


Abstract
Objectives: To compare the clinicopathological, histological and immunohistochemical features of breast cancer (BC) in between young (≤40 years) and older (>40 years) patients.
Methods: This retrospective study included histopathological reports of all patients with primary BC diagnose at the King Fahad Hospital, Madinah, Saudi Arabia between January 2006 and November 2020.
Results: During the study period, a total of 708 patients with BC were identified; 173 cases (24.4%) were ≤40 years old and 535 (75.6%) were above 40 years. There were significant differences in tumor size (p=0.046), tumor grade (p<0.0001), tumor stage (p=0.047), lymphovascular invasion (p<0.0001), and distant metastasis (p<0.0001) between the 2 groups. Comparing the status of the hormone receptors and molecular subtypes between the 2 age groups, BCs in the younger patients were triple–negative (p=0.008) in majority of the cases and less likely to be estrogen receptor (ER) and progesterone receptor (PR) hormone receptors–positive (p=0.0001, p<0.0001). Young patients exhibited the HER2/neu type with more frequent statistical significance (p=0.016) and the tumor type luminal A (p=0.002) with less frequent statistical significance compared to old patients.
Conclusion: Although BC in young women is uncommon, it may be different with regards to poor prognostic outcomes, which are attributed to more aggressive histopathological features and less favorable receptor status when compared to the cases diagnosed in older women.
The breast cancer (BC) is the most common cancer throughout the world and the fifth common cause of cancer death.1 In year 2020, GLOBOCAN in their statistics reported 2.26 million cases of BC which accounted for 11.7% of all cancer cases throughout the world.2 However, a recent Saudi Cancer Registry (SCR) reported 2,282 new cases of BC in the whole Saudi Arabia accounting for 17.3% of all cancer cases, which was significantly higher than the GLOBOCAN statistics, moreover, BC was found to be 30.4% of all new cancer diagnosed in women making it the most common cancer in the kingdom.3 While, in the western population the BC in the women less than 40 years of age is uncommon and accounts for 3.7%-6.6% of the total number of BC cases.4-7 However, a very high rate of BC in the young patients (29%-31.6%) was reported in the literature from Nigeria and India.8,9 In Saudi Arabia also the figures are higher than the western countries, according to the latest SCR report, 18.9% of all BC cases are diagnosed in women <40 years old.3
Compared to older patients, BC diagnosed at a young age is likely to behave more aggressively and prone to present with a high grade tumor, larger tumor size, more lymph node involvement, lymphovascular invasion and an advanced tumor stage with more triple-negative, human epidermal growth factor receptor 2 (HER2/neu) overexpression and fewer luminal A and B breast cancer.10-13 In line with this, higher incidence of loco-regional recurrences and distant metastases have been reported in younger BC patients, contributing to a poorer prognosis.14 Accordingly, different treatment strategies are required to treat this patient population in order to achieve optimal therapeutic outcomes. The major issues in managing the BC in young patients requires a multidisciplinary team involving many specialties including psychological approach, preservation of the fertility, management of future pregnancies and financial implication on the individual and the family. Keeping in mind the high incidence rate of BC in Saudi women, the principle aim of this retrospective study was to report and analyze the clinicopathological, histological and immunohistochemical features of BC between the young and old female patients from Madinah, Saudi Arabia.
