


Abstract
Objectives: To assess the prevalence, awareness, treatment, and control of hypertension in Saudi Arabia.
Methods: We searched electronic databases and the references lists of found publications between 1990 and 2022. Original cross-sectional studies in English were included using PubMed, Google Scholar, and the Saudi Digital Library. A meta-analysis was performed to assess the combined prevalence, awareness, treatment, and control rates of hypertension.
Results: Twenty-nine studies with 278873 individuals aged 14-100 were considered. The pooled prevalence of hypertension was 22.66% (95% CI:18.95-26.60), Cochran’s Q=6221.98, dff=22, p<0.0001; I2=99.65%, Egger’s test (p=0.0033) across 23 studies with 272378 people. The pooled hypertension awareness rate was 42.8% from 6 studies with 36046 participants (95% CI:35.66-50.01), Cochran’s Q=781.86, dff=5, p<0.0001; I2=99.4% and Egger’s test p=0.3772. The pooled proportion of hypertension patients treated in 6 studies involving 46075 samples was 59.4% (95% CI=38.14-79.02), Cochran’s Q=9793.79 dff=5, p<0.0001; I2=99.95%, Egger’s test p=0.8284. The pooled proportion of hypertension-controlled participants across 15 studies comprising 264817 subjects was 34.97% (95% CI: 27.62-42.68), Cochran’s Q=11048.28, dff=14, p<0.0001; I2=99.87% and Egger’s test p=0.9760.
Conclusion: The prevalence of hypertension was high, with low awareness, treatment, and control rates among Saudis. Therefore, policymakers and healthcare providers must work harmoniously to promote health and to prevent, detect, and control hypertension early.
PROSPERO Reg. No.: CRD42023407978
Saudi Arabia has approximately 35 million people (approximately half of whom are under 25 years), dispersed across 2,150,000 km2 and 13 directorates (Riyadh is the capital city). It is a rapidly developing country swiftly emerging into the G20’s powerful economies. Consequently, several Saudi Arabians embraced new lifestyles and eating habits. Hypertension is the most widespread chronic public health problem globally, including Saudi Arabia.1
Hypertension leads multiple complications including cardiovascular pathology, stroke, and renal failure.2 This controllable condition is next to smoking as a cause of mortality from avoidable cardiovascular events.3
Various risk factors are associated with hypertension, including growing older, being male, having fewer years of schooling, and having lower socioeconomic status. A positive correlation exists between overweight and hypertension, whereas being underweight is negatively associated with hypertension.4,5 Diabetic complications with dyslipidemia or low levels of high-density lipoproteins are also risks factors for hypertension.5 Additionally, inadequate intake of fruits and vegetables, high-fat and high-salt diets, and frequent fast-food consumption increased the odds of hypertension.6,7 Also, a link has been identified between physical inactivity, psychosocial stress, and raised blood pressure.7
Hypertension has been associated with an economic loss due to noncommunicable diseases in many countries.8 Furthermore, appropriate hypertension management results in fewer health consequences for patients and a lighter load on the healthcare system. Because hypertension rarely causes symptoms, it is frequently underdiagnosed, undertreated, or poorly controlled. Despite global efforts to manage hypertension in recent years, its frequency among adults has been increasing.
Globally, studies on the prevalence, treatment, and control of hypertension have yielded varying results. Apparently, the variation within regions and countries may be due to diverse age compositions and disparities in resources, education, and access to healthcare.9 Although hypertension is preventable, research has revealed low awareness, treatment, and control.10,11 It is anticipated that the prevalence of hypertension will increase significantly throughout the Middle East.1 This is a major concern and necessitates the development of a presentation strategy by Middle Eastern countries. Emphasizing the critical nature of hypertension management, a drop of 10 mmHg in Systolic Blood Pressure (SBP) reduces cardiovascular complications by up to 30%.12 As a result, a screening program is critical to identify hypertension early, offer treatment options, and assist patients with its management. Over the past 3 decades, several researchers explored various aspects of blood pressure in Saudi Arabia. As the prevalence varies among different settings, a systematic review is required to consolidate and critically assess the findings supplied by these researches. Therefore, this systematic review aimed to gather data and pool the prevalence, awareness, treatment, and control of hypertension in Saudi Arabia during the past 3 decades.
Methods
Following Prisma checklist,13 we performed a systematic literature search using MEDLINE/PubMed, Google Scholar, and the Saudi Digital Library, looking for pre-hypertension, hypertension, high blood pressure, awareness, treatment, management, control, and other related keywords such as cardiovascular diseases, outcome, burden, morbidity, and health need. Studies of participants aged 14 and above were presented in English between January 1990, and December 2022. One investigator performed the searches, and another investigator reviewed the results. We looked through the articles’ cited references to find more related material.
Per the Saudi Hypertension Management Society (SHMS), a SBP ≥140 mmHg, and a diastolic blood pressure (DBP) ≥90 mmHg were taken to diagnose hypertension using a digital automated or mercury sphygmomanometer. Additionally, hypertension can be defined as those on hypertensive medications. Prehypertension is characterized by an SBP between 120 and 140 mmHg and a DBP between 80 and 90 mmHg.
The population was considered hypertension-aware if they had ever had a professional diagnosis of the condition. Finally, a blood pressure reading of <140 systolic and <90 diastolic was considered under control.
Studies that were population-based or carried out in hospitals or primary care in Saudi Arabia were included. We screened all English-language cross-sectional studies examining pre-hypertension, hypertension, awareness, treatment, and control rates. We excluded studies that did not fulfill the hypertension definitions of 140/90 mmHg, those on non-systemic hypertension (secondary or pulmonary), or os special groups such as diabetics, pregnant, and children). Self-reported diagnosis and convenience studies that did not use random sampling were excluded. Also, we excluded editorials, comments or letters, qualitative data, conference abstracts, proceedings, audits, opinion pieces, reviews, case reports/series, methodological and intervention studies, animal studies, and articles missing essential data or not explicitly described. After removing duplicated studies, 2 investigators (SA and HA) independently looked at the eligibility of the paper’s titles, abstracts, and full text to be part of the current review. The most updated paper was considered when numerous publications utilized the same data. Disagreements were resolved through discussions between reviewers. Finally, we performed a quality evaluation to finalize which papers should be in the meta-analysis.
The following information was extracted: research variables: investigator, year of collection and publication, location, and sample size; participants’ age, gender, and setting; and prevalence of pre-hypertension and hypertension and the rate of awareness, treatment, and control. All studies considered >140/90 mmHg as hypertension based on the mean of 2 or more blood pressure measurements using a mercury sphygmomanometer or aneroid device and measured by trained professionals.
The extracted data was presented in a spreadsheet. Two researchers (HS and SA) checked out the titles and abstracts. Furthermore, we assessed full texts for eligibility of the retrieved articles for inclusion. The methodological quality of the papers was analyzed using the Joanna Briggs Institute criteria. There are 4 possible answers to each question: “yes”, “no”, “unclear”, and “not applicable”. The study received one point for each affirmative response. A total score for an article can range from 0 to 9. The overall quality was evaluated using the following rubric for this review: “low” at <6 points, “fair” at 6–7, and “good” at 8–9. Two investigators (AA and HA) independently carried out quality assessments. Probable disagreements were resolved by the consensus of researchers. The findings were tabulated and illustrated in a Prisma flowchart.
Statistical analysis
The meta-analysis was performed using MedCalc for windows version 15.0 (MedCalc Software, Ostend, Belgium). The meta-analysis in this systematic review was carried out to estimate the combined (pooled) estimate of the proportion (prevalence) of hypertension, the proportion of participants who were aware of hypertension, the proportion of participants who had treatment for hypertension, and the proportion of participants who had controlled hypertension. Forest plots were used to graphically show the pooled prevalence (using both fixed- and random-effect models) of the studies included in the meta-analysis. Heterogeneity in the pooled data was assessed using Cochran’s Q. Moreover, I2 was used to indicate the percentage of total variation across the studies included in this analysis. Cutoff values of I2 >50% were used to rule out higher levels of unexplained variability in effect sizes. The significance of publication bias was assessed using Egger’s test. In addition, 95% confidence intervals were used to determine the precision of the estimates. Forest plots were used to graphically show the results (pooled effects using both fixed- and random-effects models) of the studies included in the meta-analysis. Moreover, funnel plots were used to identify publication bias in the studies included in this systematic review.
