


Abstract
Objectives: To investigate the possible relationship between visceral adiposity index (VAI) and carotid atherosclerosis(CAS) in different genders and age groups in China.
Methods: This study was an observational cross-sectional study and included 1996 participants who were health examination . From January 2018 to June 2019, people over 18 years old who had physical examinations were included in the study. Each participant completed a standard questionnaire, anthropometric measurements, ultrasonic examination, and provided blood samples for biochemical measurements. Regression models were utilized to evaluate the relationship between VAI and the CAS risk. An receiver operating characteristic (ROC) was utilized to predict VAI diagnostic efficacy for CAS.
Results: Adjusting for potential confounding factors, the risk of CAS increases as the level of VAI increases, and the odds ratio (OR) of the upper tertile is 3.09 (95% confidence interval [CI]:1.64-5.82, p<0.001) in female >44 years of age. In females aged >44 years, the AUC of the VAI (AUC=0.610, 95%CI: 0.57-0.65) was higher than body mass index, WC, and HC (AUC=0.538 [95%CI:0.49–0.58], 0.499 [95%CI:0.45-0.54], and 0.526 [95%CI:0.48-0.57], VAI demonstrated a better ability to predict CAS (in females >44 years of age). However, this correlation was not observed in males.
Conclusion: The relationship between VAI and CAS, with gender and age differences. Visceral adiposity index could be selected as new and simple predictors of CAS for females (>44 years of age) in China.
Cardiovascular and cerebrovascular diseases (CCVD) are the second leading cause of death in China. The number of years of life lost each year due to cardiovascular disease (CVD) is >2 years, which negatively affects the population and imposes a heavy burden on society. Atherosclerosis is one of the most important causes of CCVD.1 The carotid artery is superficially located, and carotid atherosclerosis (CAS) is closely related to the occurrence of CCVD.2 Carotid atherosclerosis is a window for the formation and evolution of atherosclerosis in coronary artery, cerebral artery, and other artery.3 Therefore, early detection and prevention of CAS are very important for controlling the occurrence and development of CCVD.
Obesity, has been generally considered to be a key correlate in the pathogenesis of diabetes, hypertension, and CVD.4 Current evidence has revealed that the clinical risk attributable to obesity depends not only on the extent, but importantly, the distribution of the excess adiposity.5 Furthermore, visceral fat accumulation may negatively contribute more to CVD risk than general fat accumulation. Traditional adiposity indices, such as waist circumference (WC), body mass index (BMI), and hip circumference (HC), are common indicators used to evaluate obesity; fat distribution and visceral fat function have not, in large part, been considered.6 A case-control study from Spain reported that BMI is not a good predictor of the risk for myocardial infarction.7
The visceral adiposity index (VAI) was proposed by Amato et al8 in 2010, and combines WC, BMI, and blood lipid levels and indirectly reflects visceral fat function and insulin resistance. Several studies have reported that the VAI is a more accurate indicator than other simple anthropometric measures (such as, WC and HC) in predicting incident diabetes and CVD events.9,10 In addition, Jelavic et al11 and Voglino et al12 proposed that VAI also has predictive value for the prognosis of cardiovascular and surgical patients. However, the relationship between the VAI and CAS in different genders and in specific age groups has not yet been characterized. Therefore, the aim of the present study was to explore the correlation between VAI and CAS in a sample of Chinese males and females and defined age groups, as well as whether VAI can be used to effectively predict CAS.
Methods
This study was an observational cross-sectional study. A total of 1996 participants were enrolled from the Changsha Hospital Physical Examination Center, China from January 2018 to June 2019. The inclusion criteria were: aged >18 years; and those who had lived in the local area for more than 6 months over the past 12 months. The exclusion criteria were: aged <18 years; acute hepatitis, cirrhosis, chronic renal insufficiency, malignant tumors; hormone (glucocorticoid) and lipid-lowering drug use within half a year; patients with mental disorders or cognitive and language communication disorders; and pregnant women.
