


Abstract
Objectives: To investigate the safety and feasibility of subcutaneous implantable infusion ports in repeated hepatic arterial infusion chemotherapy (HAIC) for advanced hepatocellular carcinoma (HCC) in China.
Methods: A total of 237 patients who were clinically diagnosed with advanced HCC (CNLC III a/III b) in our hospitals from December 2020 to October 2022 were retrospectively analyzed. The approaches of HAIC were divided into 2 groups: arterial infusion port implantation (group A) and one-time femoral artery catheterization (group B) based on the physicians’ suggestion and the patients’ intention. The comfort level (evaluated with the General Comfort Questionnaire), complications and average inpatient expenditure were compared between the 2 groups.
Results: 116 patients were finally enrolled in the study (group A: 69; group B: 47) and completed HAIC (FOLFOX-4 regimen) according to the dosing schedules (mean: 6±1 cycles). The comfort level of group A was greater than that of group B (p<0.05). The average inpatient expenditure of group A was lower than that of group B (5.4±2.4 vs 10.4±1.9 thousand yuan RMB/cycle, p<0.05). No patients developed port incision infection, hematoma or catheter-related thrombosis in group A, whereas four patients had groin hematomas, one had femoral artery dissection and four had deep vein thrombosis in group B.
Conclusion: Hepatic arterial infusion chemotherapy via arterial infusion ports for advanced HCC decreased complications and medical expenditures and improved patient comfort levels compared with indwelling catheters.
Hepatocellular carcinoma (HCC) is an extremely common malignancies of the digestive system worldwide.1 Only surgical resection and radiofrequency ablation have good clinical efficacy for early HCC. The special biological characteristics of HCC make it more occult. Most HCC patients lose the opportunity for surgical resection because they are already in the middle or late stages at the time of diagnosis, and often present with intrahepatic vascular invasion or extrahepatic metastasis. The Guidelines of the Chinese Society of Clinical Oncology (CSCO): Hepatocellular Carcinoma (2020 edition) and the Standardization for Diagnosis and Treatment of Hepatocellular Carcinoma (2022 edition) recommend transcatheter arterial chemoembolization (TACE) and hepatic arterial infusion chemotherapy (HAIC) are recommended as first-line treatments for advanced HCC in China, although HAIC has not been endorsed worldwide.2,3 Transcatheter arterial chemoembolization is the first choice for the nonsurgical treatment of HCC patients and is currently the most widely applied treatment for HCC, with definite efficacy in prolonging HCC patient survival.4,5 However, TACE has certain limitations, especially for advanced HCC patients with an excessively large tumor diameter or portal vein tumor thrombosis (PVTT).6,7
In contrast, HAIC may provide significant clinical benefit in such patients with PVTT or high hepatic tumor burden. Chinese scholars have carried out numerous prospective, randomized phase III clinical trials on HAIC and have achieved promising results.8,9 Japanese scholars have widely applied HAIC in HCC patients with PVTT and achieved encouraging clinical efficacy.10,11 The most commonly used regimens for HAIC in Japan are low-dose cisplatin (DDP) combined with 5-fluorouracil (5-FU), interferon (IFN) combined with 5-FU, and DDP alone, while in China they are oxaliplatin-based FOLFOX4 [oxaliplatin + leucovorin + 5-FU].10,12,13 The main approaches of administration include one-time femoral artery catheterization and arterial infusion port implantation, each of which has its own advantages and disadvantages. This study focused on the safety and feasibility of the arterial infusion port as an approach for HAIC.
Methods
We retrospectively analyzed the clinical data of 237 patients who were clinically diagnosed with advanced HCC (CNLC IIIa/IIIb) and admitted to our hospitals from December 2020 to October 2022. Final analysis included 116 patients based on inclusion and exclusion criteria. On the basis of the inclusion and exclusion criteria, 116 patients were included in the final analysis. The study involving human participants was reviewed and approved by the ethics committee of Binzhou Medical University Hospital (No. LW-8) according to the principles of Helsinki Declaration.