Results
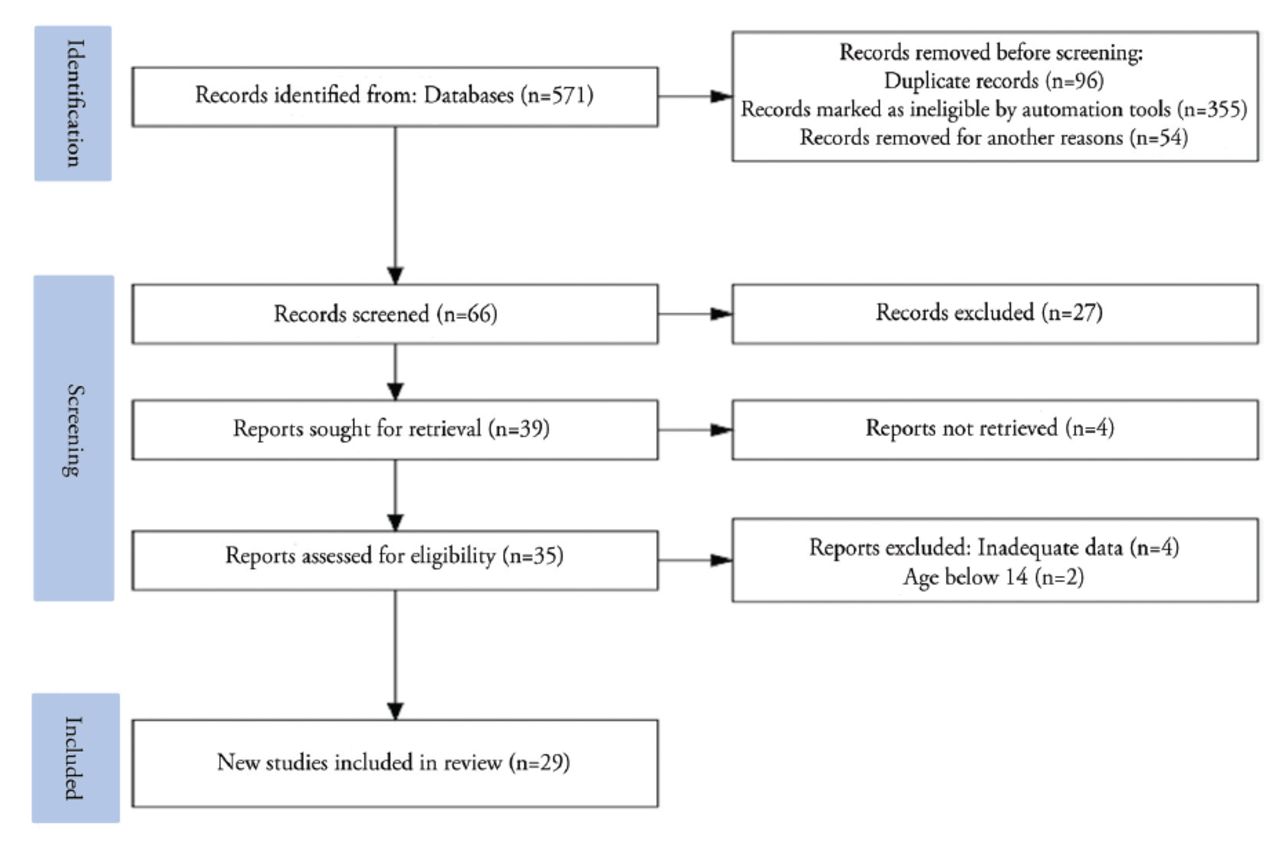
In all, 571 studies were located in the first search. By the end of the second elimination round, 66 records were identified after removing duplicate and non-eligible articles. Furthermore, 39 studies met the eligibility criteria based on study titles and abstracts. We also examined the publications’ complete texts to ensure that they met the criteria outlined in our study protocols. Finally, this review comprises 29 articles. Figure 1 illustrates the Prisma flow chart that summarizes the screening and selection of reviewed hypertensive articles.
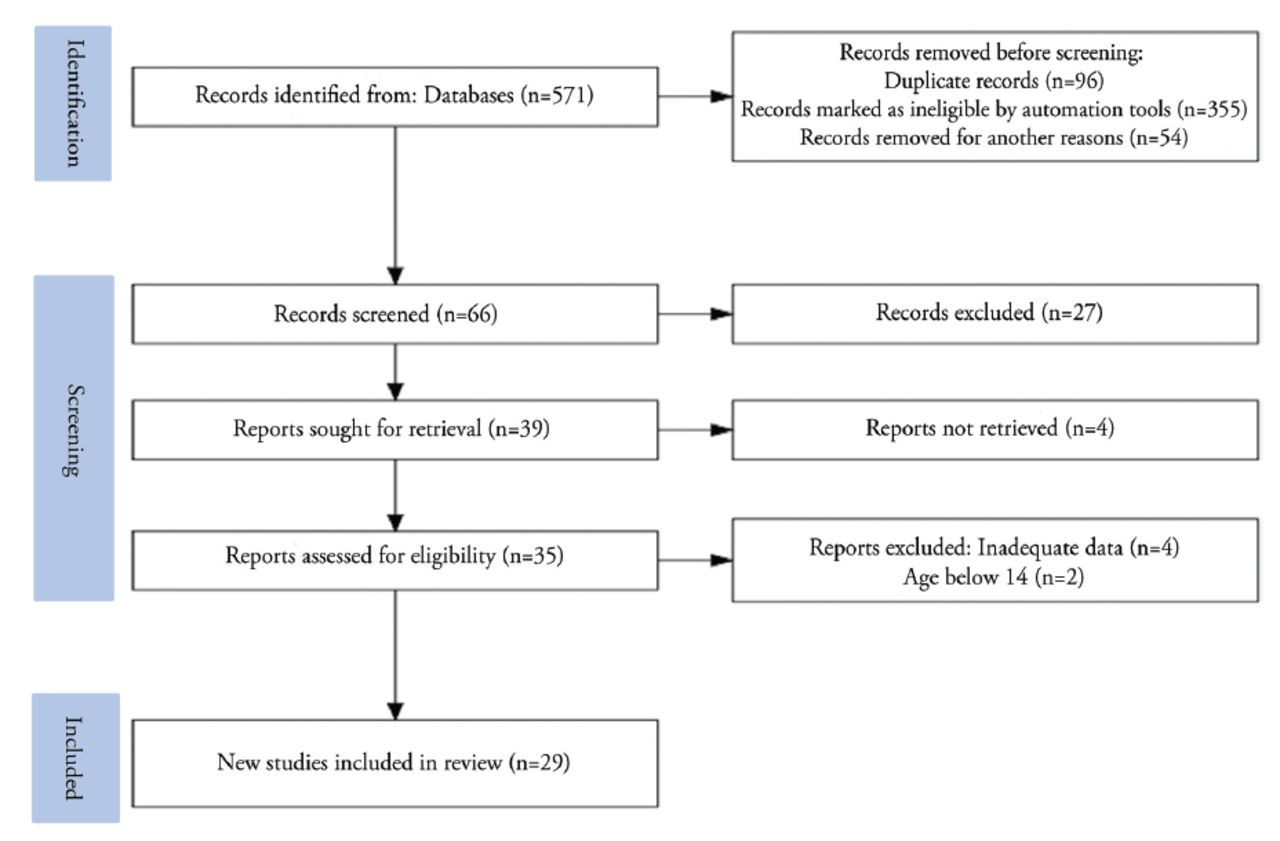
- Prisma flow chart summarizes the search’ screening and selection of the reviewed hypertensive articles.
