulation VV: veno-venous, VA: veno-arterial, ECMO: extracorporeal membrane oxygenation, ICU: intensive care unit, ACLS: advanced cardiac life support
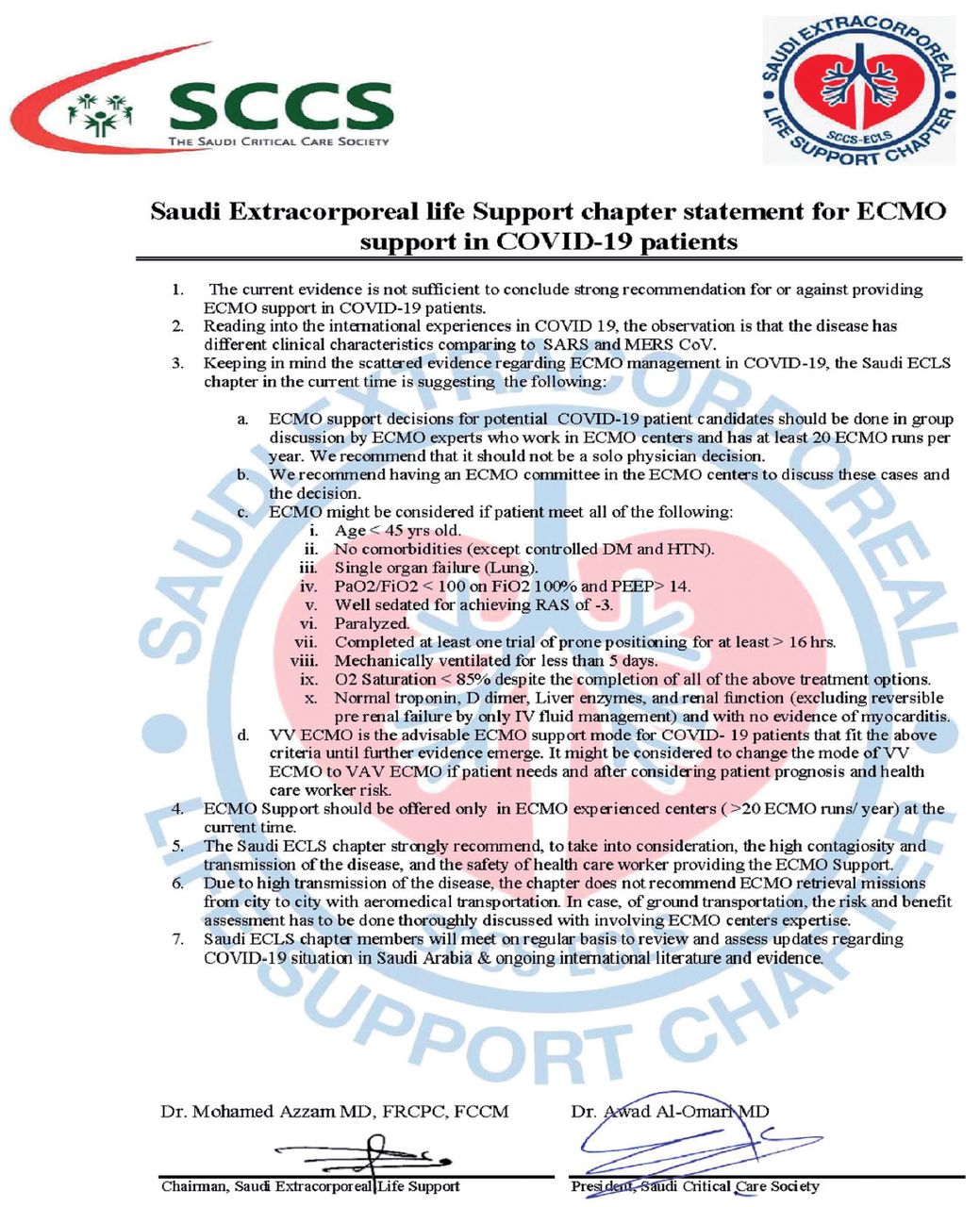
