


Abstract
Objectives: To evaluating the predictive significance of the left atrial diameter in acute ST elevation myocardial infarction (STEMI) patients undergoing primary percutaneous coronary intervention (PCI).
Methods: The STEMI population came from 2 retrospective cohorts with 1097 patients, cohorts A (YongChuan Hospital) and cohorts B (Taizhou First People’s Hospital). Within 3 days (cohort A) or 5 days (cohort B) post-PCI, patients underwent ultrasound evaluations. Cohort A was segmented into quartile categories based on eft atrial diameter (LAd) (Q1 to Q4). The odds ratios (ORs) for overall mortality were assessed using logistic regression. Cohort B was used for sensitivity analysis.
Results: During follow-up period, 226 (20.6%) patients experienced endpoint. In cohort A, univariable odds ratios were 2.68 (95%CI 1.11~6.89), 5.32 (95%CI 2.46~12.83) and 11.92 (95%CI 5.78~27.92), while multivariate ORs were 2.25 (95%CI 0.82~6.55), 5.09 (95%CI 2.12~13.56), and 15.05 (95%CI 6.58~39.09) in Q2 to Q4 group, respectively, compared with Q1 group (p for trend <0.001). Upon subgroup evaluation, the correlation between LAd and the likelihood of overall mortality was more pronounced in patients having a left ventricular ejection fraction (LVEF) between 40% and 50%, and those with LVEF ≥50%, in contrast to those with LVEF <40% (p for interaction <0.001).
Conclusion: Left atrial diameter is indicative of the long-term overall mortality risk in STEMI patients post-PCI, particularly in those with an LVEF ≥ 40%.
While percutaneous coronary intervention (PCI) has markedly decreased mortality in acute ST elevated myocardial infarction (STEMI) patients, STEMI continues to be a global issue because of its significant morbidity and mortality.1 Some patients experience adverse events even after receiving appropriate medicines and PCI.2 Early event risk assessment and active intervention can improve secondary prevention strategies and prognosis of the disease.3 Therefore, various clinical risk-scoring systems have been developed, such as GRACE, SYNTAX, Gensini, TIMI, and EUROSCORE. However, these scoring systems are relatively complex and have limited application.
Left atrial diameter (LAd) serves as a simple, convenient, and non-invasive indicator of cardiac structure.4 Its clinical value has been validated in patients with atrial fibrillation (AF). The CODE-AF registration clinical trial shows a 57% greater threat of systemic thromboembolism in the population with an increased LAd compared to the total enrolled population, and a 79% heightened risk of the systemic thromboembolism in such patients receiving anticoagulantsin South Korea.5 A study from Japan also identified a heightened stroke risk in AF patients with an enlarged LAd, as opposed to those with AF and a normal LAd.6
The prognostic stratification value of LAd in non-AF population has also received increasing attention. The result of a meta-analysis involving 91 studies shows that LAd enlargement is associated with the adverse vascular events in both the AF and non-AF populations. Moreover, the correlation is more pronounced in patients lacking AF compared to those with AF, pointing to the potential significance of left atrial myocardial anomalies.7 However, the potential prognostic value of LAd in STEMI patients receiving PCI remains undefined. We hypothesized that LAd could offer valuable insights into the prognosis of STEMI patients post-PCI. We sought to evaluate the associations between LAd and clinical outcomes among STEMI patients undergoing PCI procedures.
Methods
Studies were identified using PubMed and EMBASE databases, MEDLINE, which evaluated the effect of LAd in patients with STEMI and published before March 2023. The following keywords were used: heart atrial, myocardial infarction, prognosis, prognostic value, mortality. References of relevant articles were also reviewed for any additional studies.
This study’s participant pool was sourced from 2 retrospective cohorts, namely cohort A and cohort B. Cohort A included patients with STEMI who were visted to Yongchuan Hospital in Chongqing City, China, from January 2016 to January 2019. Cohort B encompassed STEMI patients visited to the Taizhou First People’s Hospital in the Zhejiang of Province between January 2010 and October 2014.8
Inclusion criteria were all STEMI patients admitted to both hospitals within the initial 12 hours following the onset of chest pain. Diagnosis of STEMI was characterized by persistent chest pain; dynamic electrocardiogram changes and significantly elevated troponin concentrations. Exclusion criteria were severe cardiac valvular heart disease; conservative treatment without PCI; estimated life expectancy <12 months; having a recent cerebrovascular disease within the past year or cerebrovascular disease with significant residual neurological deficits; malignancy; recent serious infection; severe renal insufficiency requiring dialysis; known contraindications to aspirin, statins, contrast agents, heparin, GPI, or clopidogrel or connective tissue disease; gastrointestinal or genitourinary tract bleeding; active major bleeding; history of chronic cirrhosis or liver hepatitis; and lost to follow-up.