The standardized questionnaire was used to obtain the basic demographic information, past history, family history, hobbies, eating habits, physical activities and work experience. Anthropometric measurements included body weight, body height, and WC. Body weight and height were measured on an empty stomach via standard methods and each was recorded to the nearest 0.1 kg and 0.1 cm, whereas BMI was calculated as the weight in kilograms divided by the square. The WC was measured twice at 1.0 cm above the umbilicus level during minimal respiration. The HC was measured at the highest point of the hip or the level of the trochanter of the femur. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured using a standardized electronic sphygmomanometer (HEM-907, Omron, Japan). The subjects are instructed to relax and sit still for 5 minutes, keep the air bag at the same level as the right atrium, measure 3 times (with an interval of more than 30 seconds each time), and take the average value. Laboratory examinations, including total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and fasting plasma glucose (FPG) were conducted. Blood samples were collected in the morning after overnight fasting for at least 8 hour. All blood samples collected were measured with the full-automatic biochemical analyzer (AU2700, Olympus, Japan) of the same model in the hospital laboratory.
A color doppler ultrasonic detector was (Logiq700/Logig9, General Electric, Milwaukee, USA) utilized in the present study, and the probe frequency was set at 7-15mhz. The subjects were placed in the supine position. Detection range: bilateral common carotid artery, carotid artery bifurcation, external carotid artery, the beginning of the internal carotid artery. A lateral scan around the vessel wall (in areas free of plaque) was used to measure intima-media thickness (IMT), and to identify the presence of plaque(s). Then, the thickness, upper and lower diameter of the plaque were measured in detail according to the image of the long axis of the vessel. For patients with asymmetrical plaques, lateral detection was performed to determine the maximum thickness of the plaque, and the mean value of 6 measurements was calculated. Arterial Health Package was used in this study. In the 2D gray scale mode, extract the image of the carotid inner intima and automatically measure the intima, adventitia, and plaque boundaries by collecting the original digital audio image, phase analysis, and processing of the original data of the vessel wall radio frequency signal. One of the following conditions is defined as carotid plaque: a) focal structure encroaching into the arterial lumen ≥0.5 mm; b) the intima of the artery thickens by 50%; c) mean carotid IMT ≥1.5 mm.13 According to according to the Mannheim plaque consensus, and related literature, the subjects were divided into 2 groups: the carotid atherosclerosis group (having a carotid plaque or mean carotid IMT ≥1.5 mm) and the control group.14,15 The ultrasound examination in this study was performed by 2 physicians who had been engaged in vascular ultrasound examination for more than 10 years and had vice senior professional title.
Visceral adiposity index calculation method: 8VAI (male)=WC(cm) / (39.68+1.88 × BMI [kg/m2]) × TG (mmol/L) / 1.03 × 1.31/HDL-C (mmol/L; VAI (female=WC(cm) / (36.58+1.89 × BMI [kg/m2]) × TG (mmol/L) / 0.81 × 1.52/ HDL-C (mmol/L).
Related diagnosis/index definition
i) Age: according to the World Health Organization age segmentation standards, divided into the young group (18-44 years of age) middle-aged and elderly group (>44 years of age).16 ii) Criteria for hypertension diagnosis: refer to the 2017 American ACC/AHA Guidelines for Hypertension: SBP/DPB >130/80 mmHg, taking hypotensive drugs,17 or those diagnosed by previous medical institutions. iii) The diagnostic criteria for diabetes: Chinese guidelines for type 2 diabetes prevention and treatment (2017 edition), with fasting blood glucose ≥7.0 mmol/L or previously diagnosed with diabetes in medical institutions. iv) Smoking: smoking at the time of the survey or smoking within 1 year in the past. v) Drinking: drinking ≥3 times/week in the past 6 months. vi) Exercise ≥3 times/week: exercise more than or equal to 3 times within a week (at least 30 minutes each time). vii) High-salt diet: total salt consumption per month (a family)/number of family members/days of the month, and the daily salt intake >6 g was defined as high-salt diet.
PubMed database was used for identification and retrieval the article. This study was approved by the Medical Ethics Committee of Changsha Central Hospital (No2021-S0217) and was in accordance with the Helsinki Declaration.