Trends in research papers published (1990‒2022)
The chronological trends of data collection showed that 4 studies were carried out between 1989‒2000, 9 articles between 2001‒2010, and 13 articles between 1011‒2022. Furthermore, 3 studies did not report data collection dates. The study setting of included articles showed 6 national community studies, 13 regional community studies, 7 studies carried out in regional primary healthcare centers, 2 studies carried out in outpatient clinics affiliated with hospital settings, and 1 study from the Saudi Biobank. Furthermore, 23 studies were carried out during this campaign.
Characteristics of included studies
The features of the included studies, as well as the estimated prevalence of prehypertension and hypertension, as well as the rates of awareness, treatment, and control, are presented in (Table 1). These investigations were carried out in Saudi Arabia between 1996 and 2022. The studies comprised 278873 participants and the number of participants varied from 201 to 197681 with a wide range distribution and reporting, ranging from to 14‒100 years. All studies had an observational cross-sectional design. Most studies (a total of 15) included more female participants than male participants, whereas 9 studies included more male than female participants. Three studies had only male participants, one had only female participants, and one did not report the gender distribution of the participants. There were 8 good-quality articles and 21 fair-quality researches.
- The general characteristics, the estimated prevalence of pre-HTN, HTN, awareness, treatment and control rates of HTN in the included studies.
- The general characteristics, the estimated prevalence of pre-HTN, HTN, awareness, treatment and control rates of HTN in the included studies (continuation).
Prevalence of hypertension
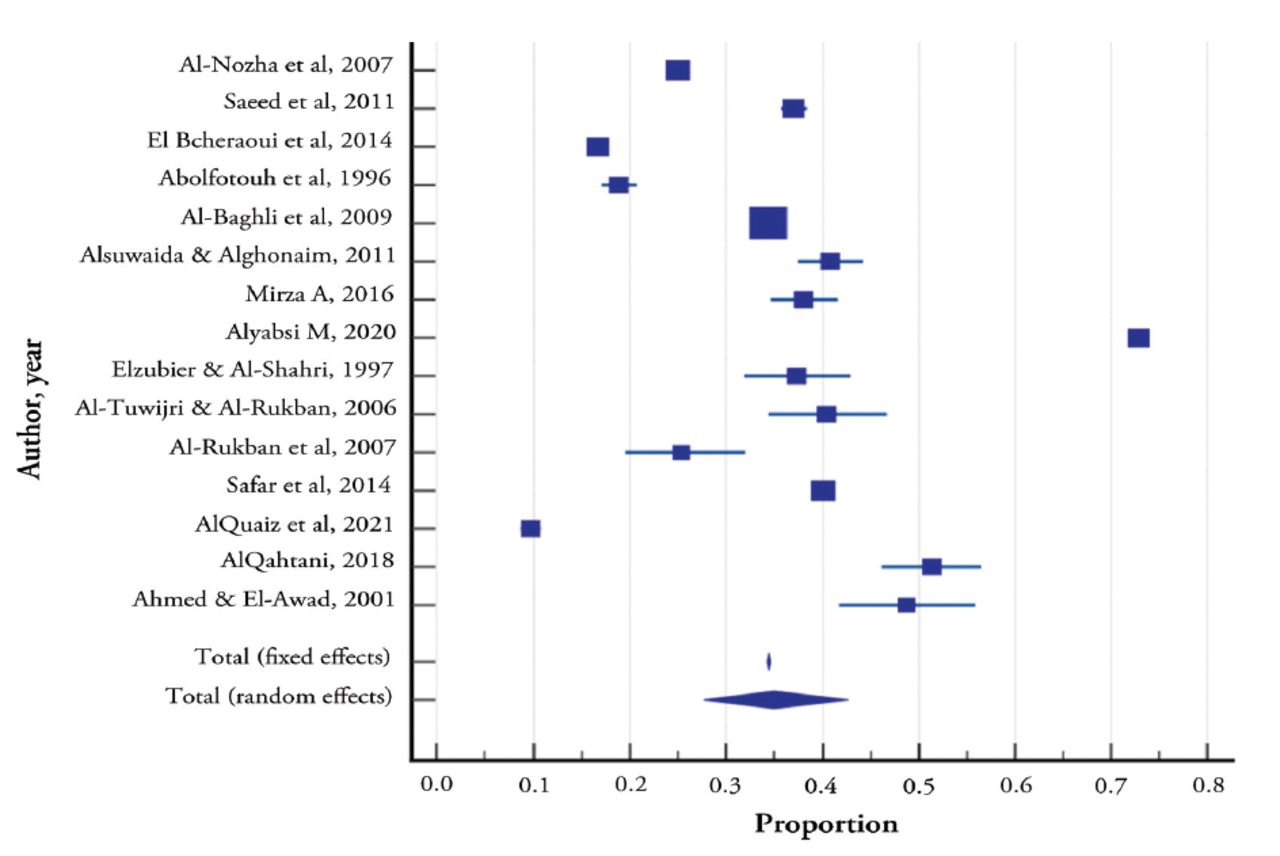
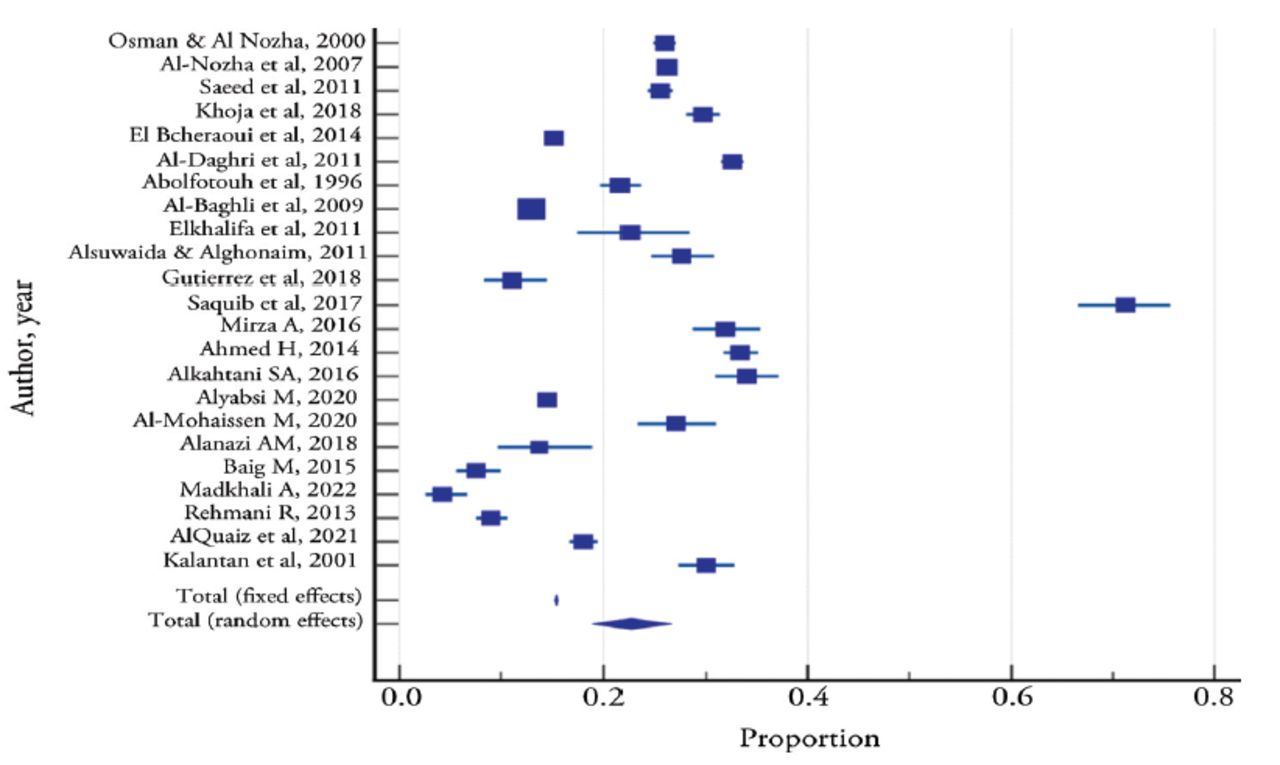
The prevalence of hypertension ranged from 15.2% to 32.6% in national community studies and from 4.2% to 71.3% in regional community studies. The meta-analysis of a categorical outcome variable, prevalence of hypertension, was carried out to assess the combined prevalence rates as obtained from 23 studies. The total sample size of these studies was 272378. The pooled prevalence of hypertension in the random-effects model was 22.7% (95% confidence interval [CI]: 18.95‒26.60). Cochran’s Q (Q=6221.98, (degrees of freedom [dff]) =22, p<0.0001) and I2 (99.7%) were statistically significant, indicating statistically significant heterogeneity across the 23 studies; hence, the pooled prevalence by random effects model was used. Publication bias which was assessed using Egger’s test (p=0.0033), was statistically significant, implying publication bias (Table 2 & Figure 2).