Finally, a total of 1097 patients (633 from cohort A and 464 from cohort B) were included in this analysis. All study procedures followed the relevant institutional and national ethical standards and guidelines, including those established in the Declaration of Helsinki (1964) and following amendments. Due to a retrospective design, the informed consent requirement was eliminated. Approval to carry out this retrospective study was obtained from the Local Ethics Committee at Yongchuan Hospital of Chongqing Medical University.
In cohort A, sociodemographic and lifestyle characteristics, medical history and laboratory data were collected upon admission. Dyslipidemia was defined according to guidelines, or receiving lipid-lowering medications. Positive smoking history was defined as being still smoking or quitting smoking for 3 months. After fasting for at least 8 hours, blood samples were collected for assessing the liver function, lipids level by testing total cholesterol, hypertriglyceridemia and fasting blood glucose levels.9 Other immediate laboratory evaluations post-admission included tests for cardiac troponin I (cTnI), white blood cell count (WBC), and B-type natriuretic peptide (BNP). Within three days post-PCI, echocardiography was conducted. Measurements for 2-dimensional (2D) echocardiography and Doppler tests were taken using standard techniques. Transthoracic echocardiography (TTE) was conducted by an echocardiography machine (Vivid E90, General Electric Company, Boston, USA). In 2-dimensional images, LAd was delineated as the distance from the posterior aortic wall to the posterior wall of the left atrium, captured in a parasternal long-axis view at the culmination of ventricular contraction (such as prior to mitral valve opening).10 After discharge, the patients were followed up through out-patient visits or annual telephone. Final patient follow-up was completed in January 2020 with the primary endpoint being defined as all-cause mortality.
In cohort B, the following biochemical parameters were collected on admission: Hb, and PLT, D-dimer and kidney and liver function, myocardial enzymes testing results. Blood lipid and fasting glucose levels were collected the following day. Echocardiography was performed within 5 days after PCI. Two-dimensional echocardiographic and Doppler parameters were measured by previous methods. All patients underwent telephone or outpatient follow-up at least 30 months of after PCI to obtain their major cardiovascular events (MACE) information. MACE was defined as: clinically driven target lesion revascularization, congestive heart failure, recurrent myocardial infarction in a target vessel, or cardiogenic shock, cardiac mortality.
Statistical analysis
Continuous variables were shown as mean and standard deviation (SD), while categorical ones were expressed in percentages. Clinical traits and overall mortality rates, segmented by LAd quartiles (from Q1 through Q4), were compared using the Kruskal-Wallis H test, Chi-square test, or ANOVA as appropriate.
To evaluate the correlation between LAd and outcome events, regression analysis and restricted cubic spline curve analysis were conducted successively. First, with LAd considered as categorical variable (quartile), ranked variable (increase per quartile) and continuous variable (per unit increment) in sequence, four different logistic regression models were conducted to evaluate both univariable and multivariable odds ratios (ORs) for all-cause mortality (95% confidence interval [CI]). Model 0 included LAd without adjustment; while Model 1 was only adjusted for patients’ gender and age; Model 2 was adjusted for age, gender, WBC count, Hb, troponin, and BNP levels; Model 3 was adjusted for age, gender, WBC count, Hb, troponin, BNP levels, and LVEF. Then, subgroup and interaction effects analyses were performed. Finally, Multivariate restricted cubic spline was employed to fit LAd with all-cause mortality in Cohort A and MACE in Cohort B.
To further explore the additional prognostic value of LAd for outcome events, receiver operating characteristic (ROC) curves were generated, with LAd, valuable variables (including age, gender, hypertension, diabetes, WBC, Hb, albumin, cTnI and BNP), LAd plus valuable variable as predictive factors and all-cause mortality in Cohort A and MACE in Cohort B as outcome. All statistical analyses were carried out with R (version 4.1.3) with a significance level of p<0.05.
Results
Baseline of the study population
The clinical characteristics of cohort A according to the LAd quartiles were summarized in Table 1. Cohort A enrolled 633 patients (28.8% women with mean age 70.74 years and mean size of LAd 40.69mm, 71.2% men with mean age 63.64 years and mean size of LAd 40.01mm). The clinical characteristics of cohort B has been published in the original literature.8
- Baseline characteristics of study participants according to the left atrial diameter quartiles.
