


Article Figures & Data
Figures
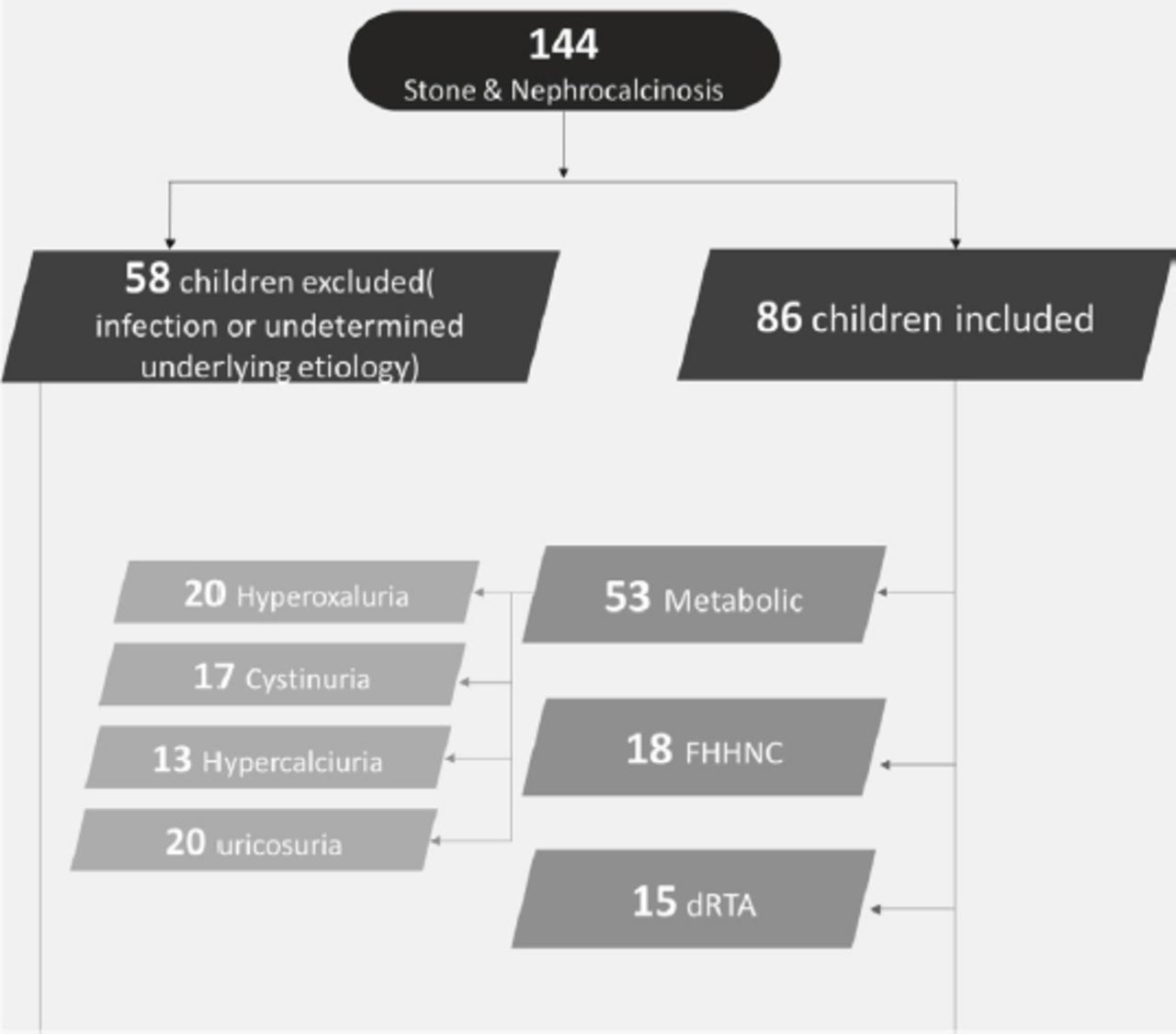
- Figure 1
- A flow diagram showing how patients were assigned to the different groups. FHHNC: familial hypomagnesemia with hypercalciuria and nephrocalcinosis, dRTA: distal renal tubular acidosis

Tables
Characteristics Metabolic FHHNC dRTA n (%) Age (months), mean±SD 73.5±54.4 70.2±43.9 72.6±52.2 Gender Male 32 (60.4) 6 (33.3) 9 (60.0) Female 20 (39.6) 12 (66.7) 6 (40) Creatinine (µmol), mean±SD 103.7±184.9 71.8±48.2 72.7±93.5 Consanguinity* 40 (75.5) 17 (100) 9 (60.0) Family history of renal disease 18 (34.0) 15 (88.2) 4 (26.7) FHHNC: familial hypomagnesemia with hypercalciuria and nephrocalcinosis, dRTA: distal renal tubular acidosis, SD: standard deviation, *35 children of the metabolic group had parents who are first degree cousins, while 5 children with second degree cousins, FHHNC group: 15 children with first degree cousins and 2 with second degree cousins, dRTA group: 8 children with first degree cousins and one with second degree cousin
Characteristics Metabolic Hypercalciuria Hyperoxaluria Cystinuria Hyperuricosuria n (%) Age (months), mean±SD 59.2±57.9 70.6±45.4 91.0±58.3 56.3±75.9 Gender Male 9 (69.2) 12 (60.0) 9 (52.9) 2 (66.7) Female 4 (30.8) 8 (40.0) 8 (47.1) 1 (32.3) Creatinine (µmol), mean±SD 37.2±17.5 178.3±262.6 77.5±130.5 44±26.9 Consanguinity 8 (61.5) 16 (80.0) 14 (82.4) 2 (66.7) Family history of renal disease 4 (30.8) 8 (40.0) 6 (35.3) 0 (0.0) Characteristics Hypercalciuria Hyperoxaluria Cystinuria Hyperuricosuria P-value mean±SD Laboratory urine results (mmol/mmol) Calcium/creatinine 1.59±0.68 1.12±1.57 2.06±6.87 0.84±0.79 0.899 Oxalate/creatinine 0.24±0.02 26.51±67.09 0.03±0.02 0.04±0.03 0.186 Cysteine/creatinine 5.73±4.68 6.21±6.19 132.03±70.60 46.32±63.80 <0.001 Citrate/creatinine 