- Meta-analysis for pooled prevalence of hypertension across the published studies.
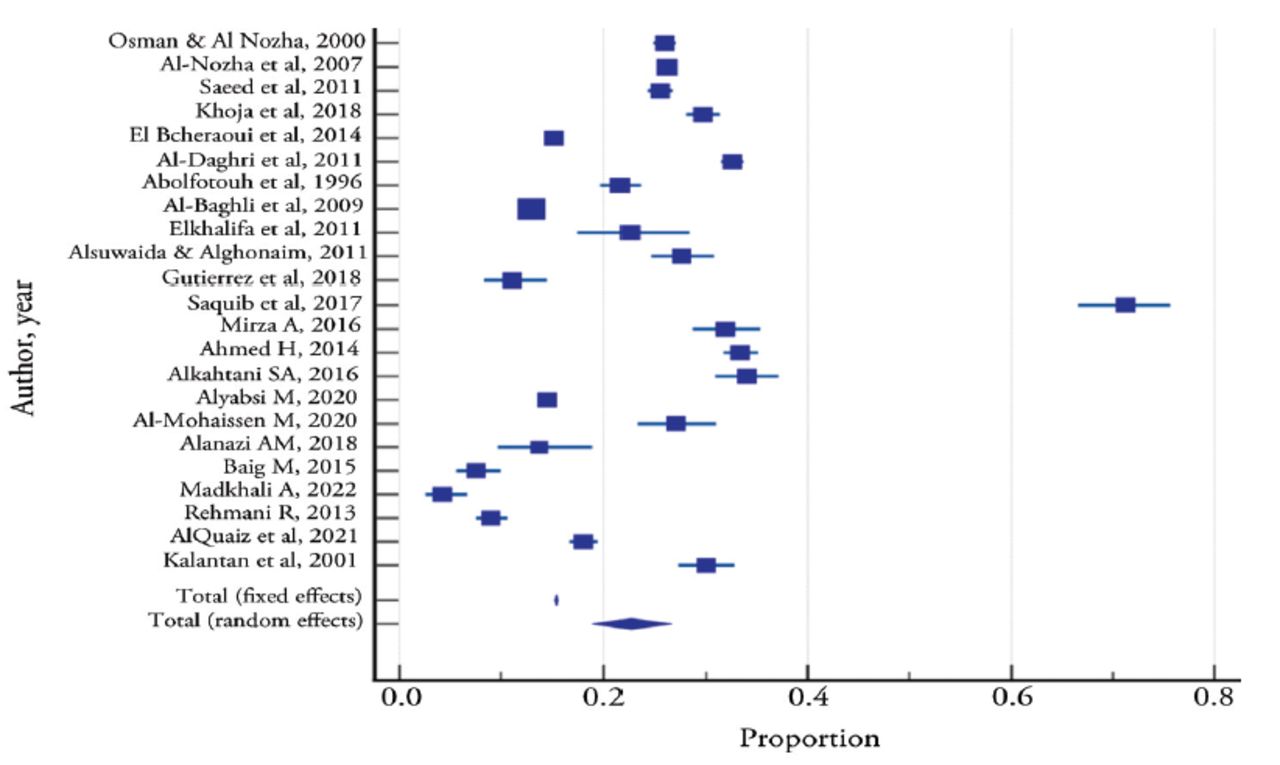
- Forest plot for studies showing the prevalence of hypertension and pooled prevalence.
Awareness of hypertension
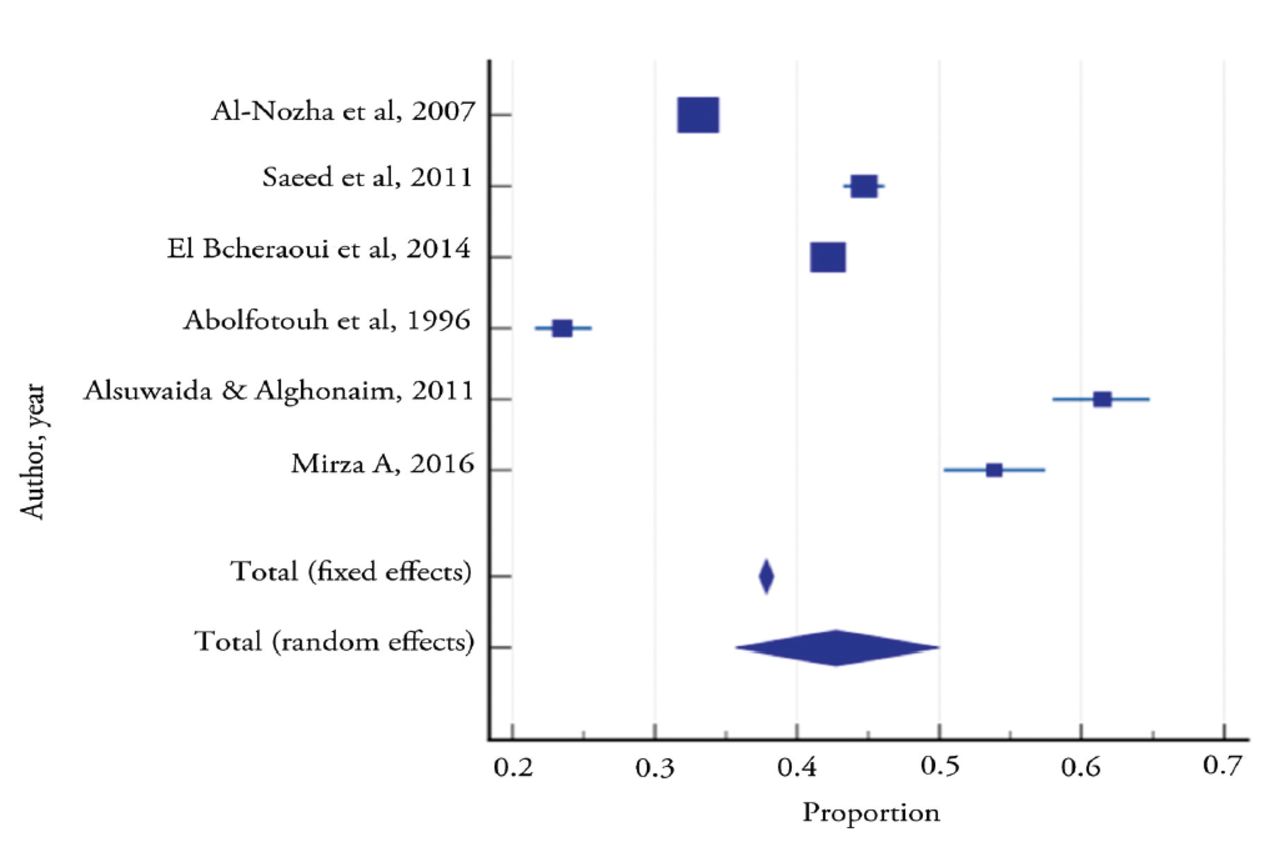
The rate of awareness ranged from 33.1% to 44.7% in national community studies, and from 22.8% to 61.4% in regional community studies. For the meta-analysis on awareness of hypertension, 6 studies with a sample size of 36046 were used to derive the pooled proportion of subjects being aware of their hypertensive condition using the random effect model. It was 42.8% (95% CI: 35.66‒50.01). Cochran’s Q (Q=781.86, dff=5, p<0.0001) and I2 (99.4%) values indicated significant heterogeneity across the 6 studies. None of the 6 papers included revealed evidence of publication bias, as measured by Egger’s test (p=0.3772) (Table 3 & Figure 3).