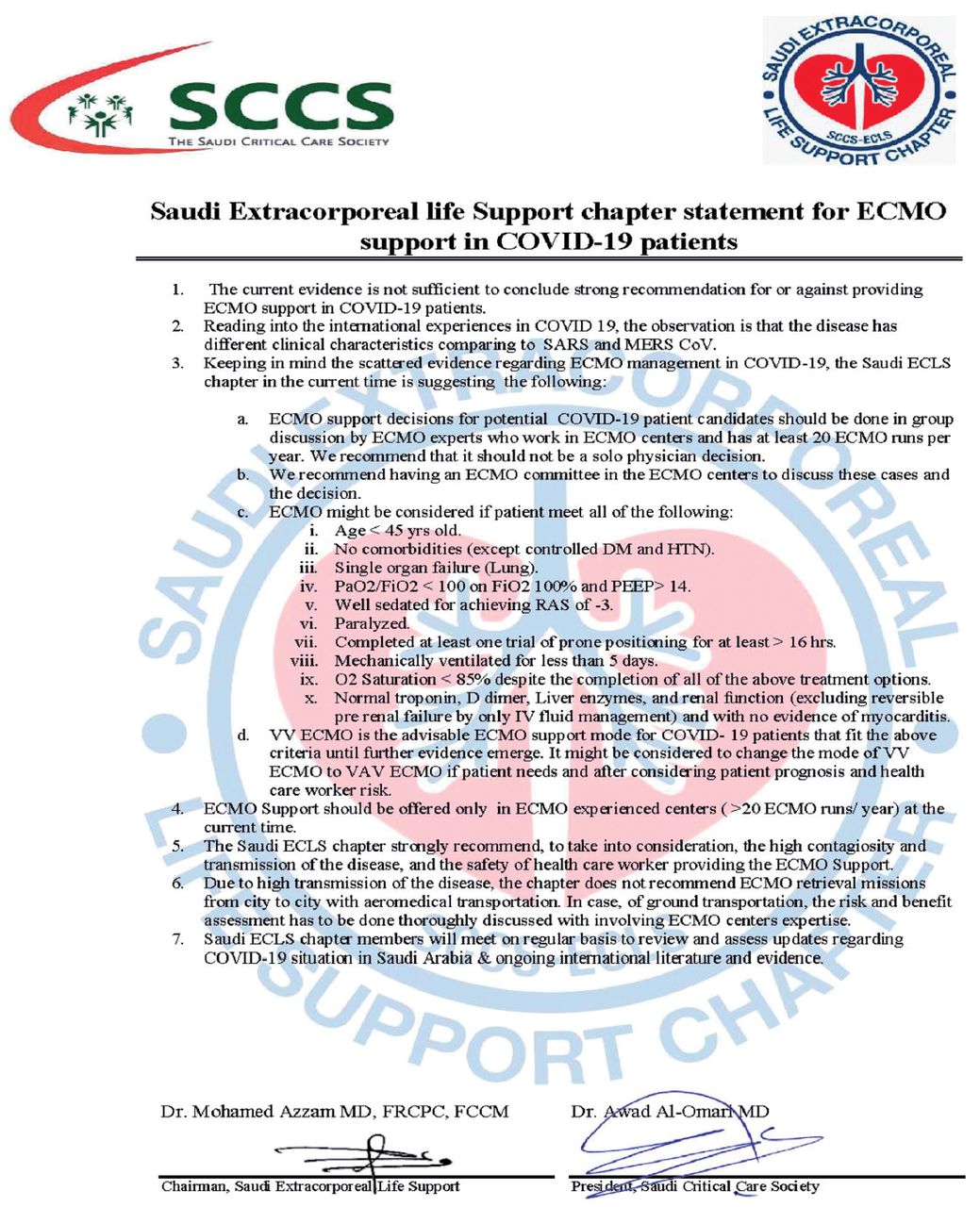
- Figure A6
- The first Saudi extracorporeal life support (ECLS) chapter statement for extracorporeal membrane oxygenation (ECMO) support in COVID-19 patients, released April 9, 2020.