Methods
This study was conducted retrospectively to analyze BC cases from January 2006 to November 2020 at King Fahad Hospital (KFH) Madinah, Saudi Arabia. During this period, a total of 708 cases of BC were reported in the histopathology laboratory of the KFH. Patients’ demographic informations such as age, gender, nationality and final diagnosis of the biopsy or surgery of the breast tumor, tumor type, tumor grade, tumor size, status of lymph nodes, lymphovascular invasion, any available history of recurrence, type of surgery (namely, breast conserving surgery or modified radical mastectomy), and status of hormone receptors were retrieved from the histopathology laboratory computer database. The inclusion criteria were the diagnosis of primary BC (both invasive as well as in-situ) in Saudi female patients of all age groups. Non-Saudis, male patients and metastatic BCs were excluded from the study. The 2019 World Health Organization (WHO) classification of BC was applied for histological typing.15 The Modified Bloom-Richardson (MBR) system was used to assess the tumor grade, while the estrogen and progesterone receptor (ER, PR) reactivity was evaluated according to the St Gallen Consensus 2009 which was documented by a positive nuclear staining pattern.16 The Her-2/neu staining was assumed positively reacting when a strong complete membranous staining was noted in more than 10% of tumor cells. Based on the receptor status of BC in our cohort we classified them according to Dai et al17 molecular subtypes:
ER +, PR +/-, Her-2/neu Negative - Luminal A (ER + and low grade)
ER +, PR +/-, Her-2/neu + - Luminal B (ER + but often high grade)
ER -, PR -, Her-2/neu + - Her-2/neu Amplified
ER -, PR -, Her-2/neu Negative - Basal like (Triple negative breast cancer)
The nuclear immunostaining of Ki67 was assessed by counting at least 500 tumor cells per case across 5 high power fields of the section under microscope. The Ki67 proliferative index (PI) was scored as high when >25% of the tumor cells were positive; and low when <25% of the tumor cells were positive.