- Meta-analysis for pooled proportion of subjects who had awareness about hypertension across the published studies.
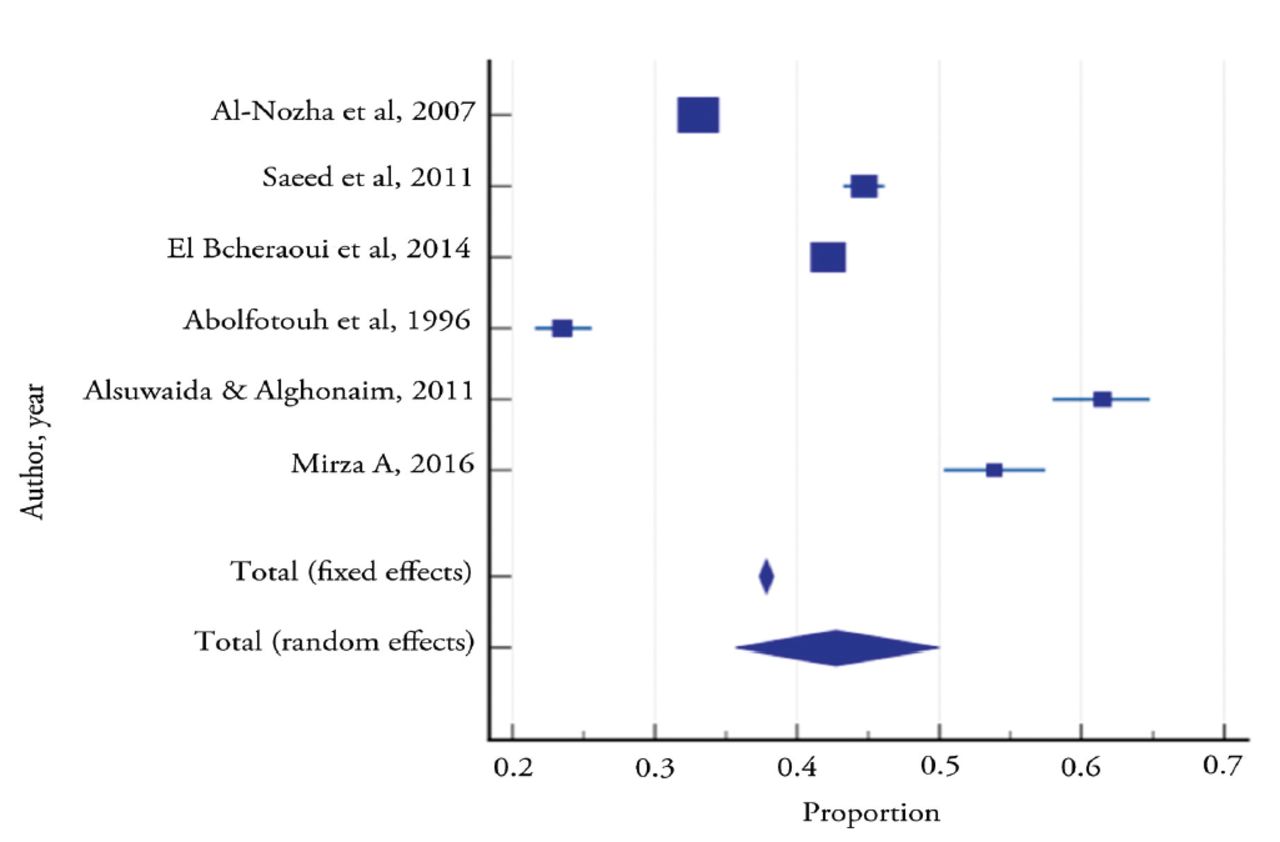
- Forest plot for studies shows the proportion of subjects who had awareness of hypertension and pooled proportion.
Treatment for hypertension
The number of patients with hypertension that received treatment ranged from 36.8% to 75% in national community studies and 6% to 76% in regional community studies. For the treatment of hypertension, 6 studies with a population of 46075 were entered in the meta-analysis to derive the pooled proportion of individuals who had been treated for hypertension. The pooled proportion of individuals who had treatment for their hypertension using the random effect model was 59.4% (95% CI: 38.14‒79.02). Cochran’s Q (Q=9793.79 dff=5, p<0.0001) and I2 (99.95%) values were statistically significant, indicating statistically significant heterogeneity across the 6 studies. There was no publication bias, as the p-value was 0.8284 using Egger’s test (Table 4 & Figure 4).
- Meta-analysis of for pooled proportion of cases who had treatment for hypertension among hypertensive subjects across the published studies.
- Forest plot for studies shows the proportion of subjects who had treatment for hypertension and pooled proportion.