The clinical characteristics of cohort A and cohort B according to endpoint were summarized in Table 2. During follow-up period, 226 (20.6%) patients experienced adverse event, with 108 (17.1%) patients suffered from all-cause mortality in cohort A, and 118 (25.4%) patients suffered from MACE in cohort B.
- Baseline characteristics of study participants according to the endpoint
Odd ratios for all-cause mortality
In Model 3, post adjustments for factors like gender, age, WBC count, Hb, cTnI, BNP, and LVEF, the multivariate risk ratios for overall mortality in the Q2, Q3, and Q4 groups were 2.25 (95% CI, 0.82-6.55), 5.09 (95% CI, 2.12-13.56), and 15.05 (95% CI, 6.58-39.09) respectively, when compared with the Q1 group (p for trend <0.001) (Table 3). Taking LAd as a ranking variable, a rise by one quartile in LAd corresponded to a 151% escalation in the multivariate mortality risk (OR 2.51, 95% CI, 1.07-1.13). Every single-unit growth in LAd related to a 10% surge in the multivariate mortality risk (OR 1.10, 95% CI, 1.94-3.32) (Table 3).
- Logistic models for the association between left atrial diameter and all-cause mortality.
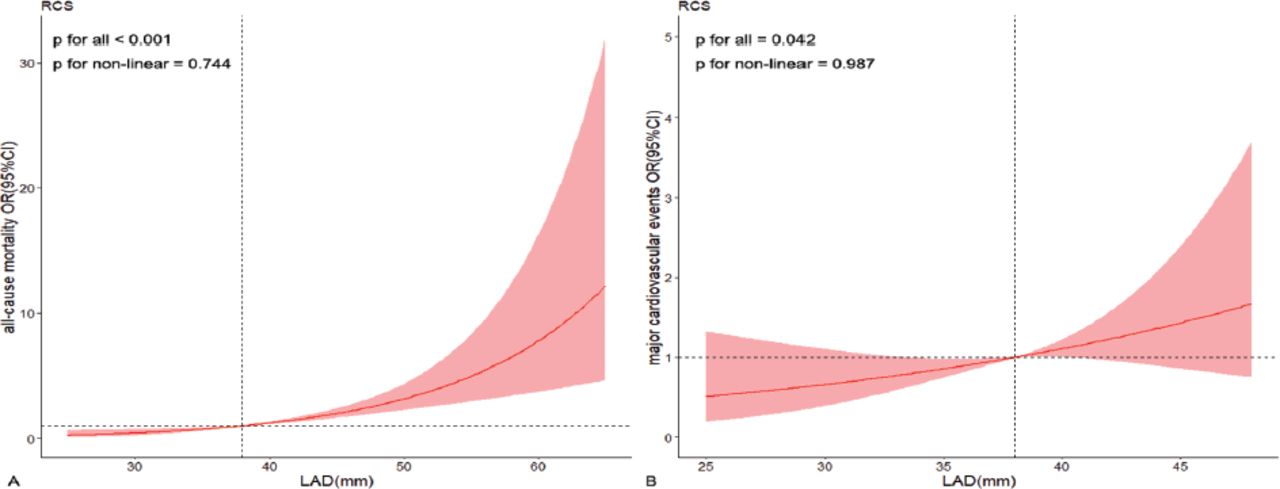
Within the restricted cubic spline regression (RCS) models, the associations between LAd and overall mortality risk (p for non-linear=0.744) (Figure 1A) and MACE risk (p for non-linear=0.987) (Figure 1B) showcased a linear. Importantly, the threshold values for both models stood at LAd 38 mm.

- Adjusted cubic spline model of the association between left atrial diameter and risk of all-cause mortality (A) and risk of major cardiovascular events (B).