The patients were assigned in 2 groups; Group 1 comprises a total of 173 patients equal to or less than 40 years of age (young patients), and Group 2 which comprises 535 patients more than 40 years of age (old patients). The American Joint Committee on Cancer (AJCC seventh edition) tumor (T), nodes (N), and metastases (M) (TNM) staging system for BC was used to stage the patient in both the groups in our cohort.
Both the groups were compared for clinico-pathological, histological and immunohistochemical features. Statistical analysis of our data was performed with Statistical Package for Social Sciences (SPSS), version 21.0 (IBM Corp. Armonk, New York, USA). Comparisons of categorical variables between the 2 groups were assessed using Pearson’s Chi-square test. In all statistical tests, a p<0.05 was considered statistically significant. Approval for the publication of this study was taken from the Department of Pathology, KFH, Madinah Saudi Arabia.
Results
An aggregate of 708 women with BC were included in this study; 173 cases (24.4%) were ≤40 years old (Group 1) and 535 (75.6%) were above 40 years (Group 2). The age for all the patients ranged between 20 and 112 years with a mean age of 50.6 years. The mean age of the younger group was 34.1 years (range 20-40 years) and the mean age of the older group was 55.9 years (range 41-112 years).
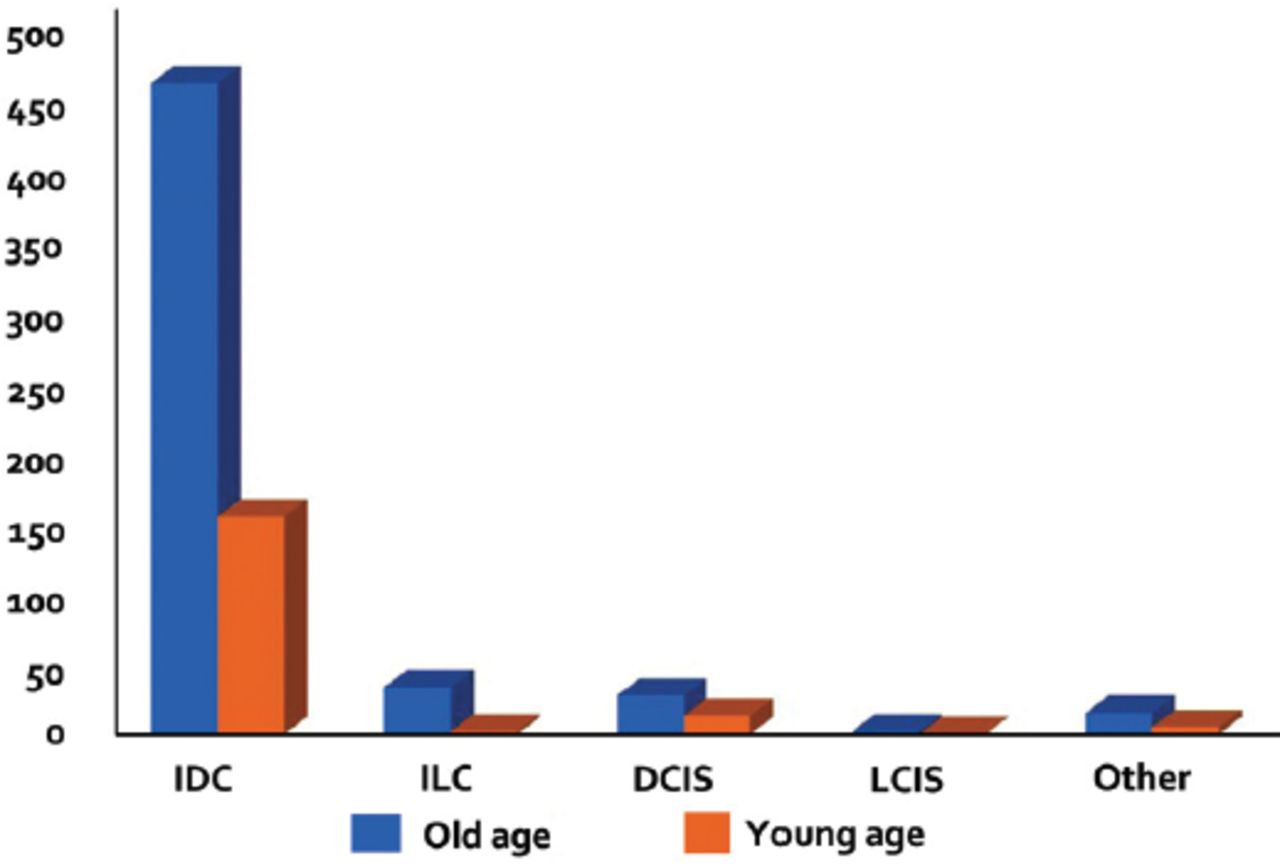
Our findings of clinicopathological, histological, and immunohistochemical features and their comparison between Group 1 and Group 2 is summarized in Table 1. Significant statistical differences were noted of the following parameters between the 2 groups; tumor size (4.5 cm in Group 1 and 3.7 cm in Group 2, p=0.046), tumor grade (more patients with grade III tumors in Group 1), lymphovascular invasion (28.5% of patients in Group 1, p<0.0001), distant metastasis and stage IV disease (more in Group 1, p<0.0001 and p=0.046). The invasive ductal carcinoma (IDC) was the most common histological subtypes of breast cancer reported in both groups. Moreover, other histological subtypes and ductal carcinoma in situ (DCIS) showed no significant statistical difference. However, a significant difference was noted in the occurrence of invasive lobular carcinoma (ILC), which was seen more frequently in Group 2 patients (p=0.028) as shown in Figure 1.