Control of hypertension
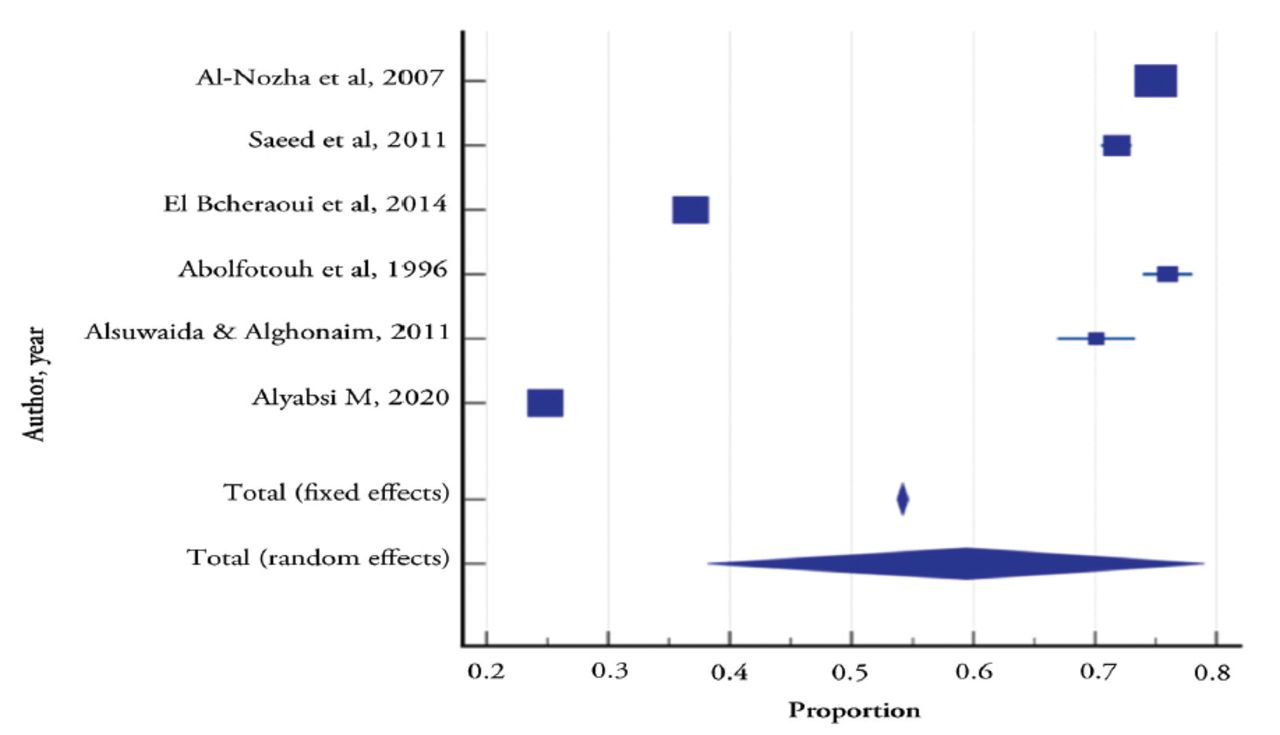
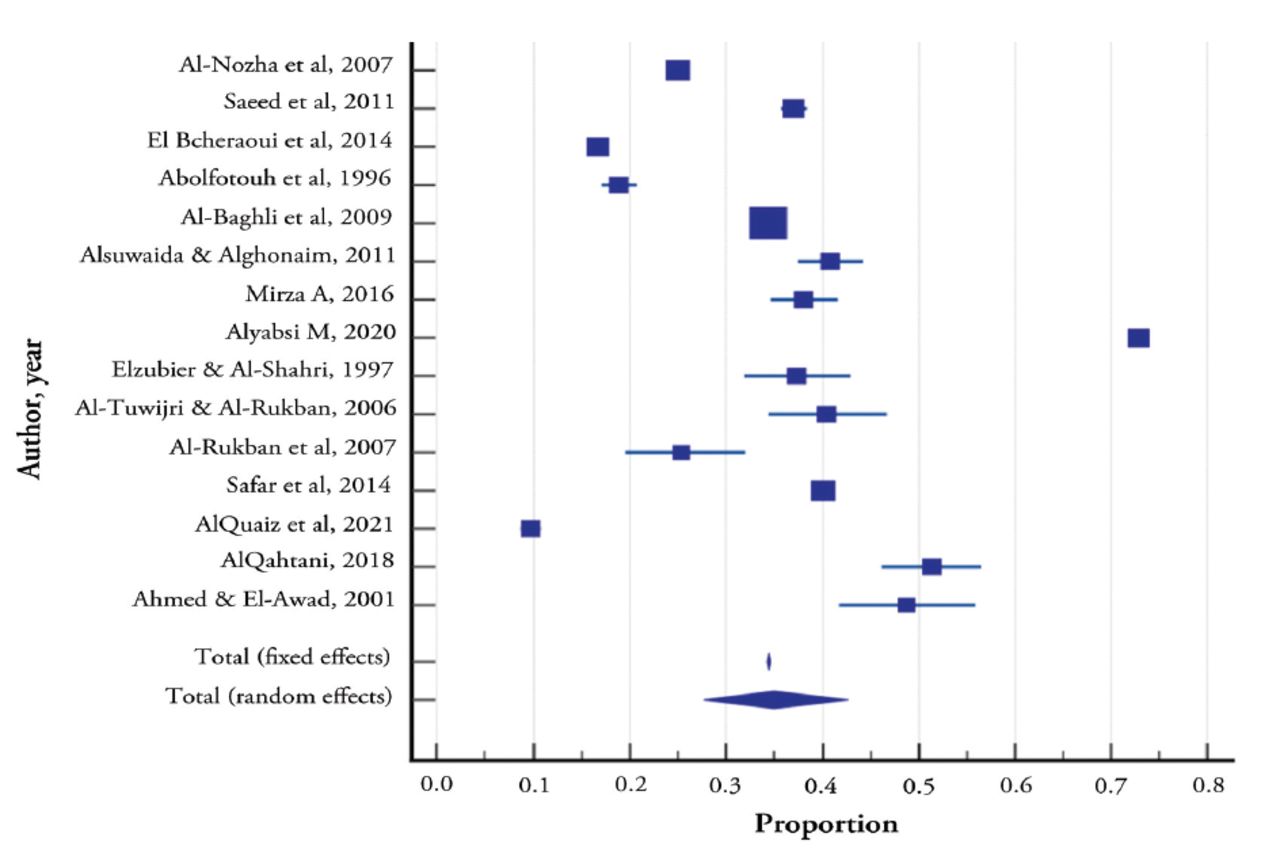
Sixteen studies reported the control status of hypertensive patients on treatment. Hypertension control ranged from 16.6% to 37% in national community studies and from 20.2% to 40.8% in regional community studies. The control rate in primary healthcare studies ranged from 9.6% to 51.3%, while that of hospital-affiliated outpatient studies ranged from 33.6% to 48.8%.
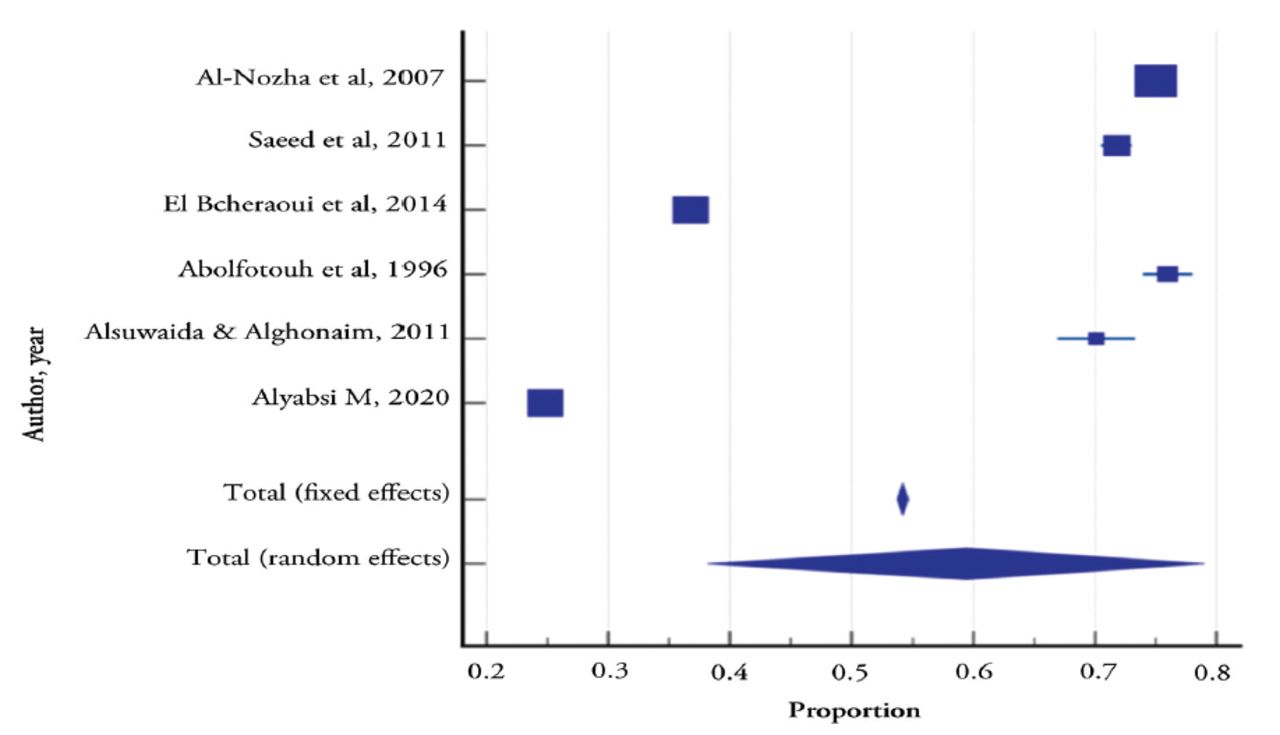
For hypertension control, 15 studies with a sample size of 264817 were used to derive the pooled proportion of individuals who had controlled their hypertension. The pooled proportion of controlled hypertension using the random-effects model was 35% (95% CI: 27.62‒42.68). Cochran’s Q value (Q=11048.28, dff=14, p<0.0001) and I2 (100%) values were statistically significant, indicating statistically significant heterogeneity across the 15 studies. There was no publication bias, as the p-value was 0.976 using Egger’s test (Table 5 & Figure 5).