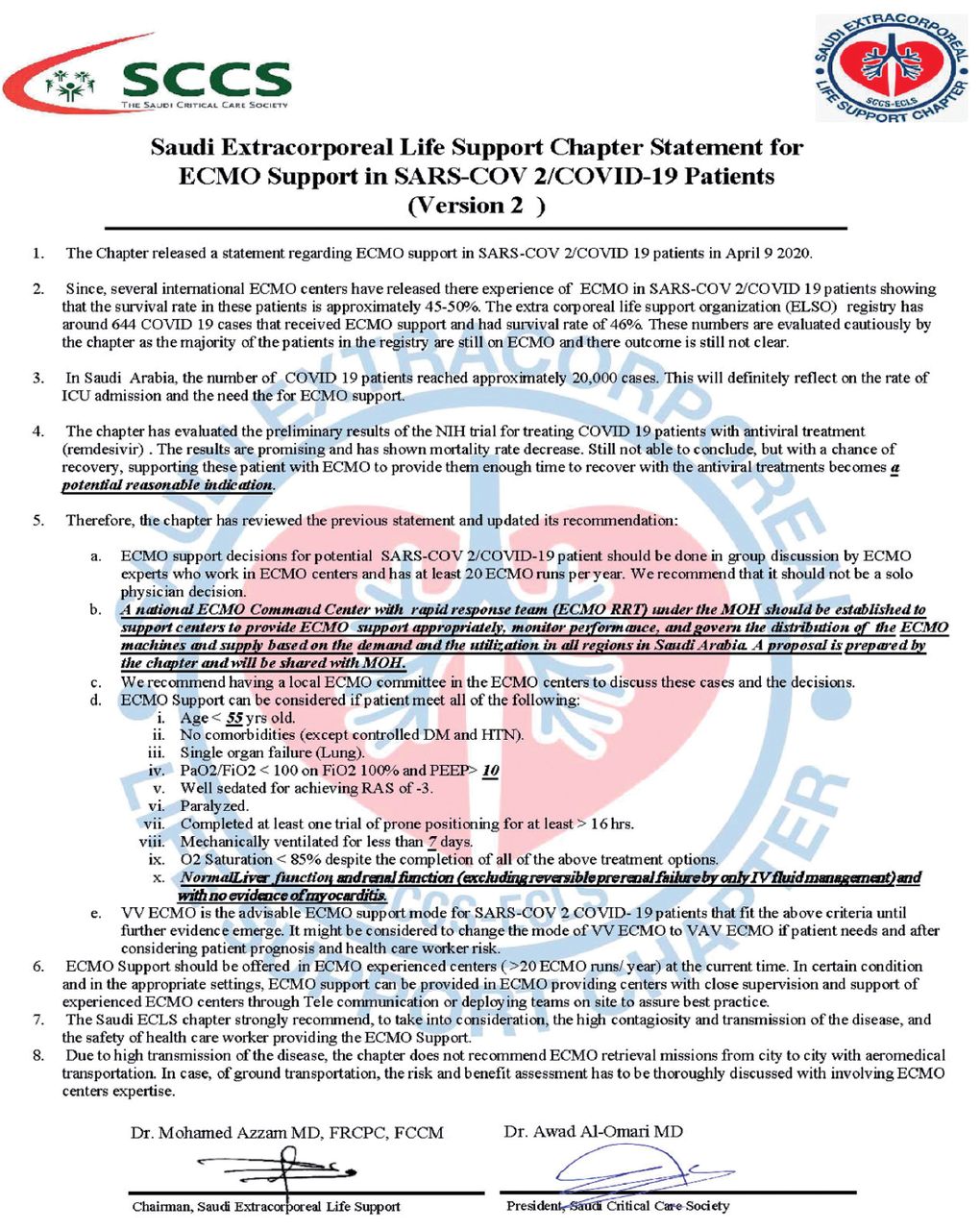
- Figure A7
- The second Saudi extracorporeal life support (ECLS) chapter statement for extracorporeal membrane oxygenation (ECMO) support in COVID-19 patients, released May 1, 2020.








Tables
Indications for VV ECMO for respiratory failure: Consider referring a patient with severe acute respiratory distress syndrome (ARDS) after optimization of all other conventional modalities if the patient has: Severe hypoxic respiratory failure: PaO2/FiO2 ratio <80 for 6 hours PaO2/FiO2 ratio <50 for 3 hours Severe hyper-carbic respiratory failure: pH <7.2 with pCO2 >60 mm Hg for >6 hours.2 - Table 2
- General indications for veno-venous (VV) extracorporeal membrane oxygenation (ECMO).
Contraindications for VV ECMO for respiratory failure: The following are some of the contraindications for ECMO in patients with severe Acute Respiratory Distress Syndrome that should be considered before referral: Absolute Circulatory collapse requiring cardiopulmonary resuscitation for >15 min (no extracorporeal cardiopulmonary resuscitation). Contradictions for anticoagulation (active bleeding or recent major surgery). Poor baseline functional status (Eastern Cooperative Oncology Group score 0-2).1 (Appendix A) Significant comorbidities associated with poor outcomes: Neurological (such as, stroke within the last 6 months, seizure disorder, dementia). Respiratory (such as, severe chronic obstructive pulmonary disease [COPD], pulmonary fibrosis, cystic fibrosis). Cardiac (such as, severe heart failure with left ventricular election fraction <30% from any cause, history of major cardiac intervention). Gastrointestinal (such as, severe short gut syndrome, Crohn’s disease, ulcerative colitis). Hepatological (such as, liver cirrhosis with child-pugh B or C). Advanced solid organ malignancy (such as, advanced-stage colon cancer). Severe peripheral vascular disease. Severe liver failure with elevated International Normalized Ratio and derangement of liver enzymes. Poor neurological status (due to intracranial bleeding, cerebrovascular accident, or others). Relative Prolonged high setting mechanical ventilation (>7 days). Age >65 years. Left ventricular ejection Fraction <30% with no previous history of low ejection fraction. Renal (such as, end-stage renal disease on hemodialysis). Morbid obesity (body mass index > 35 kg/m2). Immunocompromised status (such as, post-renal transplant). Hematological malignancies within the last 5 years. - Table 3
- Possible causes and management of bleeding on extracorporeal membrane oxygenation (ECMO).