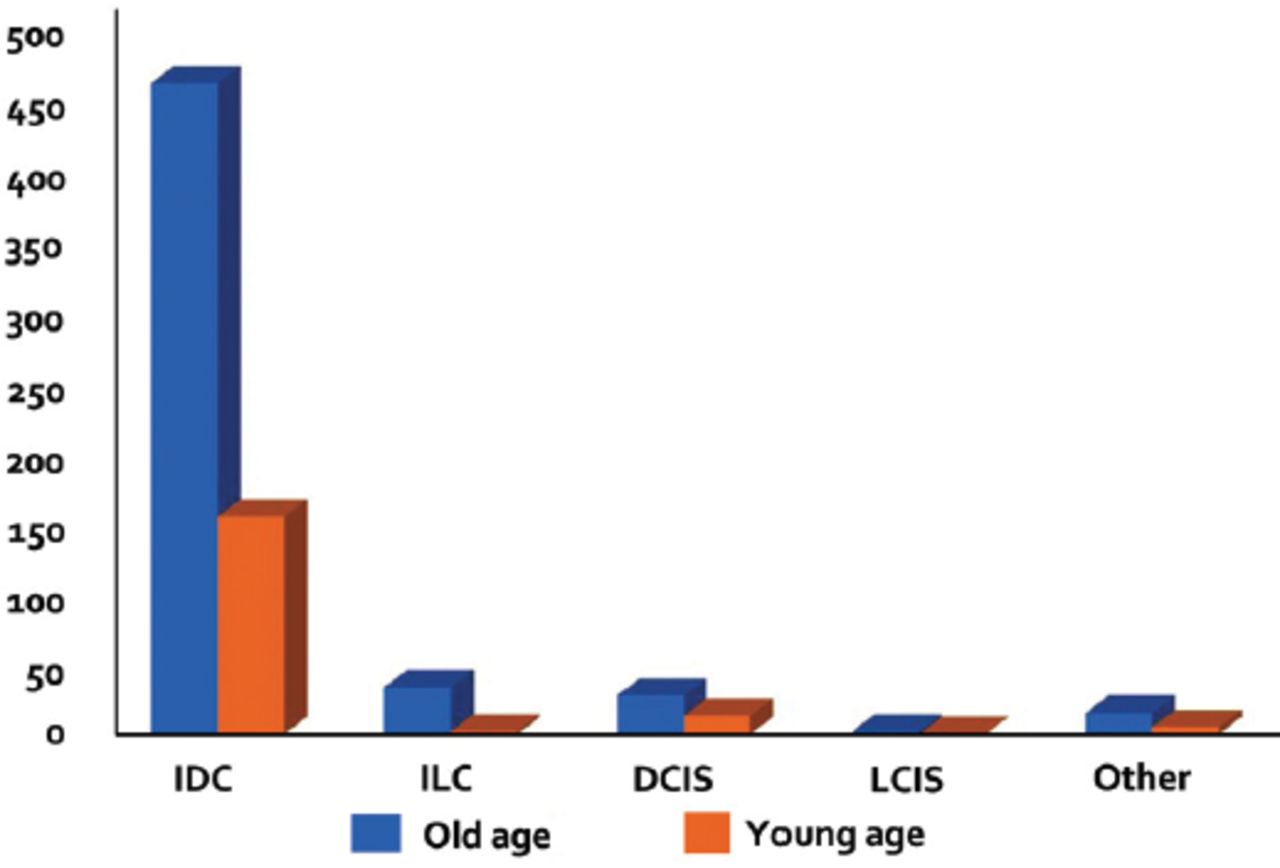
- The differences in histological subtypes between the younger and older patients (p=0.174). IDC: invasive ductal carcinoma, ILC: invasive lobular carcinoma, DCIS: ductal carcinoma in situ, LCIS: lobular carcinoma in situ
- Comparison of clinicopathological features between the young and old patients (≤40 years and >40 years of age) at diagnosis.
The other findings such as lymph node status (p=0.606), type of surgery (p=0.150), Ki67 PI (p=0.082), locoregional recurrence (p=0.163), and concomitant DCIS (p=0.441) did not significantly differ between the 2 age groups.