Statistical analysis
The Stata statistical software (version 13.0, StataCorp, College Station, TX, USA)were utilized to analyze the data. Kolmogorov- Smirnov tests were used to verify the distribution for continuity data (p>0.05, data is normally distributed). The continuous normal distribution data were expressed as mean±SD, and the comparison between the groups was carried out by one-way ANOVA; the continuous non-normal distribution data were represented as median (25 quartiles, 75 quartiles), and the comparison between the groups was conducted via the Kruskal Wallis H test. Categorical data were expressed as percentages and Chi-square analysis was used to compare groups. The VAI was divided into 3 groups according to the 3 tertile. The CAS risk in different VAI groups was analyzed via binary logistic regression. The VAI predictive ability was defined by the area under the curve (AUC) in the receiver operating characteristic (ROC). Comparisons of the AUC between VAI and other adiposity-based measurements (BMI, WC, HC)were conducted by using the z-statistics. A 2-tailed p-value of <0.05 was regarded as statistically significant.
Results
Gender characteristics stratified by VAI
A total of 1999 subjects were included in this study.There were 863 males and 1136 females, and the gender proportion was 0.76:1. The average age of male was 51.46±12.97 years, and female was 50.24±13.54 years. Men and women were divided into 3 groups according to the VAI tertile (Tertile 1-3). In women, BMI, WC, HC, TC, TG, HDL-C, LDL-C, FPG, diabetes mellitus, and smoking were significantly different among the VAI tertile (p<0.05); In men, significant differences were found among the VAI levels with BMI, WC, HC, TC, TG, HDL-C, LDL-C, FPG, diabetes mellitus, and exercise ≥3 times/week (p<0.05) (Table 1).
- Characteristics of patients stratified by visceral adiposity index tertiles.
Relationship between VAI and CAS in different genders