The inclusion criteria were advanced HCC (child-Ppugh A/B) with a clear clinical diagnosis (pathological diagnosis of HCC or dynamic contrast-enhanced scan showing the enhancement mode of “fast in and fast out”14 + alpha-fetoprotein ≥400 [ng/ml]); age between 35 and 75 years; type I-III PVTT based on Cheng’s classification; serum albumin ≥32 g/L; total bilirubin, alanine aminotransferase, and aspartate aminotransferase ≤5 times their normal values; normal coagulation function; and ability to understand the protocol and signing of the written informed consent form.14 While the exclusion criteria were HCC with extrahepatic metastasis; PVTT involving both the left and right branches of the portal vein; symptoms signs of liver decompensation, including such as esophageal-gastric variceal bleeding or hepatic encephalopathy; other invasive malignant diseases; and disseminated intravascular coagulation (DIC).
The HAIC approaches of HAIC were chosen based on the physicians’ suggestion and the patients’ intention. A total of 69 patients received HAIC via implanted arterial infusion ports (group A), and 47 received HAIC by one-time indwelling femoral artery catheters (group B).
Arteriography of tumor-supplying arteries
After conventional local anesthesia, the femoral artery was punctured using the modified Seldinger technique, and a 4-F catheter sheath (Cordis, Florida, USA) was inserted. The celiac trunk, common hepatic artery, and superior mesenteric artery were super selectively catheterized using a hepatic artery catheter (Terumo, Tokyo, Japan). Arteriography of these arteries was used to identify the trunks of tumor-supplying arteries and confirm the patency of the portal vein system.
Infusion port implantation
Under fluoroscopy, a 5-F infusion port catheter was introduced through a 260-cm guide wire (Terumo, Tokyo, Japan) into the trunk of the tumor-supplying artery or the common hepatic artery (avoiding the right gastric artery and gastroduodenal and right gastric artery). A subcutaneous pouch was made large enough to accommodate the port (Braun, Melsungen, Germany) away approximately 2.0 cm from the puncture site. Then, the distal end of the catheter was tunneled subcutaneously to the infusion port and fixed to the pouch. An angiography was performed to ensure the proper connection between the catheter and port without bending or leakage, as well as the position of the catheters tip (Figure 1). It was necessary to use metal coils (Cook, Bloomington, USA) if placement of the catheter tips into could not avoid the gastroduodenal or right gastric arteries could not be avoided. The catheter was flushed with heparin (Qilu, Jinan, China) and saline (100 U/mL) every 8 hours during the HAIC period and every 3 weeks during the interval period.
Catheter indwelling via the femoral artery
A microcatheter (Asahi, Nagoya, Japan) was inserted into the tumor-supplying artery. The exposed part of the catheter was secured in place with sutures and covered with self-adhesive dressings. It was required for the patients to stay in bed for at least 50 hours with their right thighs straight. The puncture site was bandaged and compressed to reach hemostasis for at least 12-24 hours after the indwelling catheter and sheath were removed.
Chemotherapy regimen
The regimen of FOLFOX4 consisted of a 3-hour continuous infusion of oxaliplatin (Qilu, Jinan, China) (130 mg/m2), a 1-hour continuous infusion continuously of leucovorin (Hengrui, Jiangsu, China) (400 mg/m2), and a 10-min bolus injection in bolus form of 5-FU (Haipu, Shanghai, China) (400 mg/m2), and followed by a 46-hour infusions continuouslycontinuous infusion of 5-FU (2,400 mg/m2) every 3 weeks in all patients. Hydration was performed during the HAIC period to ensure that each patient’s daily urine output was greater than 2000 ml to reduce the nephrotoxicitynephro-toxicity of the chemotherapeutic agents.15,16 In some cases, patients received molecular-targeted drugs in combination with anti-PD-1 (Hengrui, Jiangsu, China) /PD-L1 treatments.
Evaluation of comfort level
The comfort levels during HAIC were assessed by the Kolcaba general comfort questionnaire (GCQ) 3 days after the HAIC procedure for each individual.17 The GCQ contains 4 dimensions and 30 questions: physical (5 items), psychospiritual (10 items), sociocultural (8 items), and environmental (7 items). We use a 4-point Likert scale, with 1 being strongly disagreed with and 4 being strongly in agreement. The higher the score, the more comfortable they patients are.