Comparing the status of the hormone receptors and molecular subtypes between the 2 age groups, we found that the younger patients in Group 1 who tended to present with BC were less likely to be estrogen receptor (ER) and progesterone receptor (PR) hormone receptors-positive (p=0.0001, p<0.0001) and more likely to be triple-negative (p=0.008). While the old patients in Group 2 were more likely to be ER and PR receptor positive and Her-2/neu negative (luminal A type, p=0.002). Young patients in Group 1 were more in Her-2/neu amplified category (p=0.016). We further analyzed the ER positive and ER negative tumors in both young and old age groups of our cohort with respect to tumor size, tumor grade, lymphovascular invasion, lymph node metastasis, distant metastasis and Ki67 expression. A significant correlation between the ER positive tumors in young patient with high grade tumors (p=0.0001), lymphovascular invasion (p=0.003), axillary lymph node metastasis (p<0.0001), and distant metastasis was observed (p=0.0008). The Ki67 expression in ER positive tumors did not show any significance correlation (p=0.455) (Table 2). While ER negative tumors showed a significance correlation with high Ki67 expression (p<0.0001); however, it did not correlate well with other prognostic markers (Table 3).
- Sub analysis of estrogen receptor (ER) positive tumors with respect to age, tumor size, tumor grade, lymphovascular invasion, lymph node metastasis, distant metastasis and Ki67 expression.
- Sub analysis of estrogen receptor (ER) negative tumors with respect to age, tumor size, tumor grade, lymphovascular invasion, lymph node metastasis, distant metastasis and Ki67 expression.
Discussion
In the current study, young patients (≤40 years) accounted for 24.4% of the total BC cases, which is comparable to other Asian countries, such as China,18 South Korea,19 Iran,20 Pakistan,21 and the United Arab Emirates (UAE).22 However, it is significantly higher than the 3.7%-6.6% reported in many Western countries.4-7
The higher rate of BC in young patients in our cohort is comparable with the previous data from Saudi women reported by Nuzhat et al23 and Elkum et al24 from Riyadh also observed a higher rate of BC (25.2%-33.2%) in young women in Saudi Arabia than the women from the western countries (3.7%-6.6%).
Several studies have shown that in developing countries, BC patients are diagnosed a decade earlier than their Western counterparts.25-27 This could be attributed to several factors, such as differences in race/ethnic backgrounds, genetic susceptibilities, social background factors, dietary habits and lifestyles, environmental factors, and economic development levels between young women in developing countries and their counterparts in developed countries. However, data in this realm are lacking. Moreover, the young age pyramid could be an additional factor that explains the higher frequency of early onset BC in the developing countries compared to developed countries. According to the data available from the Saudi General Authority for Statistics, women under 40 years of age represent 74.6% of the total female population in Saudi Arabia.28 This is about 1.5 times higher than that of the USA for the same age group (74.6% versus 51.2%), indicating a relative over-population in the young age group in Saudi Arabia, and thus an increase in the incidence of BC in young Saudi women compared to their American counterparts.29
Histopathological analysis showed that both the young and elderly groups were dominated by IDC without any significant statistical difference in its proportion. We did not find any significance difference in the DCIS and other subtypes of IDCs between the 2 groups, similar observations were noted by Foo et al10 from Singapore and Telfah et al11 from Jordan. Interestingly, our patients in Group 2 showed statistically significant number of ILC, a similar finding was observed by the various previous authors.10-12
In this study, we observed that the young women with BC reported with an adverse clinicopathological characteristics, including larger tumor size, higher grade, advance tumor stage, more lymphovascular invasion, and more distant metastases compared with older women. Similar to our data, the study conducted by Foo et al10 of 843 women with BC from Singapore showed that young patients had a higher tumor grade and vascular invasion compared with older women (p=0.012 and p=0.034).10 Telfah et al11 from Jordan also reported similar results and found that young BC patients had larger tumors (p=0.02), increased lymphovascular invasion (p=0.05), and higher tumor grade (p=0.0001) compared with the disease arising in older patients. In addition, Maggard et al12 from the USA found that young patients were more likely to present with more advanced tumor grades and tumor stages than their older counterparts (p<0.0001 and p<0.0001). Similarly, Bharat et al13 from the USA reported that the young patients with BC in their cohort presented at an advance tumor stage with a higher grade and more lymphovascular invasion compared with aged patients (p<0.05, p<0.01 and p<0.05 respectively).