In the adjusted model, VAI tertile 2 (OR=2.16, 95%CI:1.51-3.08) and VAI tertile 3 (OR=2.44, 95%CI:1.50-3.98) demonstrated increased CAS risk in females when compared to individuals within the VAI tertile 1. In contrast, we found no such association in males (Table 2).
- Relationship between VAI and CAS in different genders.
Relationship between VAI and CAS in defined age groups
For aged >44 females, when compared to individuals within the VAI tertile 1 in the adjusted model, the OR of tertile 2 and tertile 3 were 2.42 (95%CI:1.53-3.82) and 3.09 (95%CI: 1.64-5.82), although this trend was not observed in 18-44 years of age. In the adjusted model, the correlation between VAI and CAS was not found in males (Table 3).
- Relationship between VAI and CAS in different ages.
Prediction effect of VAI based on the ROC curve on CAS in different populations
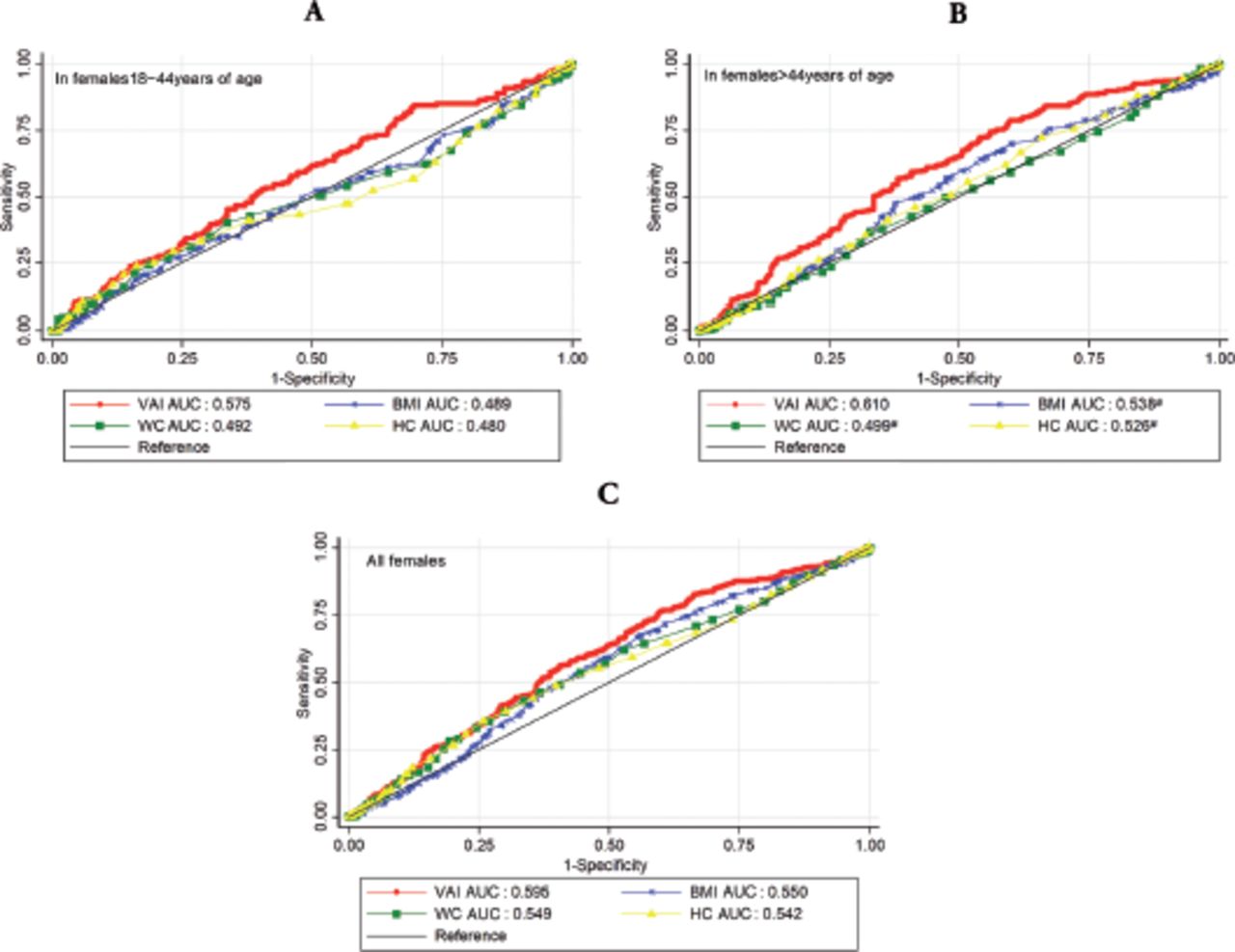
The ability of VAI to predict CAS in different populations was indicated by the area under the ROC curve. For all subjects, the AUC value of VAI was 0.561 (95%CI:0.54-0.59). To understand the VAI predictive effect in different populations, all subjects were further divided into different groups (based on the gender and age). In females, the AUC of ages >44 years were higher than 18-44 years of age, and all females groups. In contrast, the VAI was no found predictive value for CAS in males (Table 4). In order to understand which obesity index has better predictive value for CAS, we compared the areas under the ROC curve. In females aged >44 years, the AUC of the VAI (AUC=0.610, 95% CI:0.57-0.65) was higher than BMI, WC, and HC (AUC=0.538[95%CI:0.49-0.58], 0.499[95%CI:0.45-0.54], and 0.526 [95%CI: 0.48-0.57]), all pairwise comparison between VAI and these 3 indexes indicators was statistically significant (all p<0.001). But, the predictive power of VAI was not superior to other indicators in other subgroup (Figure 1).
- Area under the curve and 95%CI of VAI for identifying CAS by gender and age.