Comparison of average inpatient expenditure and complications
The average inpatient expenditure was defined as the mean cost of all HAIC cycles. Adverse reactions and complications includedincluding abdominal pain, abdominal distension, vomiting, hematoma, arterial dissection, and deep vein thrombosis (DVT). The lower the inpatient expenditure and complications, the more significant the advantage of the HAIC approach.

- An intraoperative arteriography. A) Angiography via implanted port (white arrow) showing no contrast agent leakage. B) Angiography via implanted port was performed to ensure that the tip of the catheter was located in the trunk of the tumor-supplying artery (white arrow).
Statistical analyses
The Scientific Packages for the Social Sciences for Windows, version 22.0 (IBM Corp., Armonk, N.Y., USA) program was used for this study. Data obtained through measurement were expressed software was used for statistical analysis of the data. Measurement data are expressed as (x±s) and were compared by using the t test. Count data are expressed as (%) and were compared by the χ2 test or Fisher’s exact probability test. A statistical significance level of 0.05 was considered. P<0.05 was considered statistically significant.
Results
The medical records of 237 patients were reviewed retrospectively, and 116 were ultimately included in the final analysis based on standard criteria. Among the included patients, 69 patients received HAIC via ports (group A), while 47 received HAIC via catheters (group B). However, not every patient completed the HAIC dosing schedules, although none of the discontinuation events were related to the HAIC infusion approaches (Table 1).
The levels of total comfort were significantly different between the 2 groups during the HAIC period (p<0.05). Based on the evaluation of the 4 dimensions of the GCQ, a significant difference was observed in the physical (p<0.05) and psychospiritual (p<0.05) dimensions, but not in the sociocultural (p=0.62) or psychological (p=0.48) dimensions (Table 2).
- Comparison of general data and average medical costs.
- Comparison of general comfort questionnaire subscale.
- Comparison of adverse reactions and complications.
Inpatient expenditure and short-term complications
Significant differences in the average inpatient expenditure for each treatment course were noted between the 2 groups (p<0.05). There were also some differences in short-term complications such as abdominal symptoms, vascular injury at the puncture site and DVT, and more details are presented in Table 3.
Discussion
The 2 main administration approaches of HAIC are via a one-time indwelling femoral artery catheter and via an implanted subcutaneous port. Both delivery methods are safe and feasible for HCC patients with advanced stages, and the choice of delivery mode is dependent on the location of the tumor, angiographic characteristics and clinical conditions. It is also important to note that there are some substantial differences between the 2 approaches.
The advantage of the former is that the catheter can be adjusted during periodic chemotherapy based on tumor progression to achieve precise HAIC or TACE.18,19 However, repeated puncture and catheterization may increase the risks of arterial dissection, arteriovenous fistula, and hematoma. It is also required that patients stay in bed for at least 50 hours from the time of HAIC, with a straight lower limb on the catheter side, which results in poor patient compliance and comfort. It is well known that patients with advanced HCC have poor liver function and are prone to refractory ascites and hypoproteinemia.20 In addition, the hepatic synthesis of coagulation factors and the loss of the dynamic balance of anticoagulant proteins increase the risk of deep vein thrombosis (DVT) during the bed-rest period.21 The 2 groups did not differ significantly in terms of bellyache and hiccups during the same HAIC regimen treatment despite chemotherapy drugs having adverse effects on gastrointestinal function. However, the number of cases of abdominal distention in the catheterization group was obviously greater than that in the infusion port group, which was associated with the patients in the latter group being able to get out of bed early during the HAIC period.