Subgroup analysis subgroup analysis
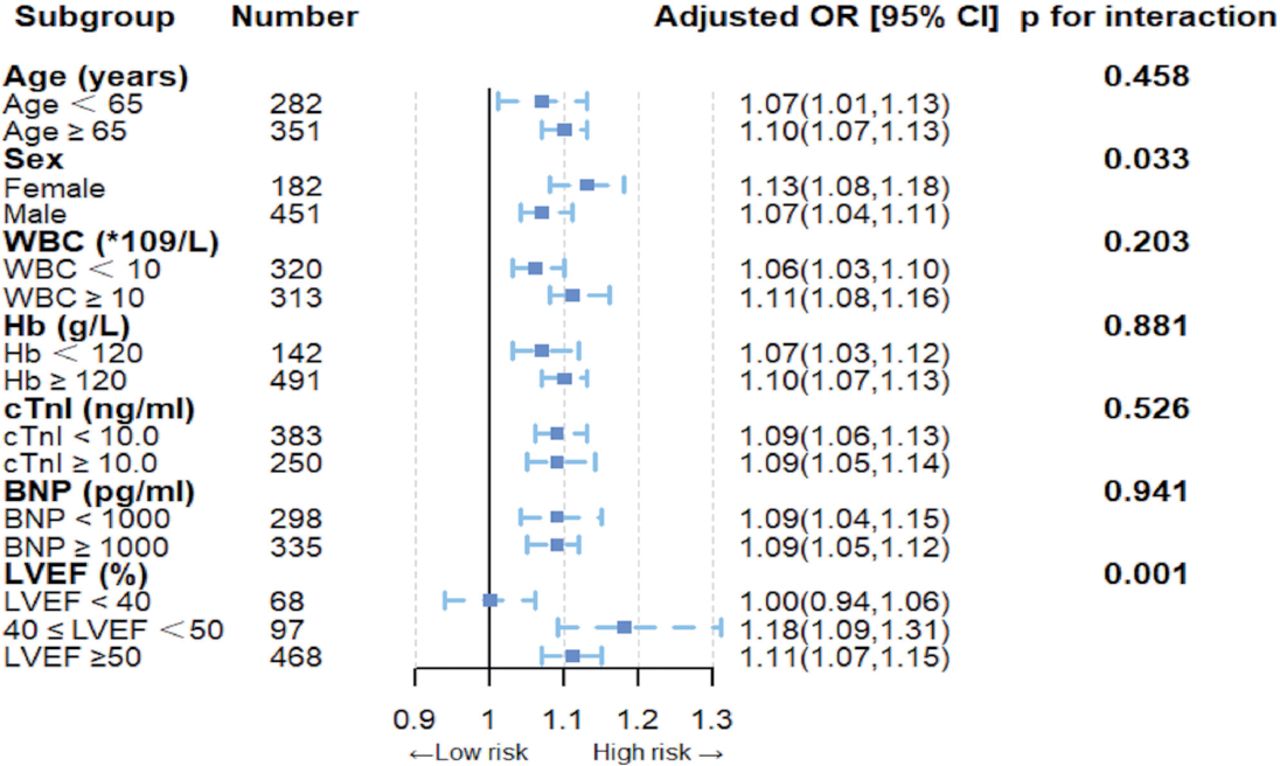
We assessed the link between LAd and overall mortality across subgroups characterized by factors such as age, gender, WBC count, Hb concentrations, cTnI, BNP, and LVEF. Tests for interaction were also conducted (Figure 2). An interaction emerged between gender and LAd concerning the overall mortality risk (p for interaction=0.033). Notably, this association was more pronounced in male patients than in females. Additionally, an interaction between LVEF and LAd was observed for the overall mortality risk (p for interaction <0.001). This association was particularly potent in patients having a LVEF between 40% and 50%, and those with LVEF ≥50%, as opposed to those with LVEF <40%. This positive correlation remained consistent in patients with different levels of ages, WBC counts, Hb, troponin and BNP levels.

- Odd ratios and error bars delineating 95% confidence intervals from Model 3 by subgroups. Multiplicative interaction terms for each subgroup were performed, gender subgroup and left ventricular ejection fraction subgroup were statistically significant (p<0.05).