- Meta-analysis for the pooled proportion of hypertension control cases among hypertensive subjects across the published studies.
- Forest plot for studies shows the proportion of subjects control hypertension and pooled proportion.
There are inherent flaws in the studies included in this review. Hence, a complete meta-analysis was not possible because of inadequate reporting of the measure of association (odds ratio [OR]) across studies.
Age/gender differences
The prevalence of elevated blood pressure in the included studies rises with age. Regarding participants’ gender, 7 selected articles showed more men than women hypertensives, whereas 3 found the opposite.
Risk factors
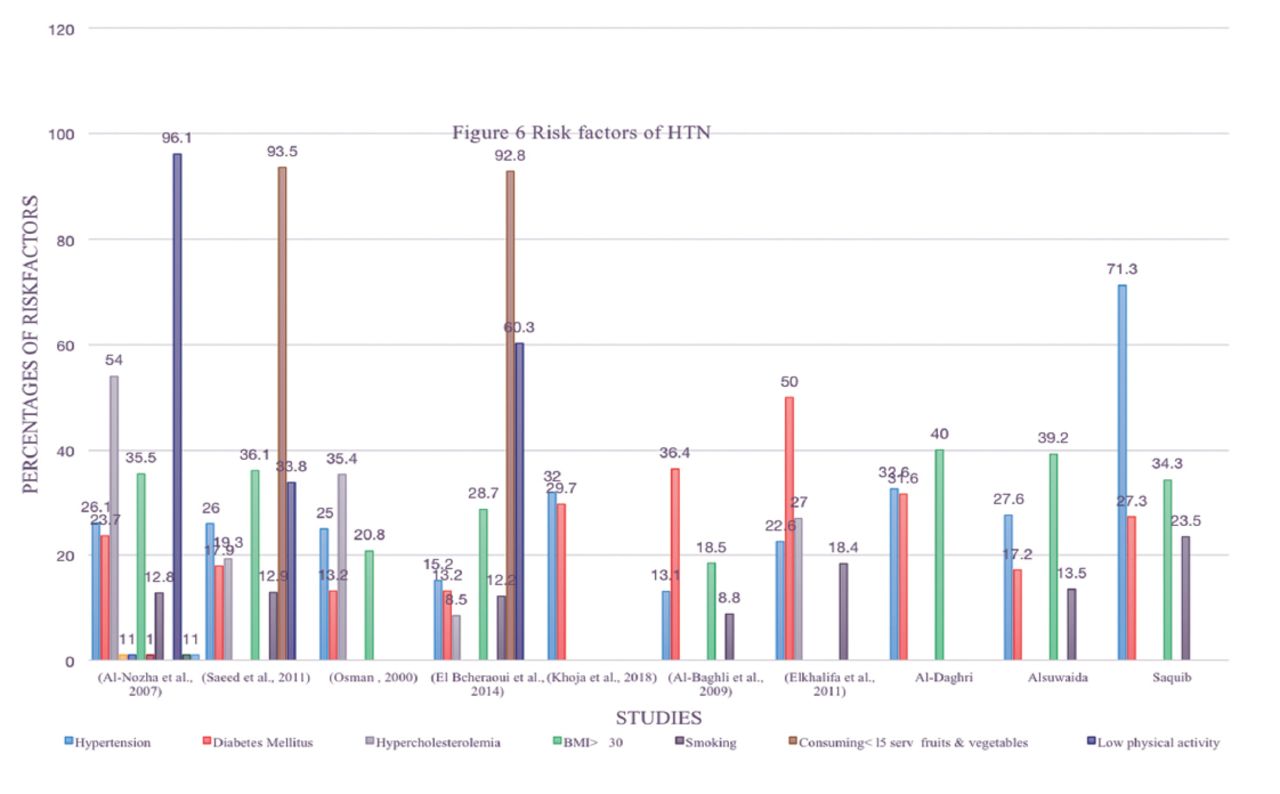
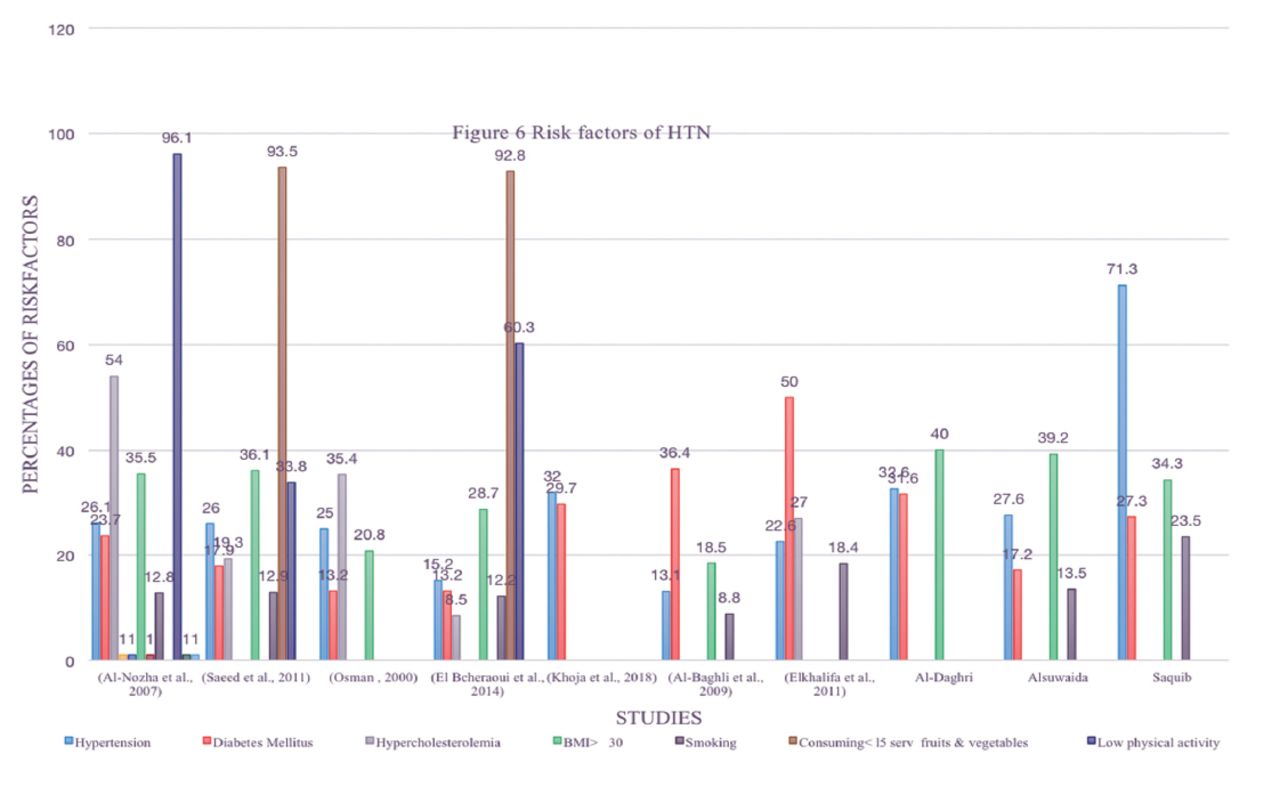
Figure 6 depicts the risk factors for hypertension identified in the reviewed papers. Inactivity and insufficient fruit and vegetable eating were significant risk factors affecting >90% of the participants in some studies. Furthermore, obesity (18.5%‒40%), diabetes mellitus, hypercholesterolemia, and smoking were significant risk factors.
- Risk factors of hypertension.