The other approach of HAIC, an implanted subcutaneous port, is less complex. The chemotherapeutic agents are placed into a portable electronic drug infusion pump, and the patient can ambulate at any time during the HAIC period, with no immobilization restrictions, substantially reducing adverse reactions such as abdominal distension. Therefore, the physical and psychological scores of the GCQ were significantly higher in the port group than in the catheterization group, and the former patients had a greater level of comfort during HAIC and demonstrated better compliance. The primary expenditure during hospitalization was from the chemotherapeutic drugs, thus mitigating the patients’ financial burden. Hepatic angiography can be performed by an infusion catheter, which has a high-pressure tolerance of up to 325 psi, to confirm tumor progression, and lipiodol hemoembolization can also be performed via an infusion catheter. The port can be removed at any time after adjustment of the therapeutic protocol according to tumor progression.18
Transcatheter arterial chemoembolization has been beneficial to most treated liver cancer patients.6,22 Patients with advanced HCC with thrombosis of their portal veins (PVTT) have complications such as refractory ascites and hepatic encephalopathy, and conventional TACE may further occlude the liver-supplying arteries and exacerbate the disease condition.7 In comparison to TACE, HAIC may provide a greater survival benefit for these patients. He et al12 found a significant difference in the length of the time to progression in the FOLFOX-HAIC group compared to the TACE group (p=0.015), and that the partial remission rate and disease control rate of the HAIC group were higher than those of the TACE group (52.6% versus [vs.] 9.8%, 83.8% vs. 52.5%; all p<0.01) In contrast, a multicenter randomized phase II clinical trial in Japan showed that the median overall survival (OS) of HAIC (cisplatin) combined with sorafenib chemotherapy was lower than that of sorafenib monotherapy (p<0.05).23 Multiple HCC treatment guidelines in China have recommended HAIC (FOLFOX4) as a first-line scheme for patients with advanced HCC who are not suitable for surgical resection or local treatment.24 In the present study, we only focused on the advantages and disadvantages of different HAIC approaches, and the follow-up period was relatively short. Therefore, no further analysis of time to disease progression (TTP), median progression-free survival (mPFS), or OS was performed.
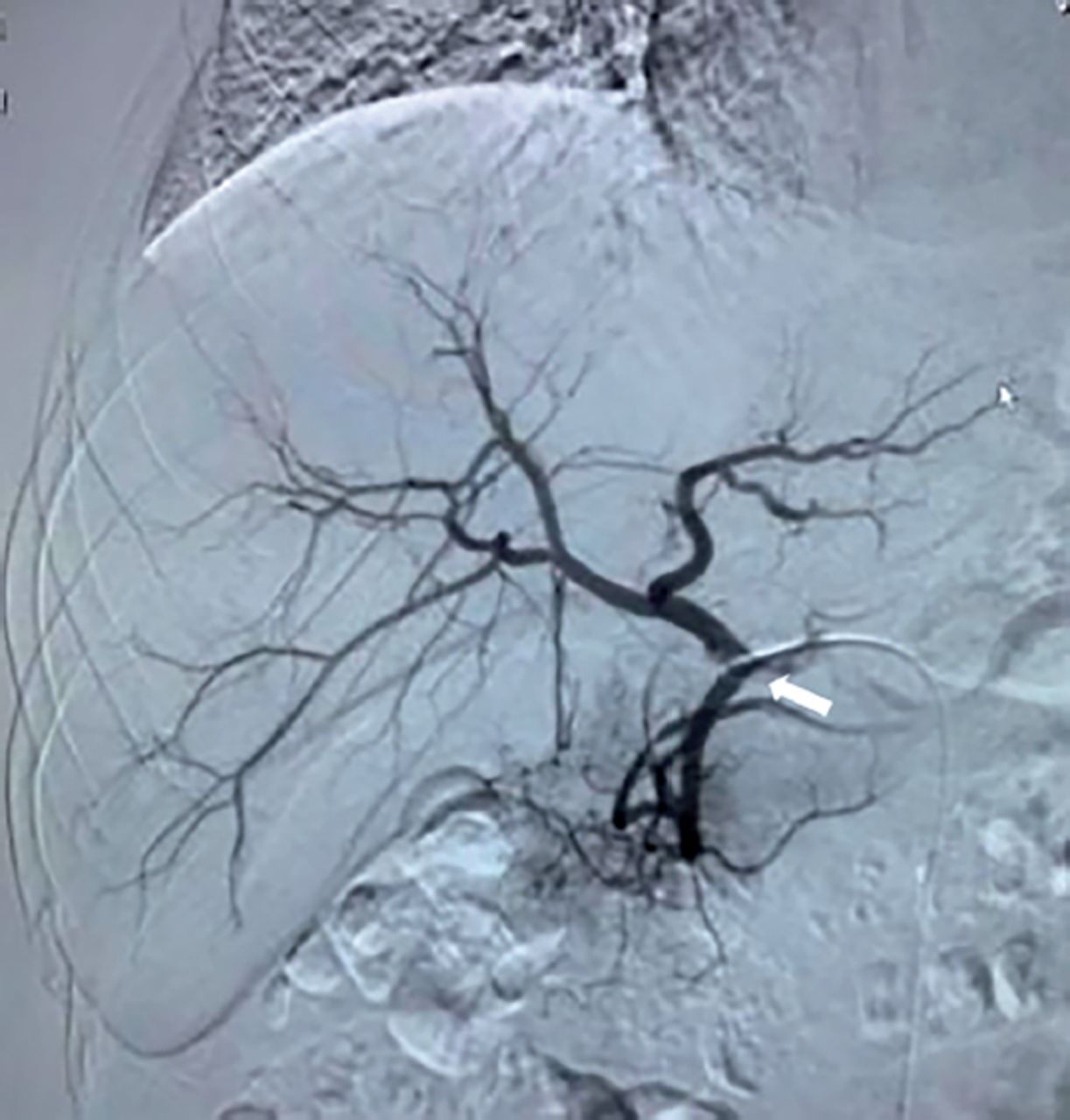