- Receiver operating characteristic of obesity indices (VAI, BMI, WC, HC) comparing the carotid atherosclerosis predictive values A) ROC curves in females 18-44 years of age, B) ROC curves in females >44 years of age, and C) ROC curves in all females. #The differences of AUC between VAI and the index were significant (p<0.001); ROC: receiver operating characteristic, BMI: body mass index, WC: waist circumference, HC: hip circumference
Discussion
In this study, we evaluate the relationship between of VAI and CAS in different genders and defined age groups. In logistic regression analyses, compared to the lowest tertile of VAI, the higher tertile was an independent predictor in women; further subdivided into age group, this trend was found to be highly significant in women >44 years of age; however, this trend was not observed in females 18-44 years of age. In contrast, we found no such association in males. Results of this study revealed the relationship between VAI and CAS, with gender and age differences. The reason for this difference remains still elusive, and it may be related to the different distribution of sex hormones and visceral fat between males and females.18 Frank et al19 showed that age and sex hormones play an important part in the distribution and location of fat. Amdanee et al20 reported that visceral fat increased with age, and adipose tissue was more likely to accumulate in the viscera and abdomen with increasing age
In most population-based studies, BMI and WC were the most commonly used parameters to measure obesity and abdominal adipose tissue. Investigators are interested which of these indicators is a better predictor of fat dysfunction. Our study revealed that, compared with other anthropometric indicators (sucha as: BMI, WC, and HC), VAI demonstrated a better ability to predict CAS (in females >44 years of age), as indicated by the area under the ROC curve. Hameed et al21 proposed that VAI had a good predictive ability to identifying blood glucose control status, compared with other anthropometric measure. A large follow-up study reported that VAI was an independent predictor of renal function decline, which is better than BMI in predicting renal function decline.22 Furthermore, a study from Turkey found that high visceral adiposity was associated with decreased testosterone levels and testosterone/estradiol ratios, and VAI was also considered to be the strongest predictive marker of metabolic syndrome in females with polycystic ovary syndrome.23,24
The association between VAI and CVD is considered to be related to the accumulation of adipokines, oxidative stress, and a proinflammatory milieu.25 Now there are a lot of experimental and clinical evidence that atherosclerosis is a chronic inflammatory process involving many inflammatory cells and inflammatory mediators.26 Accumulation of visceral adipose tissue leads to the accumulation of adipokines; lipoprotein molecules enter the sub-intima of arteries and are oxidatively modified to trigger the production of multiple inflammatory factors (macrophage-enhancing cytokines) and factors leading to oxidative tendencies, which precipitate the occurrence and promote development of atherosclerosis.27 Recently, a cross-sectional study by Klisić et al28 revealed that the phenotype of obesity (such as VAI) was associated with high endocan levels. As a novel inflammation marker, endocan is highly involved in the development of cardiometabolic diseases. Focusing on the distribution of visceral fat may help identify patients with high endocan levels and improve cardiometabolic levels.
In the past 10 years, the overweight and obesity rates of Chinese residents have significantly increased, surpassing those of many other developed countries.29 Obesity, especially visceral obesity, can lead to increased incidence of CCVD, metabolic diseases, and malignant tumors, which has been confirmed by many studies.30,31 At present, computer tomography (CT) and magnetic resonance imaging (MRI) are the best methods for accurately evaluating visceral fat. Research has demonstrated a significant correlation between abdominal visceral fat and arteriosclerosis via CT.32 However, these imaging modalities are unsuitable for the general population or epidemiological research due to their limited availability, time consumption, cost, or radiation exposure hazard. As a mathematical model that includes anthropometric and metabolic parameters, VAI is closely correlated with MRI-measured visceral adiposity, which is a useful indicator of adipose distribution.33 Our study complements and confirms the relationship between VAI and CAS in different genders and defined age groups in the general population. As such, VAI may be used as a simple and effective predictor of CAS in females >44 years of age.
Study limitations
First, although the data of diet, exercise, and work experience were collected, these data were all from self-reported data, which have certain subjectivity. Second, this study was a cross-sectional study, which has certain limitations and cannot verify the causal relationship between VAI and CAS. Finally, some related risk factors, such as endothelial cell function, the economic status of subjects, homocysteine levels were not collected in this study.
In conclusion, the relationship between VAI and CAS was different in genders and defined age groups. Our study has shown that the VAI may be associated with the risk of CAS in females, and it is highly significant in females >44 years of age; VAI predicted carotid atherosclerosis better than other obesity indicators (in females >44 years of age). However, no such value was found in males.
Acknowledgment
We would like to thank www.editage.com for English language editing.
Footnotes
Disclosure. This study was funded by Science and Technology Program Foundation of Changsha (No. kq2004169); the Natural Science Foundation of Hunan Province (No. 2020JJ8044); and the Scientific Research Funds of Health Commission of Hunan Province, China (No. 20201936).
- Received October 9, 2021.
- Accepted December 7, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.