2.92±2.33 7.57±13.83 5.49±6.73 12.19±8.29 0.36 Uric acid/creatinine 0.34±0.19 0.35±0.19 0.40±0.23 2.12±1.34 <0.001 Radiology findings, n (%) Stones 11 (84.6) 16 (80) 17 (100) 3 (100) 0.211 Nephrocalcinosis 2 (15.4) 4 (20) 0 (0.0) 0 (0.0) Stone number, n (%) Single stone 4 (36.4) 4 (25) 4 (23.5) 1 (33.3) 0.860 Multiple stones 7 (63.6) 12 (75) 13 (76.5) 2 (66.7) Stone locations, n (%) Kidney 19 (90.9) 12 (75) 6 (35.3) 3 (100) 0.006 Bladder 0 (0.0) 2 (12.5) 16 (94.1) 0 (0.0) <0.001 Ureteric 2 (18.2) 7 (43.8) 5 (29.4) 0 (0.0) 0.399 SD: standard deviation
Genetic analysis Diagnostic group Metabolic FHHNC dRTA n (%) No test done 36 (67.9) 11 (61.1) 13 (100) Positive results 14 (26.4) 7 (38.9) 0 (0.0) Negative results 3 (5.8) 0 (0.0) 0 (0.0) AGXT gene 11 (78.5) 0 (0.0) 0 (0.0) CLDN16 0 (0.0) 7 (100) 0 (0.0) SLC3A1 3 (21.4) 0 (0.0) 0 (0.0) Genetic analysis Metabolic group Hypercalciuria Hyperoxaluria Cystinuria Hyperuricosuria n (%) No test done 11 (85) 8 (40) 14 (82.4) 3 (100) Positive results 0 (0.0) 11 (55) 3 (17.6) 0 (0.0) Negative results 2 (15) 1 (5) 0 (0.0) 0 (0.0) AGXT gene 0 (0.0) 11 (100) 0 (0.0) 0 (0.0) SLC3A1 0 (0.0) 0 (0.0) 3 (100) 0 (0.0) FHHNC: familial hypomagnesemia with hypercalciuria and nephrocalcinosis, dRTA: distal renal tubular acidosis, AGXT: alanine-glyoxylate and serine-pyruvate aminotransferase, CLDN16: Claudin-16, SLC3A1: solute carrier family 3 member 1, AGXT was homozygous in 9 children and 2 combined heterozygous in 2 children while all mutations of SLC3A1 were homozygous as well as CLDN16 were homozygous in 7 children