Additional prognostic value of LAd
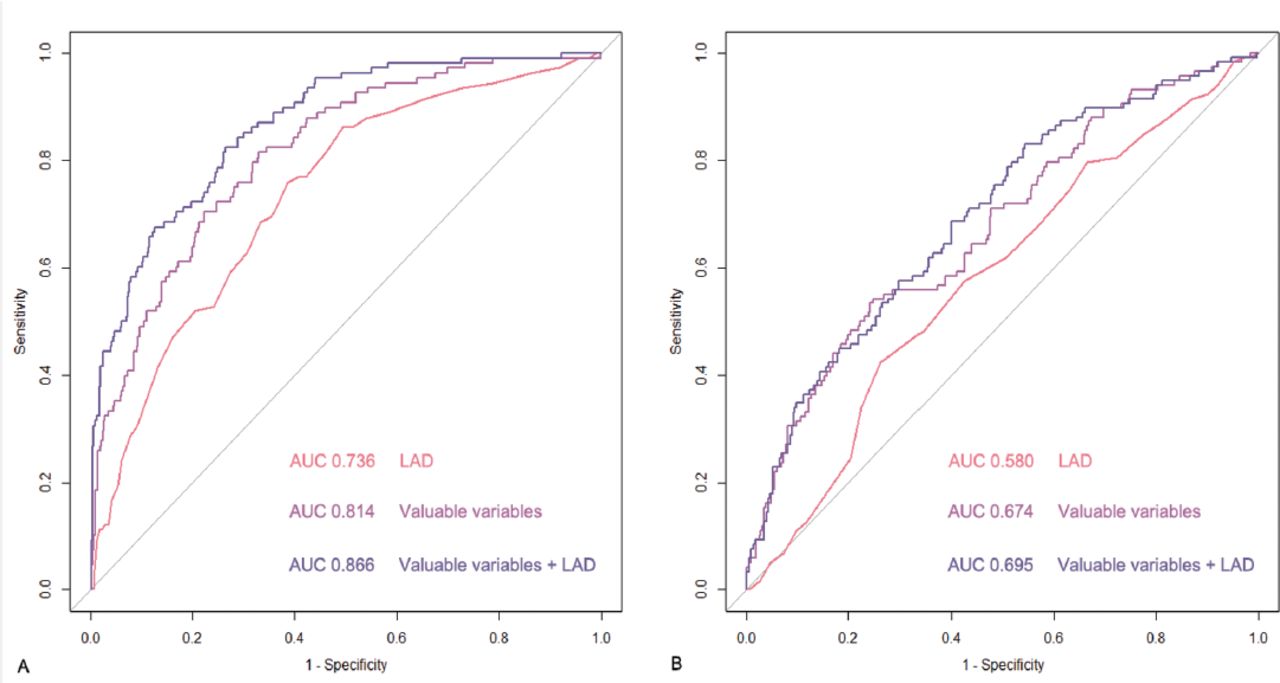
The analysis of ROC curves demonstrated that the inclusion of LAd could significantly enhance the prognostic value on the basis of other valuable variables. In cohort A, the area under the curve (AUC) increased from 0.814 to 0.866 (Figure 3A, p<0.001), while in cohort B, the AUC increased from 0.674 to 0.695 (Figure 3B, p=0.036).

- Receiver operating characteristic curves of LAd, valuable variables (including age, gender, hypertension, diabetes, WBC, Hb, albumin, cTnI and BNP), LAd plus valuable variable for predicting all-cause mortality (A) and major cardiovascular events(B).
Discussion
In our research, we probed the relationship between LAd and the extended prognosis for STEMI patients post-PCI. The results indicated that patients exhibiting an enlarged LAd had an elevated risk of all-cause mortality, and a greater LAd value was found to be an independently predictor of increased long-term all-cause mortality.
An increase in LAd is perceived as a marker of heightened LV pressure and compromised left ventricular diastolic function.10 The prognostic stratification values of the left atrial (LA) structure and function in patients with cardiovascular diseases have gradually attracted attention.11 Transthoracic echocardiography has been widely used in the evaluation of cardiac structure and function, due to its non-invasive, economical, excellent operability and repeatability. It has become a routine method for the LA assessment. While left atrial volume (LAv) or LAv index are considered the standard metrics for assessing left atrial function, LAd continues to be utilized in some large databases and epidemiologic studies for its feasibility and recorded in the routine echocardiographic examination report. Studies also show that LAd measurements can accurately estimate LAv values.1,12,13 In addition, the LAvI assessment is not easily available (almost 1/3 of patients cannot be accessed); therefore, LAd is more practical.5 Based on the above findings, research involving LAd demonstrates that an increased LAd acts as an independent prognostic factor for the onset of atrial fibrillation, the emergence of heart failure, and adverse cardiovascular events.14-16 Nonetheless, definitive evidence regarding the prognostic value of LAd in STEMI patients remains lack. In this study, the LAd was successively divided into categorical variables, ranked variables and continuous variables for analysis. The results showed that an increase in LAd was strongly associated with the all-cause mortality in STEMI patients after PCI, which was consistent with the results of previous relevant work.17,18 After adjusting for potential covariates, our findings indicated that for every standard deviation (SD) increment in LAd, there was a corresponding 10% rise in the risk of all-cause mortality.