There are relatively few complications associated with HAIC catheters that involve misperfusion.25 Branches responsible for misperfusion mainly included the right gastric artery and gastroduodenal artery (GDA). As a first step, it is important to locate the catheter tip away from the origin of the GDA. Alternatively, endovascular embolization could be considered for the prevention of chemotherapy-induced gastroduodenal toxicity.26 Furthermore, it is crucial to take into account the catheter tip positions during HAIC periods. In this study, one patient who underwent HAIC via a port had upper abdominal pain at the beginning of the second cycle, and the symptoms improved after omeprazole treatment. However, the abdominal pain was aggravated again when HAIC was repeated. Gastroscopy revealed that the mucosa of the gastric antrum and the duodenal bulb were rough, with scattered spotted erythema and erosion. Angiography demonstrated that the indwelling catheter tip had dislodged from the tumor feeding artery and was displaced into the GDA origin (Figure 2). In response to changes in respiratory rhythm and body position after port implantation, the catheter was displaced. In addition, metal coil embolization can be performed in patients with multiple tumor-supplying arteries to redistribute the hepatic arterial blood flow so that only one artery provides blood supply to the tumor.27 Although previous studies found that the arterial infusion port approach can lead to adverse events such as thrombosis and infection, we did not find any adverse reactions in this study. 28,29

- The indwelling hepatic artery catheter is retracted from the proper hepatic artery to the initial segment of the gastroduodenal artery (white arrow).
Study limitations
The present study mainly focused on the analysis of the advantages and disadvantages of different HAIC approaches, and the follow-up period was relatively short. Therefore, no further analysis of TTP, mPFS, or OS was performed. However, it does not affect the validity of the findings on HAIC approaches in our study.
In conclusion, HAIC via a subcutaneous infusion port provides more advantages in terms of long-term persistence and repetitive administration for patients with advanced liver cancer, as well as a reduced risk of complications, improved patient comfort level, lower medical expenditures and improved convenience of clinical application compared with one-time indwelling catheters.
Acknowledgment
We would like to thank AJE (www.aje.cn/) for teh English language editing. We are grateful for the support of the Students Innovation and Entrepreneurship Training Program of Binzhou Medical University, Binzhou, China (Grant No.: X202210440409).
Footnotes
Disclosure. This study was supported by the Students Innovation and Entrepreneurship Training Program of Binzhou Medical University, Shandong, China (Grant No.: X202210440409)
- Received August 20, 2023.
- Accepted October 10, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.