Characteristics FHHNC dRTA n (%) Clinical presentation Accidental discovery 5 (29.4) 2 (14.3) FTT 4 (23.5) 12 (85.7) UTI 7 (41.2) 0 (0.0) Hematuria 1 (5.9) 0 (0.0) Loin pain 0 (0.0) 0 (0.0) Urine results FHHNC dRTA Normal range Mean (95% CI) Calcium/creatinine (mmol/mmol) 2.43 (1.62-3.24) 1.51 (0.74-2.28) 1-3 years: >1.5 4-7 years: >1 8-14 years:>0.7 FEMg% (mean) 15.46 (11.09-19.82) 2.52 (1.24-3.79) <5% TRP% (mean) 90.66 (86.48-94.84) 83.66 (76.92-90.41) 78-91% Serum results (mmol/L) Serum sodium 139.3 (138.50-140.27) 140.6 (138.60-142.72) 136-145 Serum potassium 3.87 (3.61-4.13) 3.14 (2.90-3.38) 3.5-5.1 Serum chloride 100.94 (98.88-103.00) 109.53 (105.51-113.54) 98-107 pH 7.48 (7.46-7.50) 7.25 (7.21-7.30) 7.35-7.45 Serum HCO3 (mmol) 29.83 (29.31-30.35) 17.80 (16.21-19.38) 22-26 Serum calcium 2.24 (2.15-2.33) 2.28 (2.22-2.33) 2.12-2.52 Serum phosphate 1.38 (1.21-1.56) 1.25 (0.96-1.53) 0.81-1.58 Serum magnesium 0.54 (0.50-0.59) 0.81 (0.76-0.86) 0.70-1.0 Radiological findings FHHNC dRTA n (%) Stones 0 (0.00) 3 (20.0) Nephrocalcinosis 17 (100) 12 (80.0) Stone number Single stone 0 (0.00) 2 (66.7) Multiple stone 0 (0.00) 1 (33.3) Stone location Kidney 0 (0.00) 2 (66.7) Bladder 0 (0.00) 0 (0.00) Ureteric 0 (0.00) 2 (66.7) FHHNC: familial hypomagnesemia with hypercalciuria and nephrocalcinosis, dRTA: distal renal tubular acidosis, FTT: failure to thrive, UTI: urinary tract infection, FEMg%: fraction excretion of magnesium, TRP%: transtubular reabsorption of phosphate, pH: potential of hydrogen, HCO3: bicarbonate
Item Range (month) Range (year) Cut-off level Ca/creatine (mmol/mmol) 0-12 0-1 2.2 12-36 1-3 1.5 36-60 3-5 1.1 60-84 5-7 0.8 >84 >7 0.6 Oxalate/creatine (mmol/mmol) 0-12 0-1 0.17 12-24 1-2 0.13 24-36 2-3 0.1 36-60 3-5 0.08 60-84 5-7 0.07 >84 >7 0.06 Cystine/creatine (mmol/mol) 0-1 0≥1 85 1-6 53 >6 18 Citrate/creatine (mmol/mmol) 0-60 0-5 0.12 >60 >5 0.08 Uric acid/creatine (mmol/mmol) 0-12 0-1 1.5 12-36 1-3 1.3 36-60 3-5 1 60-120 5-10 0.6 >120 >10 0.4
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.