In our study, ER and PR receptor were negative and Her-2/neu overexpression was noted in majority of the young patients. Similar observations of ER and PR negative tumors in young BC patients were made by Bharat et al13 from the USA. In line with this, Anders et al30 analyzed the microarray data from 784 BC patients, and found that young patients had lower ER and PR mRNA expression, as well as higher HER2/neu expression compared with aged patients. Similarly, Zhang et al31 compared the clinicopathological features of 6,668 cases of young and 143,920 cases of older BC patients, and noticed low prevalence of ER/PR positivity and overexpression of the HER2/neu receptor in young patients compared with older patients. Telfah et al11 also reported similar findings in their study and noticed low prevalence of ER positivity and overexpression of the HER2/neu receptor in young patients compared with aged ones. In another detail study on gene profiling of breast cancer in 3,522 women by Azim et al,32 from Brussel, Belgium where they subclassified their patients in 3 molecular subtypes (ER+/HER2-, HER2+ and ER-/HER2-) and found that young women had a higher percentage of ER-/HER2- cancers (p<0.001). They also found that young women with BC have a unique molecular processes, and cancers in them are augmented with extracellular signal regulated kinases and P13K signaling genes. They also found that BRCA1 germline mutated breast cancers were significantly associated with younger women. Further sub-analysis of ER receptor status of our cohort showed a significant correlation between the ER negative status with young age (p=0.0001), larger tumor size (p<0.0001), high grade tumor (p<0.0001), and high Ki67 expression (p<0.0001). A similar observation of high Ki67 expression by immunohistochemistry and mRNA expression in young patients by Aine et al33 from Lund University, Sweden.
Currently, it is widely accepted that molecular subtyping of BC is considered an important prognostic factor, which influences disease prognosis and the patient’s outcome. The triple negative breast cancers (TNBC) and the BCs with over expression of Her-2/neu behave more aggressively and have a poor prognosis due to the high risk of lymphnode and distant metastasis and recurrence rate, similar observations were made by Ma et al34 from Shanghai, China and Al-thobaity35 from Jeddah, Saudi Arabia. Similarly, Radosa et al36 from Memorial Sloan-Kettering Cancer Center, New York also reported that young patients with TNBC presented with larger tumor size and higher tumor stages. Our findings of significantly high rates of triple negative BC in young women as compared to their older counterparts are in accordance with the previous published research.
Study limitations
The potential limitations of our study are mainly related with the retrospective nature of the study and sample selection from a single tertiary care hospital which might limit the representation of our findings to the general population of the region. Lack of patients’ survival data, physicians’ choice of therapy (breast conservative surgery, mastectomy, radiation, chemotherapy), BRCA gene profiling, family history and recurrence rate, these limitations are mainly attributed to the sample collection from the histopathology laboratory and limited access to the medical record section of the hospital. Another possible limitation is lack of intrinsic subtyping of BC in our cohort which might hinder the prognostic and predictive information. Additionally, the lack of comparative sub analysis based on age and ER status is another possible limitation due to the small numbers of cases in our group.
In conclusion, although BC in young women is uncommon, it may be different with regards to poor prognostic outcomes which is particularly ascribed to more aggressive histopathological features such as higher tumor grade and lymphovascular invasion and less conducive hormonal receptor status when compared to the cases diagnosed in older women. Healthcare professionals should keep the aggressive nature of BC in young patients in their mind while dealing with the breast abnormalities in this age group. We believe that our study provides a baseline tool for future population-targeted studies to analyze the behavior of BC in young patients for developing efficient adjuvant therapies for a better outcome in this population.
Acknowledgment
We acknowledge Scribendi (https//www.scribendi.com), the Editing and Proofreading Services for English Documents for reviewing and editing our manuscript.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 25, 2020.
- Accepted May 30, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.