In the present study, RCS analysis showed similar linear relationships and identical cutoff values between LAd and both all-cause mortality and MACE. Furthermore, the utilization of ROC curve analysis expanded the analytical breadth of the data, providing additional confirmation from an alternative standpoint that LAd possessed incremental prognostic significance for adverse events in the population with STEMI, in conjunction with other pertinent variables. Given the limitations inherent in observational studies and the constraints of this particular investigation, further research, including randomized controlled trials, is warranted to validate the present findings.
Subgroup and interaction effect analyses showed a more pronounced association between LAd and all-cause mortality risk in men than in women (p for interaction=0.033), and sensitivity analyses provided results consistent with this (p for interaction=0.043), suggesting that gender differences may affect the interpretation of echocardiography in prognosis. In previous studies, the left atrial metric, namely global longitudinal strain, emerged as a strong prognostic factor of individual cardiovascular complications and overall mortality within the broader populace. Interestingly, gender influenced this prognostic value.19 Our results align with these findings. The different prognostic values of LAd in men and women may be due to differences in age, with the average age of women in this study being significantly higher than that of men. The possible mechanism for this difference is still unknown and may be related to gender hormones or life style.
Notably, the link between LAd and overall mortality risk was notably stronger in patients within the 40% ≤LVEF <50% bracket or those with LVEF ≥50% compared to their counterparts with LVEF <40% (p for interaction <0.001). The association between reduced LVEF and poor prognosis in STEMI patients after PCI has been previously demonstrated.20 Our research identified a meaningful statistical relationship between LAd and overall mortality among patients in the 40% ≤LVEF <50% category and those in the LVEF≥50% group. This emphasizes the greater value of LAd in the prognostic stratification for patients with LVEF≥40%. One explanation for this phenomenon is LA remodeling is closely related to the LA function. After STEMI, part of the LV and LA myocardium loses its ability to move in unison, and the LV and LA ejection fraction EF dramatically reduced. When LVEF is greater than 40%, the LA can effectively supple the LV function. However, when LVEF is less than 40%, the LA compensation ability could not compensate for the decline of the LV function. This observation aligns with Ahmet’s study, which highlighted that while the left atrial’s contribution to LV output per beat in healthy individuals stands at 20%, this figure escalates to 35% in STEMI patients with an LVEF averaging 49.4 ± 7.1%.21 This perspective is further reinforced by the evident LA dysfunction in both HFrEF and HFpEF (HF with preserved EF) patients compared to normal controls. Notably, this dysfunction is significantly tied to mortality solely in the HFpEF group (LVEF≥40%).22
Unlike ventricular muscles, atrial myocytes are more vulnerable and sensitive to pathological stimuli. LA remodeling reflects structural and electrophysiological changes in atrial tissue, most commonly due to an overload of capacity or pressure.23 Left atrial remodeling is a highly complex pathophysiological process that involves oxidative stress, microRNA, calcium overload, or inflammation, atrial dilatation, and myofibroblast activation.24 At present, relevant literature has shown that angiotensin converting enzyme inhibitors and angiotensin receptor antagonist therapy can reverse LA remodeling and improve the LA function, which further illustrates the importance of accurate and repeatable LA quantification in clinical practice.25 We believe that this strategy will play a more prominent role in the gradual optimization of secondary prevention strategies for STEMI patients.
Study limitations
There had four limitations in this research. First, it was a post-hoc analysis from a retrospective single-center cohort study with inevitable selection bias or regression bias.26 However, we performed sensitivity analysis on a population from another center to compensate for this selection bias as much as possible. Second, some variables including the valvular disease and diastology were unavailable in both cohort A and B, which makes further studies necessary for deep analysis. Third, the accuracy of left atrial diameter measurement could be one of the limitations due to the retrospective nature. Fourth, adopting a holistic revascularization strategy correlates with a reduced threat of cardiovascular death in STEMI patients presenting multivessel lesions.27 Revascularization strategy was not included in this analysis, which could affect the robustness of the results, and a more comprehensive cohort population is needed in the future.
In conclusion, our research highlighted that a rise in LAd acts as an independent indicator of long-term all-cause mortality in STEMI patients post-PCI, notably among males and those boasting an LVEF≥40%. It is imperative that future multi-center investigations corroborate these observations.
Acknowledgment
We would like to thank Taizhou First People’s Hospital, China, for providing the data and the patients for participating in this study. We also would like to thank Elsevier for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 14, 2023.
- Accepted October 17, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.