Discussion
High blood pressure is a common health problem in Saudi Arabia. However, it is not well acknowledged; hence, inadequate control among its population. This is the most updated systematic review and meta-analysis on this topic in Saudi Arabia. Additionally, most of the included studies employed a population-based survey using a random stratified large sampling method from various geographical areas and settings, varying ages, lifestyles, and health status. In addition, there was wide variation in the sample size. Therefore, high heterogeneity was observed in this review. Moreover, small study population and recall bias may have occurred in some studies involving awareness and control questionnaire responses. The articles revealed that trained professionals carried out the interviews, and blood pressure measurements were performed according to standardized blood pressure measurement guidelines using standardized devices.
In this review, hypertension among Saudi 14 year old and above was 22.7% (95% CI: 18.95‒26.60), which is significant. These values were lower than those recorded in the United Arab Emirates (UAE) (24%),14 Oman (41.5%),1 and other Arab nations such as Jordan (33.8%),15 Lebanon (29.3%),4 and the Middle East as a whole (26%).1 However, this prevalence was less than that of the world (32%),9 Korea (30%),16 and Nigeria (38.1%).17
Furthermore, the prevalence was lower than the overall prevalence in high-income countries (28.5 %).2 A review of 12 high-income countries reported a prevalence ranging from 33% in Australia to 34% in Canada to 59% in Finland, the variation is wide for men, and 32.9% in US adults.10,11
The studies included in this review reported that the prevalence of hypertension rises with getting older. This finding is similar to previous research from Jordan15 and Malaysia.18 This age association may be due to atherosclerosis and other cardiometabolic diseases. Furthermore, the prevalence of hypertension was higher in males than in females in most of the included studies, which is consistent with the findings in Lebanon.4 Gender differences in hypertension may be attributed to biological (such as the hormones), behavioral factors (such as smoking) in addition to other risk factors.
However, the level of awareness in this review is still inadequate as it means that less than half (42.8%) (95% CI: 35.66‒50.01) of patients were aware of their elevated blood pressure, and others were unaware and untreated.
Although the obtained results were comparable to those of neighboring countries, they were less appealing than those from industrialized nations. According to study in 12 high-income nations, awareness ranged from 46% in Ireland (men) to 87% in Germany (women).10
In the UAE, 41% were aware of their high blood pressure, and approximately 60% were aware in Jordan.14, 15 In Nigeria, awareness was the highest (62.2%).17 In 6 Latin American countries, 58.9% were aware of their hypertension.19 Our review did not consider gender differences in the rate of awareness; however, the Middle East and North Africa reviews reported that pooled awareness was significantly lower in men than in women1 and similar findings were reported in Malaysia.20
However, 59.4% (95% CI: 38.14‒79.02) were treated for hypertension in Saudi Arabia, which was lower than that obtained from Canada (66% for women and 81% for men).10 However, the percentage of patients on treatment in the present review was higher than that of 6 pooled Latin American countries (53.3%)19, the UAE (23%)14, and Nigeria (40.9%).17
The control of hypertension in our review was 35% (95% CI: 27.62‒42.68), which was less than that in the United States of America (48.2%)11 and Canada (69%).10 However, this rate is higher than that in Nigeria (14%)17, and Oman (34.5%).1
Saudi Arabia has invested significantly in improving healthcare facilities and coverage, with more clinics and hospitals being built throughout the past 3 decades to ensure better access to healthcare in Saudi Arabia, and supported by Saudi vision 2030, which emphasizes health promotion and disease prevention. Therefore, future reviews are expected to reveal improved outcomes.
The articles in the current review did not consistently report known hypertension risk factors such as increased age, male gender, sedentary lifestyle, unhealthy diet, obesity, dyslipidemia, diabetes mellitus, and smoking.
However, many previous studies have associated obesity, independently or through poor nutrition and exercise, with hypertension. Furthermore, diabetes, cigarette consumption, and psychological stress 6,5,21-23 increases the risk of hypertension. Excessive salt intake of more than the World Health Organization (WHO) standard of 5 g/day is another risk factor reported in Saudi Arabia and other Eastern Mediterranean population. Therefore, salt intake must be reduced by 30% by 2025 to achieve WHO targets.7 Fortunately, Saudi vision 2030 includes salt-reduction initiatives.
Control of blood pressure is associated with awareness; hence, being aware of high blood pressure leads to a higher chance of treatment and control. This result agrees with the research carried out across all regions of the world. Inadequate control could be related to insufficient medical treatment, such as pharmacological non-adherence, ineffective prescription, and prevalent lifestyle risk factors. Previous studies found that control of the blood pressure is strongly correlated with subjects’ knowledge on the disease,24 and combined anti-hypertensive treatment.25 Moreover, hypertension is associated with significant burden of inflammation,26,27 hence reduction in inflammatory burden may ease blood pressure control in patients with hypertension.28 We would like also to emphasize the importance of blood pressure measurement at home by automatic devices to achieve blood pressure control.29
Early detection and effective treatment are essential due to the prevalence of hypertension as a risk factor for cardiovascular illnesses. However, high rates of cardiovascular death and morbidity will persist unless these patients are identified. Managing hypertension requires a multifaceted approach that raises awareness, promotes healthier behaviors, and eliminates risk factors. To reduce the total prevalence and mortality associated with hypertension in Saudi Arabia, the healthcare community must work to raise awareness and implement effective means of early identification and treatment. Health campaigns at clinics, hospitals, and community centers are examples of actions that may be carried out to raise awareness.30 Finally, the current findings highlighted the deficiencies in hypertension prevalence, awareness, treatment, and control. Such a situation may encourage all stockholders, such as, patients, clinicians, and decision-makers, to bridge the gap and gain the possible clinical benefits. Management of hypertension is complex and should be approached through multi-sectorial collaboration, primary preventive measures, and improved healthcare accessibility. Steps are being taken to enhance the management and control of hypertension and the SHMS has updated the national guidelines and carried out public awareness campaigns on hypertension.
Study strengths and limitations
Despite the strengths of this review such as the inclusion of several studies with a large population-based survey using a random stratified sampling method from different geographical areas and settings, various generations, range in behaviors and clinical conditions and the assertion that trained professionals carried out interviews and measured blood pressure using standardized blood pressure measurement devices, this study had certain limitations.
First, high heterogeneity was observed among the included studies. Second, it is possible that some respondents to the awareness and control questionnaires were affected by recall bias. Third, some studies did not disclose important variables such as the gender distribution of hypertension. Finally, there were inherent flaws in the studies included in this review; hence, a complete meta-analysis was not possible owing to inadequate reporting of measures of association (OR) across studies.
In conclusion, the studies revealed critical inadequacies in the healthcare of hypertension in nationally, mirroring a similar situation worldwide. Therefore, great strides must be made to educate the public, provide effective care, and keep hypertension under control. Approximately one-fourth of Saudis (aged 14 years and above) are hypertensive, and hypertension is associated with increasing age and male gender. However, only 42.7% of patients with hypertension were aware of being hypertensive, and approximately 60% on treatment. Alarmingly, only around half of individuals who have hypertension are able to keep it under control. These problems can be addressed by systematic ways to screening at various school levels and universities, and pre-employment and pre-promotion to a higher-rank job. In addition, any visitor to a clinical facility, regardless of their health status and purpose of visit, should undergo a blood pressure check. This should be combined with improved patient health education, health promotion, and proper clinical management. Furthermore, other healthcare team members should be involved in these early detection efforts, particularly in family medicine and primary care centers.
Future research implications
The progress in hypertension prevalence, awareness, treatment, and control must be assessed periodically. Future research should also focus on a representative sample using a standard approach to measure blood pressure and associated risk factors, including age, gender, obesity, diabetes mellitus, dyslipidemia, cigarette smoking, and salt intake.
Acknowledgment
We would like to thank Editage (http://app.editage.com/) for the English language editing through Prince Naif Health Research Center, King Saud University, Riyadh, Saudi Arabia.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 25, 2023.
- Accepted March 26, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.