Cause Cause Solution a) Low mean arterial pressure (MAP) with good ECMO flow and NO visible bleeding AND ACT is too high Internal bleeding Reduce anticoagulation Investigate source of bleeding b) Low MAP with good ECMO flow and no visible bleeding AND ACT is within range Double check hemoglobin reading Make sure that patient is not fluid-overloaded Transfuse Fluid removal c) Low MAP with good ECMO flow and visible bleeding Bleeding from wounds or cannula sites Transfuse Compress Call surgical team d) Bleeding with low platelets Destruction of platelets from ECMO Heparin-induced thrombocytopenia (HIT) Transfuse platelets Check for HIT Change anticoagulant e) Bleeding with normal platelets Factor deficiency Unstable fibrin clot Check coagulation Fibrinogen level TEG or ROTEM if available Treat cause TEG: thromboelastography, ROTEM: rotational thromboelastometry, ACT: activated clotting time - Table 4
- Possible causes and management of low O2 saturation on extracorporeal membrane oxygenation (ECMO).
Cause Solution Note ↓ ECMO blood flow ↑ ECMO blood flow (↑RPMs) Look for cause ↓ Hemoglobin ↑ Hemoglobin (transfusion) Look for bleeding Inadequate FiO2 or ventilator support ↑ FiO2 on ECMO↑ Ventilator support Look for cause Too much flow through shunts or bridges (such as, contentious renal replacement therapy) Check and reduce shunt flow Oxygenator failure Check pre- and post-oxygenator blood gases If yes → change Pneumothorax Chest x-ray Cause Issue Improved pulmonary function Check tidal volumes (consider ECMO weaning protocol) ECMO pump flow is too high Decrease ECMO flow gradually down to 3 L/min, then decrease FiO2 after (consider ECMO weaning protocol) Category Causes Response ECMO-related i. Gas flow rate is too low i. ↑ Sweep gas flow ii. Oxygenator failure ii. Check pre- and post-oxygenator blood gases Patient-related i. Pneumothorax i. CXR ii. Hemothorax ii. Pulmonary cultures iii. Ventilator-associated pneumoniaiv. PE iii. Bronchoscopyiv. CT PE Ventilator-related Inadequate ventilation Adjust ventilator parameters pCO2: partial pressure of carbon dioxide, PE: pulmonary embolism, CXR: chest x-ray, CT: computed tomography Causes Response i. Gas flow rate is too high i. ↓ Sweep gas flow ii. Tachypneic ii. Treat the underlying cause iii. Over-ventilated iii. Adjust ventilator settings Eastern Cooperative Oncology Group (ECOG) performance status Grade ECOG 0 Fully active, able to carry out all pre-disease performance without restriction 1 Physically strenuous activity is restricted, but is ambulatory and able to carry out work of a light or sedentary nature, e.g., light housework, office work 2 Ambulatory and capable of all selfcare but unable to carry out any work activities. Up and about for >50% of waking hours 3 Capable of only limited selfcare, confined to bed or chair for >50% of waking hours 4 Completely disabled. Cannot carry out any selfcare. Totally confined to bed or chair 5 Dead Cause Action Response Change in venous cannula position Reduce pump speed (rpm) temporarily and optimize ventilator settings This will improve venous drainage until the cause is addressed and there is definitive management Hypovolemia If patient is hypovolemic due to high urine output: Aggressive diuresis, bleeding, etc. Volume assessment Give volume/transfuse Other causes of increased intrathoracic or abdominal pressure (pneumothorax, cardiac tamponade, intrabdominal bleeding, and so on) Change the patient position and/or venous cannula position Tip migration Check by x-ray Check tubing and pump head for fibrin or clot Consider changing the cannula or circuit Venous line obstruction by clot or kink or twist Consider FAST (focused assessment with sonography for trauma) exam and manage accordingly May require surgical intervention Cause Cause Solution a) Clots in oxygenator • Low extracorporeal membrane oxygenation blood flow
• Inadequate anticoagulation
• High pre-oxygenator pressure
↑ ECMO flow
↑ Anticoagulationb) Decreased patient O2% saturation Check pre- and post-oxygenator blood gases Change oxygenator c) ↓ pO2 Check pre- and post-oxygenator blood gases ↑ FiO2 d) ↓ pCO2 Check pre- and post-oxygenator blood gases ↑ Sweep
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.